
Abstract
Abstract
Oliver, Samuel J., Petra Golja, Jamie H. Macdonald. Carbohydrate supplementation and exercise performance at high altitude: a randomized controlled trial. High Alt. Med. Biol. 13:22–31.—Acute carbohydrate supplementation decreases effort perception and increases endurance exercise capacity at sea level. It also improves laboratory-based endurance performance at altitude. However, the effect of chronic carbohydrate supplementation at altitude, when acclimatization may attenuate carbohydrate effects, achieved doses are lower and metabolic effects may be different, is unknown and was therefore focused on in the present study. Forty-one members of a 22-day high altitude expedition were randomized in a double-blind design to receive either placebo or carbohydrate supplementation. Diet was manipulated with commercially available energy drinks consumed ad libitum throughout the expedition. Participants performed a mountaineering time trial at 5192 m, completed submaximal incremental exercise step tests to assess cardiovascular parameters before, during, and after the expedition, and recorded spontaneous physical activity by accelerometer on rest days. Compared to placebo, compliant individuals of the carbohydrate-supplemented group received daily an additional 3.5±1.4 g carbohydrate·kg body mass−1. Compliant individuals of the carbohydrate supplemented group reported 18% lower ratings of perceived exertion during the time trial at altitude, and completed it 17% faster than the placebo group (both p<0.05 by t-test). However, cardiovascular parameters obtained during submaximal exercise and spontaneous physical activity on rest days were similar between the two groups (all p>0.05 by analysis of variance). This study utilized testing protocols of specific relevance to high altitude sojourners, including the highest mountaineering time trial completed to date at altitude. Chronic carbohydrate supplementation reduced ratings of perceived exertion and improved physical performance, especially during prolonged and higher intensity exercise tasks.
Introduction
However,
In this regard, at sea level acute carbohydrate supplementation is well recognized to increase endurance exercise capacity (Jeukendrup and Jentjens, 2000) and decrease perception of effort (Backhouse et al., 2005). However, at altitude, data on performance benefits of acute supplementation is contradictory (Fulco et al., 2005; Fulco et al., 2007). Length of altitude stay may explain these variable findings, as acclimatization may attenuate benefits of carbohydrate supplementation (Fulco et al., 2007). Nevertheless, such acute laboratory studies have little relevance to multi-day altitude sojourns that are better characterized by performance tasks involving repeated and prolonged bouts of lower intensity exercise.
Consequently, studies investigating the effect of chronically increasing carbohydrate intake on endurance performance are of greater relevance to altitude sojourners. In contrast to acute supplementation, chronic supplementation at sea level reveals very contradictory results, probably because of differences in performance task duration and intensity, and possibly because of different metabolic effects of chronic compared to acute carbohydrate ingestion (Erlenbusch et al., 2005). In any case, chronically increasing carbohydrate intake at altitude is problematic. Carbohydrate supplementation with solid foods is largely unsuccessful at increasing carbohydrate intake (Edwards et al., 1994). One study did successfully increase carbohydrate intake over a 27-day altitude stay but had to resort to enforced feeding of pure liquid diets that would be unpalatable in real-life conditions (Consolazio et al., 1969). Thus, studies that have used more acceptable interventions of supplemental beverages are of particular interest. Askew and colleagues (Askew et al., 1987) determined that participants allocated to a carbohydrate supplementation group for 4 days voluntarily ran 12.5% further than those on placebo, as assessed during daily 2-hour runs. However, whether sojourners completing longer expeditions can carry, prepare, and drink sufficient carbohydrate to achieve minimum doses required for beneficial effects on performance (Jeukendrup, 2004) is not known. Furthermore, whether carbohydrate supplementation benefits maximal and submaximal performance on other more common performance tasks, such as mountaineering capacity, has not been investigated.
Therefore, the aim of this article was to determine the effects of chronic carbohydrate supplementation on submaximal and maximal exercise performance at high altitude. We hypothesized that, at altitude, supplementation with commercially available energy drinks would increase ad libitum carbohydrate intake, resulting in an increased capacity to complete physical exercise, as evidenced by a reduced perception of effort, a decreased cardiovascular strain, an increased ability to complete periods of higher intensity exercise after prolonged, lower intensity tasks, and an increased level of spontaneous physical activity.
Methods
Participants and ethical clearance
Forty-one healthy participants were recruited from the Medical Expeditions 2008 Hidden Valley Expedition to Nepal. Demographic and anthropometric data is provided in Table 1. The study was registered on clinicaltrials.gov (NCT00731510) and was approved by both the North West Wales Research Ethics Committee and the Nepal Health Research Council. All participants provided written informed consent.
Data are means±SD. Statistical significance was determined by independent t tests. AMS score Day 14, acute mountain sickness score (calculated as total Lake Louise score) on the morning of the mountaineering time trial day; AMS score Day 15, acute mountain sickness score on the morning of the high altitude step test day; Vo2max, maximal oxygen consumption at sea level determined indirectly prior to the expedition.
Preliminary measures
Prior to the expedition, height and body mass of the participants were measured, and their age recorded. Body mass index of the participants was calculated and their maximal oxygen uptake (
Trial design and intervention
This study was a prospective, experimental, randomized parallel groups design with outcome measures obtained serially. The allocation to carbohydrate or placebo solution was double-blind; experimenters learned of participants' allocation only after the statistical analysis had been performed on all outcome measures. The allocation ratio to each group was 1:1. As described in detail previously (Macdonald et al., 2009), participants were randomized to receive either 10% carbohydrate (PSP22, Science in Sport, Blackburn, UK) or placebo solution. Carbohydrate was principally maltodextrin, and provided 100 g·L−1 of carbohydrate and 370 kcal·L−1. Placebo solution was composed principally of natural flavorings and aspartame, and its nutrient content was negligible. Solutions were prepared by expedition group cooks and drunk ad libitum either from mugs at meal times or from personal water bottles during the day.
Outcomes
The study design is shown in Figure 1. Three different performance tests were completed by the participants: The primary outcome measure was rating of perceived exertion obtained during a high-altitude mountaineering time trial. The mountaineering time trial was completed on Day 14 of the expedition. On every testing day, acute mountain sickness score was obtained and calculated as total Lake Louise score (Roach et al., 1993) prior to a standard breakfast consumed at ∼0700 h. From a camp located at 4669 m, participants completed an 8 km self-paced walk on snow to the mountaineering time trial location at 5192 m. The walk included 523 m of vertical height gain as determined by global positioning technology (Garmin Etrex Venture). During this walk participants consumed food from a standard lunch pack and supplement drinks ad libitum until they reached the time trial location. Upon reaching the time trial location, blood glucose (capillary ear lobe sample) was determined by a handheld monitor (Accu-Chek, Aviva). Total mass, including clothed body, winter boots, and rucksack mass was then determined for each participant (Seca, Hamburg, Germany). Full mountaineering kit was worn throughout the self-paced walk and preloaded mountaineering time trial, including winter boots and rucksack. The mountaineering time trial started at 5192 m, and finished at 5320 m above sea level. The time trial consisted of a 200 m preload stage, which was a 4 min paced walk at 3 km·h−1, followed by a 400 m maximal effort stage with 128 m of vertical height gain. The preload stage was marked by orienteering markers every 25 m and was paced with a stopwatch to ensure correct speed. Rating of perceived exertion (6–20 scale) (Borg, 1998), heart rate (RS800CX MULTI, Polar, UK) and finger tip arterial blood oxygen saturation (9500, Onyx, Nonin, MN) were obtained in the final 25 m of the preload stage, thus when steady state had been achieved. The maximal stage was marked every 100 m to provide feedback of distance completed and time to complete the stage was recorded. Weather conditions for the time trial were +10°C, light winds, zero precipitation, and compacted snow underfoot.
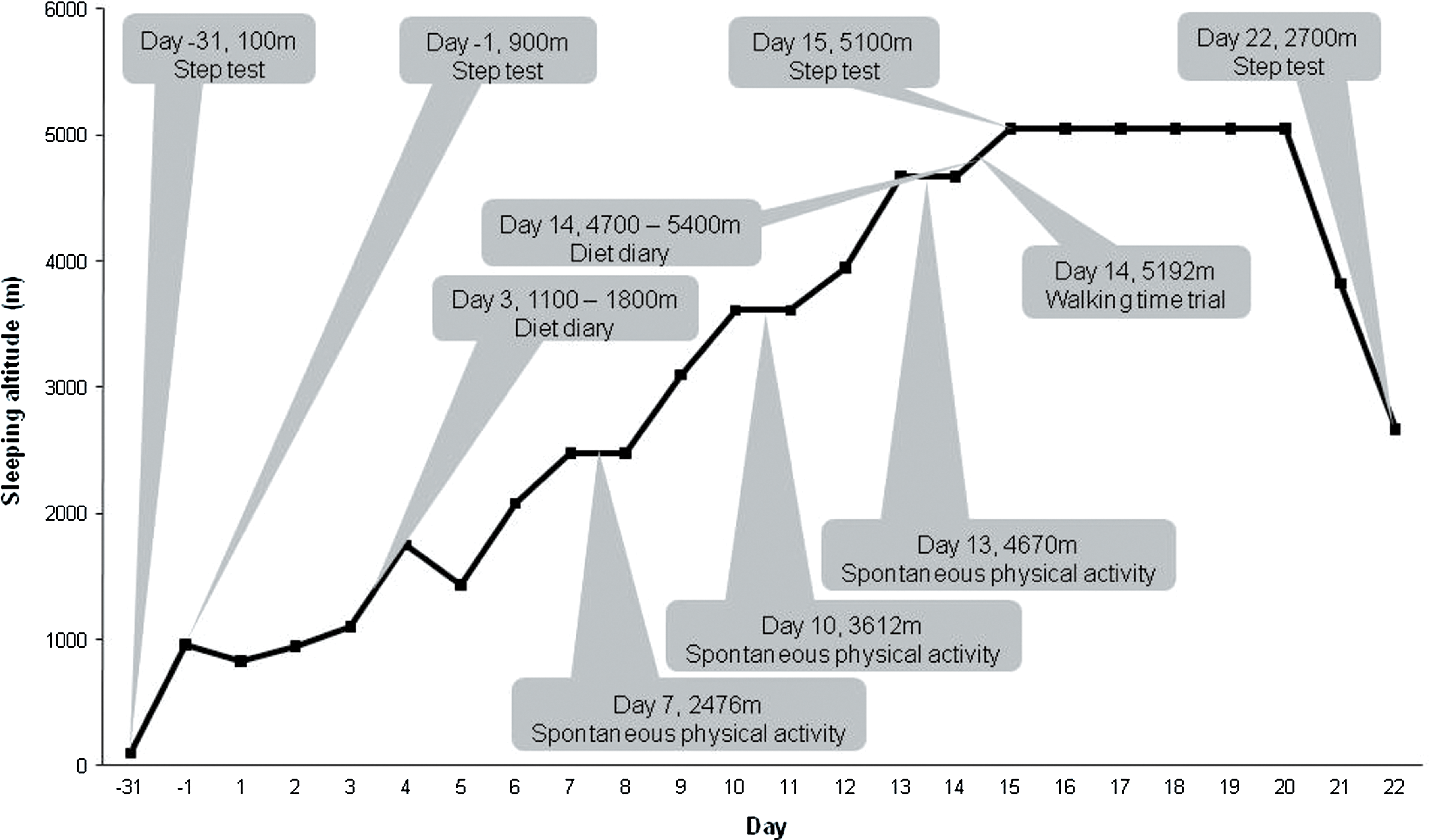
Study design.
The second test of performance was a submaximal incremental exercise step test to obtain rating of perceived exertion and simple cardiovascular parameters. This measure was chosen to represent the mode and intensity of exercise typically performed in mountaineering tasks. The step test was conducted one month prior to (Day -31, 20 m), one day prior to (Day -1, 960 m), mid (Day 15, 5050 m) and post (Day 22, 2670 m) the expedition. In the morning following a 2 h fast, participants were required to complete a step test comprising of a 4 min rest period, followed by two 4 min stages of stepping on a 22 cm high step, at 13 and 26 steps·min−1, respectively. This equated to a mean power output of 44±8 W and 89±16 W, respectively. Participants wore mountaineering base layers and winter boots. Correct stepping frequency was maintained throughout using an electronic metronome. Ratings of perceived exertion and heart rate (both as above) were recorded in the final 30 seconds of each stage.
The final performance measure was spontaneous physical activity level during waking hours recorded on three rest days at the altitudes of 2476 m, 3612 m, and 4670 m. Physical activity was measured using a tri-axial accelerometer (3dNXTM model v2, BioTel Ltd., Bristol, UK). Participants wore the monitor on their lower back, attached by a belt, to record daily physical activity count, and removed the monitor only for washing and downloading of data. The monitor measured acceleration in the anterio-posterior, medio-lateral and vertical directions with a sampling range of 0.2–10 Hz, and a sampling frequency of 100 Hz. Body movement (accelerations or counts, where a count of 1000 equated to an acceleration of 1 g) was recorded in 1-min epochs; total activity counts per minute were calculated as the sum of x, y, and z axis counts, and expressed as total activity counts per day for awake hours (that were defined by a self report sleep diary) (Carter et al., 2008). The validity and reliability of this technique has been demonstrated previously (Carter et al., 2008).
Intake of drinking solution was self-recorded every day by using drink bottles of known volume, and bead counters to record refills, as previously described (Macdonald et al., 2009). Food diaries were recorded for 24 h on 2 days of the expedition (Fig. 1) by each participant under the supervision of a group researcher, as previously described (Macdonald et al., 2009). Dietary composition (including fluid from food) was calculated using computer software (Dietmaster, Lifestyles Technologies Inc, Phoenix, Australia).
Statistical analysis
All data are presented as means±SD. All analyses were performed on a statistical computer package (SPSS Version 15, Illinois). Statistical significance was set at p≤0.05 (2-tailed). An intention to treat analysis detailed overall effect of supplementation; trial participants were analyzed within the group to which they were randomized, regardless of how much treatment they actually received. Missing data were treated by removing the participant from analysis (rather than using a last observation carried forward method). A per protocol analysis detailed effect of carbohydrate supplementation in compliant individuals; participants from the carbohydrate group were only included in the per protocol analysis if all outcome data were available, and if they had consumed sufficient supplement to receive at least 400 kcal·day−1 on top of their normal diet. This value was chosen because it equated to energy deficit observed in previous chamber studies (Rose et al., 1988; Westerterp et al., 2000) and ensured participants exceeded the recommended minimum carbohydrate consumption for high altitude sojourners (Hoyt and Honig, 1996). Participants included in the per protocol analysis thus received>5.7 kcal·kg body mass−1·day−1 of carbohydrate. Providing all outcome data were obtained, all participants from the placebo group regardless of compliance were included in the analysis, because the placebo supplement had negligible nutritional value.
Baseline anthropometric, basic physiological data, and the preloaded mountaineering time trial data were analysed by Student's t test (after checking relevant assumptions). Effect size (Cohen's d) was also presented for main outcome measures and can be interpreted as small (0.2), medium (0.5), or large (0.8).
Data from the submaximal incremental exercise step test were analyzed by a three-factor repeated measures analysis of variance, with within factors of time (days -31, -1, 15, and 22) and workload (rest, stage 1, and stage 2), and a between subjects factor of allocation (carbohydrate or placebo). The spontaneous physical activity data were analyzed by a two-factor repeated measures analysis of variance with a within factor of time (days 7, 10, and 15), and between factor of allocation (carbohydrate or placebo). Assumptions such as normal distribution and sphericity of data were checked by visually inspecting plotted data, and by Mauchley's test and Box's M in SPSS. Greenhouse-Geisser correction to the degrees of freedom was applied when violations to sphericity were present (Stevens, 2002). Significant main effects and interactions were followed up with test of simple main effects, Tukey's test, or step down Holm-Bonferroni procedures (Ludbrook, 1998) as appropriate to control for multiple comparisons.
Sample size was based on data obtained during a pilot study assessing rating of perceived exertion during a preloaded rucksack carry task (Macdonald and Oliver, 2008), and using the method of magnitude-based inferences (Hopkins, 2006). The smallest change worth detecting was assumed to be one unit of the rating of perceived exertion scale. The between subject standard deviation was 0.74. With maximum rates of statistical errors of 0.5% and 25% (type I and type II, respectively), a total sample size of 12 participants (6 per group) was required.
Results
The flow of participants through the study is shown in Figure 2. Participants were recruited during a familiarization weekend in September 2008 and were followed up for the entire 22-day expedition, which was completed in October 2008. For anthropometric and basic physiological variables, no significant differences were noted between carbohydrate and placebo group for both intention to treat and per protocol analyses (Table 1).
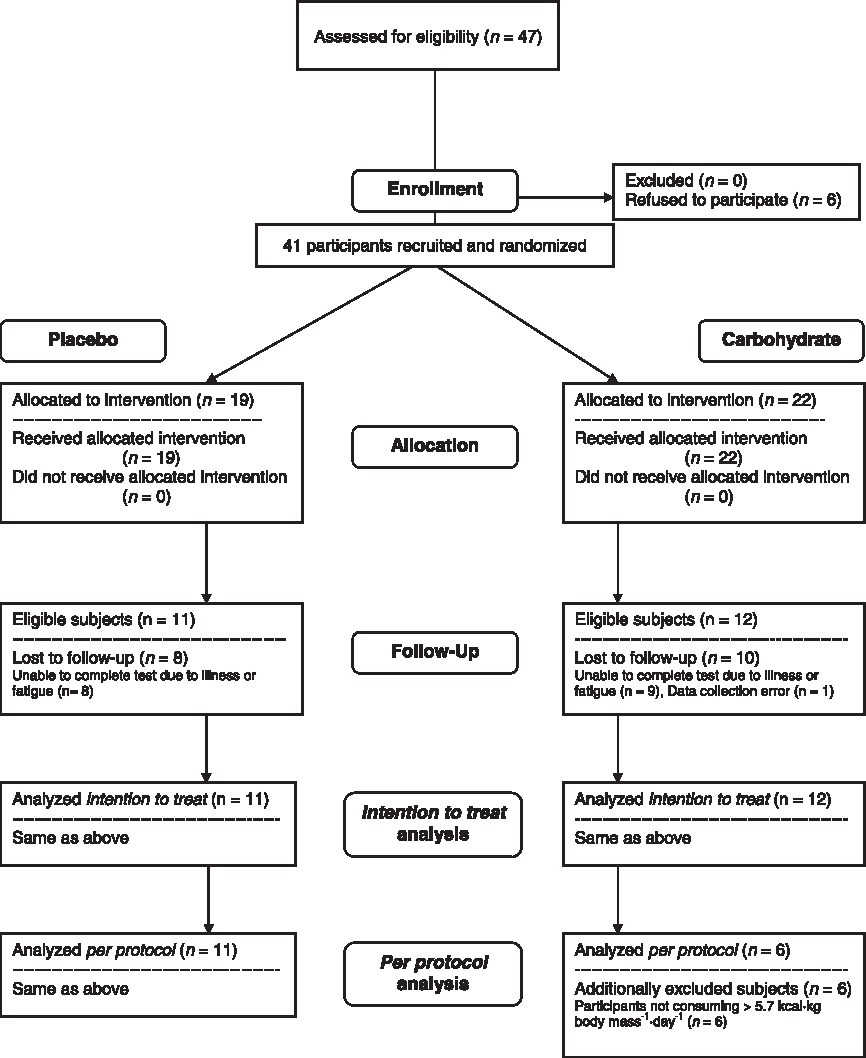
Flow of participants through the study.
Dietary analysis confirmed that, during the expedition, daily carbohydrate intake increased in the supplementation group, as compared to the placebo group, yet the intake of carbohydrate, protein, and fat from solid foods and other drinks remained similar (Macdonald et al., 2009). Specifically, 11 of 22 individuals (50%) originally allocated to receive carbohydrate were sufficiently compliant to achieve the target average supplemented intake of 400 kcal·day−1 (>5.7 kcal·kg body mass−1·day−1 of carbohydrate). Results of dietary analyses completed on the day of the mountaineering time trial in compliant participants completing the time trial are presented in Table 2, and confirm that total carbohydrate intake was increased by 44% compared to placebo.
Data are means±SD obtained from a per protocol analysis. Dietary data are from the entire day of the time trial. HR, heart rate; SpO2, arterial oxygen saturation; Preload stage, walking speed of 3 km·h−1. Statistical significance was determined by independent t tests, *p<0.05 between placebo and carbohydrate groups. Effect sizes can be interpreted as small (0.2), medium (0.5), or large (0.8).
For the mountaineering time trial, intention to treat analyses revealed no significant differences between the two groups for any outcome measure, although in the carbohydrate supplementation group rating of perceived exertion during the preload phase was one scale point less than in controls (11.5±2.8 vs. 12.8±0.9, t=1.56, p=0.142, d=0.60). In contrast, results from the per protocol analyses revealed that rating of perceived exertion during the preload phase (Fig. 3, top panel) and time to complete the time trial (Fig. 3, bottom panel) were significantly reduced by 17% and 18%, respectively, in the carbohydrate compared with the placebo group. Specifically, compliant participants allocated to the carbohydrate supplement group reported significantly reduced ratings of perceived exertion compared to those allocated to the placebo group (10.5 (95% confidence interval: 8.4–12.3) vs. 12.8 (12.3–13.3), t=2.51, p=0.047, d=1.30 (large effect)). Those allocated to carbohydrate also completed the 600 m time trial (preload and maximal effort stage) faster than those allocated to placebo (990 s (903–1077) vs. 1194 s (1041–1347), t=2.28, p=0.038, d=0.86 (large effect)). Despite this improved performance, there were no obvious differences in physiological parameters, such as heart rate or oxygen saturation, at rest or during the preload stage, except for a trend and large effect size for blood glucose to be higher in the carbohydrate group (Table 2).

Rating of perceived exertion in the preload stage (top panel) and total elapsed time including both preload and maximal effort stage (bottom panel), during a mountaineering time trial performed at 5129 m. Data are means±SD obtained from a per protocol analysis. Preload stage, 200 m with no height gain at walking speed of 3 km·h−1; maximal effort stage, 400 m with 128 m of vertical height gain at maximum walking speed. Statistical significance was determined by independent t-test: *p<0.05 between carbohydrate and placebo groups.
For the submaximal incremental exercise step test, intention to treat analyses revealed a significant triple interaction for heart rate (F=3.764, p=0.007, Fig. 4, bottom panel), but not for rating of perceived exertion (F=0.087, p=0.917, Fig. 4, top panel). Thus, at 5050 m, participants allocated to carbohydrate supplementation group had a significantly lower resting heart rate compared with the placebo group. It is worth noting that AMS scores on the day of testing were similar for the two groups (Table 1). As expected, heart rate in all stages of the step test (F=13.283, p<0.001) and ratings of perceived exertion in all stages of the step test except rest (F=37.501, p<0.001) were significantly elevated at Day 15 (5050 m) compared with all other time points (20 m to 2670 m), as evidenced by main effects for time. Per protocol analyses revealed no further significant findings.
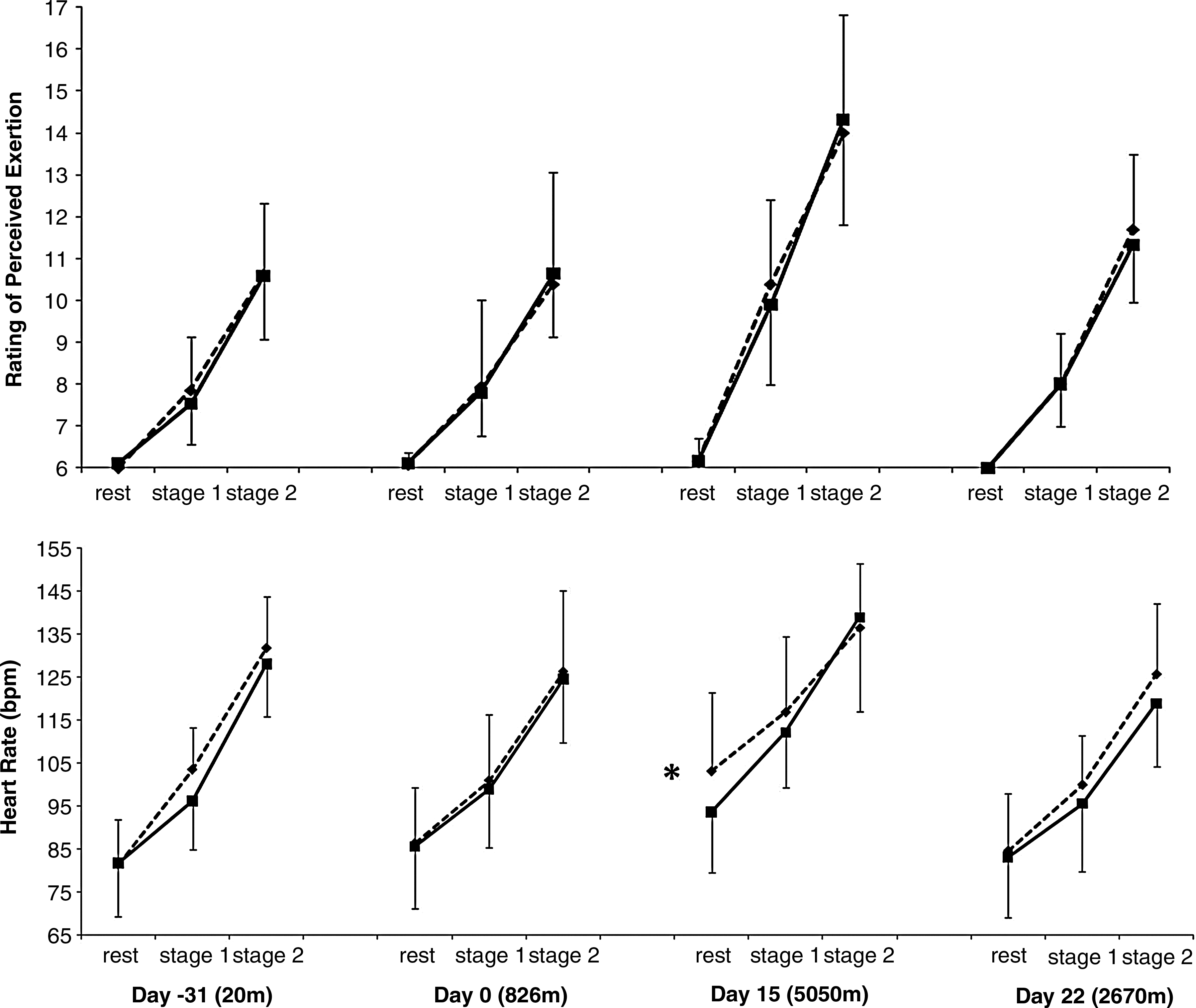
Ratings of perceived exertion (top panel) and heart rate (bottom panel) in response to a submaximal incremental exercise step test completed before, during, and after a high altitude expedition. Solid line: carbohydrate supplementation group; dashed line: placebo group. Statistical significance was determined by three-factor analysis of variance. There was a significant triple interaction for heart rate: *p<0.05 between carbohydrate and placebo groups.
Spontaneous physical activity counts averaged 103,768±46,507 per day; however, carbohydrate supplementation had no effect on the three rest days assessed as indicated by no interaction (F=0.099, p=0.906) and no main effect of group (F=0.93, p=0.768).
Discussion
The main finding of the present study is that a commercially available carbohydrate energy drink is sufficiently palatable and easy to administer to allow chronic supplementation of carbohydrate intake, improving mountaineering exercise performance during a high altitude expedition. In particular, perceived exertion and time to complete a mountaineering time trial were reduced at 5192 m in those consuming a carbohydrate supplement compared with a placebo. In contrast, rest day spontaneous activity and submaximal step test performance, as assessed by perceived exertion and heart rate, were not different between the carbohydrate and placebo supplemented groups throughout the high altitude expedition.
In contrast to solid carbohydrate supplementation, which has previously been shown to be ineffective at increasing carbohydrate intake at altitude (Edwards et al., 1994), the ad libitum provision of carbohydrate as a beverage successfully increased total daily carbohydrate and energy intake. Specifically, 50% of participants allocated to carbohydrate achieved an average daily supplement intake greater than our target of 400 kcal per day. Thus, compliant individuals attained the recommended intake of 400 g of carbohydrate per day from their total diet (Brouns, 1992; Marriott and Carlson, 1996). Notably, participants allocated to the placebo group fell far short of this target, achieving only 262 g of carbohydrate per day from their total diet. It is plausible that beverages are more effective at increasing carbohydrate intake than solid food, because they are easier to prepare and consume throughout the day in the hostile environment experienced at high altitude, and are more palatable if sojourners are nauseous. These results extend a single previous study at altitude where carbohydrate beverages were shown to increase daily energy intake and double carbohydrate intake but only for a period of 4 days (Askew et al., 1987).
Although the effect of carbohydrate supplementation at altitude has not been extensively investigated, some (Askew et al., 1987; Consolazio et al., 1969; Fulco et al., 2005) but not all (Fulco et al., 2007) acute efficacy studies indicate carbohydrate may benefit exercise performance at altitude. The current study extends these previous investigations by also showing a beneficial effect of chronic carbohydrate supplementation, even when acclimatization may have attenuated carbohydrate efficacy (Fulco et al., 2007), when achieved doses are lower (Jeukendrup, 2004) and when metabolic effects may be different (Erlenbusch et al., 2005). The present study also suggests that beneficial effects of carbohydrate seem to be realized during more applicable and relevant mountaineering performance tasks, and that performance on these tasks may be suboptimal when carbohydrate intake is less than 3.7 g·kg body mass−1 per day. Thus, this study also provides the first experimental evidence that not achieving recommended guidelines for carbohydrate intake of 400 g per day is detrimental to performance.
However, although carbohydrate supplementation had a positive effect on the mountaineering time trial, which was completed after 8 km of walking at altitudes above 4600 m and after 500 m of vertical gain, there was no effect of carbohydrate supplementation on the submaximal step-tests or on spontaneous physical activity on rest days. The effects of carbohydrate supplementation might therefore be exercise duration or intensity dependent, where positive effects are observed after prolonged exercise or during periods of higher-intensity exercise only. These findings are consistent with one of the only other investigations examining carbohydrate intake and performance at altitude, where 9 days of liquid carbohydrate diet had no effect on submaximal treadmill exercise physiological responses (i.e., heart rate, ventilation, or oxygen consumption), but did improve time to exhaustion (Consolazio et al., 1969).
During periods of energy deficit at altitude, resting muscle glycogen and serum glucose concentration are reduced (Askew et al., 1987; Young et al., 1982). One mechanism by which the higher daily carbohydrate intake could improve endurance performance at altitude is therefore by better maintenance of important exercise substrates (i.e., muscle and liver glycogen and blood glucose (Bergstrom and Hultman, 1967; Romijn et al., 1993)). Specifically, carbohydrate supplementation has previously been shown to better maintain blood glucose, increase carbohydrate oxidation, and spare liver glycogen, as well as to promote glycogen synthesis during and after exercise (Jeukendrup, 2004). In the present study and in previous research (Askew et al., 1987), blood glucose levels were superior in those supplemented with carbohydrates, supporting a role for improved substrate availability. To date, no study has examined whether muscle or liver glycogen is maintained at a higher level or increases with chronic carbohydrate supplementation at altitude; however, this has been shown many times at sea level (Bergstrom and Hultman, 1967; Simonsen et al., 1991).
It is also plausible that mountaineering time trial performance might have been, at least in part, improved via alterations of perception of effort (Marcora and Staiano, 2010), particularly as perceived exertion was lower during the mountaineering time trial in the present study. Carbohydrate supplementation during prolonged exercise at sea level lowers perceived exertion and central fatigue (Backhouse et al., 2005; Nybo, 2003), while chronic carbohydrate diets have also been previously shown to be associated with lower perceived exertion during exercise at sea level (Achten et al., 2004) and during exercise at altitude (Consolazio et al., 1969). At altitude, carbohydrate supplementation also increases carbon dioxide production (Golja et al., 2007), respiratory quotient (Eckman, 1945), pulmonary ventilation, and ultimately arterial oxygen saturation (Hansen et al., 1972; Lawless et al., 1999), although whether these mechanisms contributed to the improved performance observed in the present study is not clear.
Carbohydrate supplementation may also exert beneficial effects via the central nervous system (CNS) (Jeukendrup, 2004). Consistent with this is the lower resting heart rate observed before the submaximal step test in the carbohydrate group at 5050 m, which was not due to differences in altitude illness. This finding extends recent research at sea level, which indicates that low carbohydrate intakes (<2 g·kg body mass−1 per day) are associated with an increase in resting sympathetic activation and reciprocal vagal withdrawal (Havemann et al., 2006; Lima-Silva et al., 2010). As the difference diminished with exercise, it might be speculated that the effect of carbohydrate acted on the vagal withdrawal component of heart rate control.
Finally, taken together with other findings by our group (Macdonald et al., 2009), the present study suggests that carbohydrate intake may be more important for maintaining altitude performance than preventing weight loss. Although participants allocated to carbohydrate improved performance, we have shown previously that supplementation did not prevent body mass loss (Macdonald et al., 2009). This interpretation is supported by energy restriction studies at sea level and altitude, where deficits of 750–1500 kcal per day did not reduce 5-mile run performance, muscle strength, and endurance performance (Fulco et al., 2002; Zachwieja et al., 2001), and an isocaloric diet study at altitude where treadmill time to exhaustion was significantly longer in those consuming the higher relative carbohydrate diet (Consolazio et al., 1969).
It must be remembered that not all participants allocated to the carbohydrate group were compliant. Expedition leaders will need to educate altitude sojourners that compliance is important to attain performance benefits. For a 70 kg person, a minimum target is 1 L of 10% carbohydrate solution per day. Given that higher daily carbohydrate intakes have been shown to further improve exercise performance at sea level (Achten et al., 2004; Simonsen et al., 1991), future research should examine whether the prescription of higher carbohydrate diets can be tolerated and have further benefits to exercise performance at altitude. Future studies should also determine whether chronic carbohydrate supplementation at altitude increases performance via similar mechanisms to that observed at sea level.
Conclusion
In conclusion, carbohydrate beverages are a well tolerated and effective strategy to palatably and easily increase chronic carbohydrate intake and improve prolonged mountaineering performance at high altitude.
Author Disclosure Statement
This study was supported by Science in Sport (drinks supplement and funding for outcome measures), Ministry of Defence (Army) (funding for outcome measures), Mountain Equipment (researcher personal equipment), Panasonic United Kingdom (Toughbook laptops), Qatar Airways (Carriage), Polar United Kingdom, Optimal Performance, nSpire Health Inc, Vitech Scientific, and Digitalscales.com (all scientific equipment). The study funders played no part in study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the article for publication. This work is the opinion of the authors and not that of Science in Sport or Ministry of Defence (Army). Portions of this article were presented in abstract form at the Medical Expeditions Altitude Symposium 2008, 4 December and at Hypoxia 2009, 11–14 March.
Footnotes
Acknowledgments
The authors gratefully acknowledge all participants, data collectors, and funders.