
Abstract
Abstract
Burtscher, Martin, Erich Gnaiger, Johannes Burtscher, Werner Nachbauer, and Andreas Brugger. Arnold Durig (1872–1961): Life and work. An Austrian Pioneer in exercise and high altitude physiology. High Alt Med Biol. 13:224–231, 2012.—Arnold Durig (1872–1961) grew up in the Austrian mountains in the period when intense exploration of the Alps started. As an enthusiastic mountaineer, scientist, and physician, he became one of the pioneers exploring physiological and pathophysiological aspects of humans sojourning to high altitudes. At the beginning of the 20th century, Durig was one of the great physiologists whose knowledge covered the whole field of physiology. Durig founded a renowned School and his students spread all over the world. He stayed in close contact with many colleagues and famous scientists, such as Albert Einstein and Sigmund Freud. Although he was an extremely productive and acknowledged physiologist and teacher at that time, his work and life are not very well known at the beginning of the 3rd millennium, even by high altitude physiologists. Thus, this article provides an overview on Durig's life and work, highlighting the most important scientific studies he performed at moderate and high altitudes, in an attempt to provide a few links to the development of high altitude research in the late 19th and early 20th centuries, complemented by some comments from a current point of view.
Introduction
Arnold Durig sojourning in his beloved mountains of the Montafon (Vorarlberg, Austria); (Manfred Dönz, Schruns, Vorarlberg).
Biography
Early life
Arnold Durig's father came from Tschagguns, a small mountain village in the Montafon in the Austrian province of Vorarlberg. He was the head of the teacher training college in Innsbruck, where Arnold Durig was born on November 12, 1872. There, Arnold Durig spent his childhood and school days, started studying medicine, and at the early age of 22, he obtained an assistant position in Professor Vintschgau's team. In 1898, he earned his medical degree from the University of Innsbruck.
Start of medical and scientific career
Durig acquired clinical experience at various hospital departments, and after working as a country doctor in Lower Austria for some time, he became an assistant of Professor Sigmund Exner at the Institute of Physiology at the University of Natural Resources and Life Sciences in Vienna in 1900. Two years later, he achieved the position of a private lecturer at this university. After having the opportunity to visit Oxford for one semester of research, he started his important collaboration with Professor Nathan Zuntz from the Royal Agricultural College in Berlin.
Core research on altitude physiology
In 1903, Durig participated in the high altitude studies on respiratory and metabolism physiology performed by Nathan Zuntz and his team at the Capanna Regina Margherita (4560 m) in the Monte Rosa Massif. Afterwards, he returned to Vienna where he became an associate professor specializing in the anatomy and physiology of domestic animals in 1904, and a full professor in the same field 1 year later (Brugger, 2011; Montafon Archive 1 and 2). In 1905, Durig conducted the “Bilkengrat Studies” on metabolism and alcohol effects during hiking in the mountains of the Montafon (Vorarlberg, Austria) (Durig, 1906a,b). Afterwards, he led his own expedition to the Monte Rosa during the summer months in 1906 (Durig, 1911). Four years later, Durig participated in a further expedition with Nathan Zuntz, this time to Tenerife (Canary Islands) where he performed further high altitude studies on Pico Teide (3718 m). Although Durig remained an enthusiastic mountaineer for his whole life, his main research work on high altitude physiology only continued for about 1 decade (Gunga, 2009).
Time during and after the First World War
In 1914, Durig was called up into military service and became the head of the Department of Internal Medicine in the Fortress Hospital in Sarajevo, and later of the Department of Infectious Diseases in the same hospital. One year later, he was appointed as chief staff surgeon and commanding officer of the Military Hospital in Grinzing, Vienna, with 6000 beds. It was the largest hospital in Austria; 116,000 patients were treated under Durig's direction between 1915 and 1918 during the First World War (Oberkofler, 1972)
In 1918, Durig succeeded Exner as head of the Institute of Physiology at the University of Vienna. During the following years, Durig structured his institute by dividing it into departments of physiological-chemistry, comparative physiology, morphologic physiology, sensory physiology, electro-physiology, and special physiological operative sections. Durig also founded departments for applied physiological methodology, physiological examination, and physical therapy in the Vienna General Hospital (Oberkofler, 1972).
Durig and his staff were extremely productive over 2 decades, as shown by their more than 1000 publications (Scheminsky, 1952). Their main research focused on the physiology of nutrition and metabolism, the regulation of blood pressure, and social and occupational medicine. Thus, Durig was highly predestined to be involved in public health affairs. He established a renowned school and his students spread all over the world. Among the most famous are Ulrich Ebbecke (Bonn), Walter R. Hess (Zurich), Franz Lippay (Adelaide), Richard Wagner (Munich), Rudolf Allers (Washington), Walter Fleischmann (Baltimore), and Emil Fröschels and Paul Liebesny (both in New York) (Oberkofler, 1972).
The Second World War and retirement
In 1938, Arnold Durig was forced to retire due to the “Anschluss” and relocated to the Gauer Valley in Tschagguns in the Montafon (Vorarlberg, Austria). He spent his retirement in his beloved mountains of the Montafon but stayed in close contact with colleagues and scientists all over the world, such as Albert Einstein and Sigmund Freud, as is proved by his personal documents that are preserved in the Montafon Archive at the Montafon Folk Museum in Schruns (Montafon Archive 1).
Right until old age, Arnold Durig remained an enthusiastic mountaineer. He was a member of the Austrian branch of the Alpine Club for 70 years. At the age of 65, only 8 weeks after he had broken his leg, he successfully completed a “23-hour-test-walk” on the following route: Latschau, a district of Tschagguns (about 1000 m)—Scesaplana (2965 m)—Mannheim Hut, formerly called Strasbourg Hut (2679 m)—Palatinate Hut (2108 m)—Drei Schwestern (a mountain with three peaks, the so called “Three Sisters”, about 2000 m)—Frastanz (510 m)—Latschau (about 1000 m) (Montafon Archive 2).
In 1959, Durig's wife Alexandra died. She had been a true companion to him for 60 years, and had given birth to their daughter Ilse in 1905. Two years later, Arnold Durig died on October 18, 1961, at the age of almost 89, in the same year when Erwin Schrödinger, living then in the mountain village Alpbach, the Tyrol, died. Arnold Durig will never be forgotten in the Montafon; in the villages of Schruns and Tschagguns, 2 streets are named after him, and the school of Latschau is called “Arnold Durig School.” Furthermore, in 1978, the Durig–Böhler Prize for innovative medical research in Vorarlberg was created (Brugger 2011; Galehr and Vonier 2008).
Durig's Research on Moderate and High Altitude Physiology
Early high altitude research as inspiration
Arthur Mermod and William Marcet were among the first researchers investigating physiological responses to increasing altitude in humans. Whereas Mermod studied effects at rather low altitudes, starting from Strasburg (124 m) up to Sainte-Croix (1100 m), Marcet already ascended to high altitudes (Breithorn, 4200 m, Switzerland; Marcet, 1878). Marcet also went to Tenerife (Canary Islands) to investigate differences between effects of altitude and temperature using his self-built treadmill for standardized exercise testing up to 3260 m (Alta Vista). Around the same time, Paul Bert studied altitude effects in animals, exposing them to reduced air pressure in a hypobaric room. In 1878, he published his results in the book “La pression barometrique” (Bert, 1878). Several years later, before realizing a famous railway project (planned in 1893 by the Swiss industrialist Adolf Guyer-Zeller) to high altitudes (Jungfrau Joch, Switzerland, 3471 m), the physiologists Hugo Kronecker, Hermann Sahli, and Leon Asher were studied physiological and pathophysiological effects on humans when passively ascending to the Monte Rosa plateau (Kronecker, 1903). Due to the difficulties in transporting subjects, they only reached an altitude of 3750 m. Subsequently, these researchers continued several experiments at the Gornergrat railway (3089 m). At the same time, the Capanna Regina Margherita had been built on the Gnifetti Peak (Monte Rosa Massif, 4560 m), offering a high altitude research station for physiological, zoological, botanical, bacteriological, and physical departments. The main founder of this research station, Angelo Mosso, started with his reknowned high altitude experiments by climbing up to this peak (Mosso, 1898). He studied responses of heart rate, blood pressure, body temperature, and respiration during rest and exercise at various altitudes (Gressoney 1627 m, Inderalp 2515 m, Linty Hut 3047 m, Gnifetti Hut 3820 m, and on the Cap. Margherita 4560 m). In 1895, Zuntz, Schumburg, and Loewy conducted their first expedition to the high altitudes of the Monte Rosa. Angelo Mosso was nearly 60 years of age when Zuntz, Durig and colleagues continued with their physiological studies at Capanna Regina Margherita.
Monte Rosa Study in 1903 with Nathan Zuntz
Nathan Zuntz led his first Monte Rosa expedition in 1895 and a second 6-week expedition in 1901. The main research questions covered the physiological effects of high altitude on respiration and metabolism during rest and exercise (Gunga, 2009).
After this major expedition to the Monte Rosa in 1901, Nathan Zuntz returned for 3 weeks to the Monte Rosa in 1903 to continue and finalize his respiratory and metabolic research at high altitude. Arnold Durig had the opportunity to participate in this expedition to ‘rarefied air.’ A transportable dry gas meter was an essential prerequisite to perform the respiratory and metabolic measurements. This apparatus had been developed by Nathan Zuntz for field studies because the Zuntz–Geppert respiration apparatus was only suitable to perform metabolic measurements in the laboratory. The data collected during this 3-week sojourn to the Monte Rosa are discussed in “Höhenklima und Bergwanderungen in ihrer Wirkung auf den Menschen” (Effects of High Altitude Climate and Mountain Hiking on Humans) published in 1906 by Zuntz and colleagues. A nice overview on the life and entire work of Nathan Zuntz and his collaboration with Durig is provided by Gunga (2009).
“Mountaineering on Monte Rosa” became the title of a chapter in the classic physiology textbook by Graham Lusk at Cornell University, New York City. ‘The Elements of the Science of Nutrition’ (Lusk 1928) illustrates how well received the work of Durig and Zuntz was at that time: “A research of Zuntz on the subject of mountaineering describes how he and Durig ascended to the Col d'Olen (2900 meters), and, having remained there for a week, passed upward to a hut (4560 meters) constructed near the summit of Monte Rosa… They lived in this hut for two and a half weeks. The height of the barometer was 443 mmHg, equivalent to Fi
Durig's most important studies at moderate and high altitude
At the beginning of the 20th century, most of the existing scientific knowledge on high altitude physiology and pathophysiology originating from studies in the Alps had been published in two well-known books authored by Angelo Mosso and Zuntz and colleagues (Mosso, 1898; Zuntz, 1906). Based on that knowledge and on his research collaboration with Zuntz, Durig started his own experiments at moderate and high altitude.
The Bilkengrat Study at moderate altitude
The development of the transportable dry gas meter enabled physiologists to determine the energy requirements for walking on horizontal and ascending paths under various field conditions. At that time, Zuntz and colleagues, and also Zuntz and Durig, had already performed several metabolic studies during walking at low and high altitude (Gunga, 2009; Zuntz, 1906). They consistently demonstrated an energy consumption of 0.55 kcal per 1000 mkg when walking on horizontal paths. Whereas this value had been found to remain stable when carrying additional weight, it tended to increase at high altitude (Durig, 1911). In 1905, Durig extended these experiments when he performed his well-known hiking studies in the mountains of the Montafon (Vorarlberg, Austria). There he determined oxygen consumption and hiking economy during a series of ascents from 1324 m to 2446 m. The main goal of this study was to investigate the effects of alcohol consumption on hiking performance and hiking economy (Durig, 1906a,b). Durig measured an energy consumption of 7.43 kcal per 1000 mkg of vertical distance, corresponding to a hiking economy (vertical distance) of 31.5%. These results were well in accordance with previous findings and they are also comparable to those determined using modern equipment in laboratory settings (ASCM, 1995). The main finding of the Bilkengrat Study, however, was that 30 g of alcohol intake reduced usual hiking speed by 20% and hiking economy by 13% (Durig, 1911). Both effects were attributed to more awkward movements. In addition, Durig was able to show that a small amount of the ingested alcohol was actually used for energy supply to working muscles, however without any beneficial effects when considering the excess energy consumption. He did not see a clear influence of moderate altitude on energy consumption during comparable submaximal workloads.
The Monte Rosa Study
Durig began the intense and sophisticated preparations for his research project on the Monte Rosa in autumn 1905. Beside himself (33 years), four young (23–30 years) healthy and well-trained male researchers and experienced mountaineers participated in the study. Particular attention was paid to the standardization of conditions with a special emphasis on nutrition. The study started in Vienna (250 m) on July 11, 1906. The researchers arrived on the Monte Rosa (4560 m) on August 9 and remained there until September 3, performing a wealth of field experiments. Then they descended to Alagna (1190 m) where they finished their experiments on September 10. They returned to Vienna and conducted several re-tests in January 1907. The main research focus was placed on the effects of high altitude on respiratory gas exchange at rest and during various types of exercise, related cardiovascular and respiratory responses, but also on psychological processes and conditions related to the development of acute mountain sickness (Durig, 1911).
Cardiovascular responses and body temperature
Durig and colleagues performed many properly planned measurements at rest, during, and after exercise under standardized conditions over the entire 1-month period at high altitude. At that time, their primary study goal was to describe physiological responses, mostly without possibilities of studying the underlying mechanisms. They demonstrated that resting heart rates remained nearly unchanged at 2850 m compared to low altitude, but steeply increased with acute exposure to 4560 m and tended to decrease during the 1-month stay at high altitude (Fig. 2). In contrast, resting systemic blood pressure decreased when acutely exposed to 4560 m, but became normal or even increased during the sojourn. Decades later, hypoxia-related sympathetic activation, vagal withdrawal, and regional vasodilation explained the mechanisms for the cardiovascular responses reported by Durig during the first days at high altitude. Because he did not measure stroke volume, cardiac output, and systemic vascular resistance, he had no idea of the reduction with regard to stroke volume and cardiac output and to the increases in vascular resistance and mean arterial blood pressure during prolonged sojourns at similar altitudes (Wolfel and Levine, 2001). Durig found heart rates at submaximal exercise to be already elevated at 2850 m, which was even more pronounced during the first days at 4560 m, but tended to decrease during the sojourn. Again, as he did not measure stroke volume and cardiac output, he did not detect the “cardiac sparing effect” (ie, reduced heart rate, stroke volume, and cardiac output), with sustained exposure to high altitude (Wolfel and Levine, 2001).
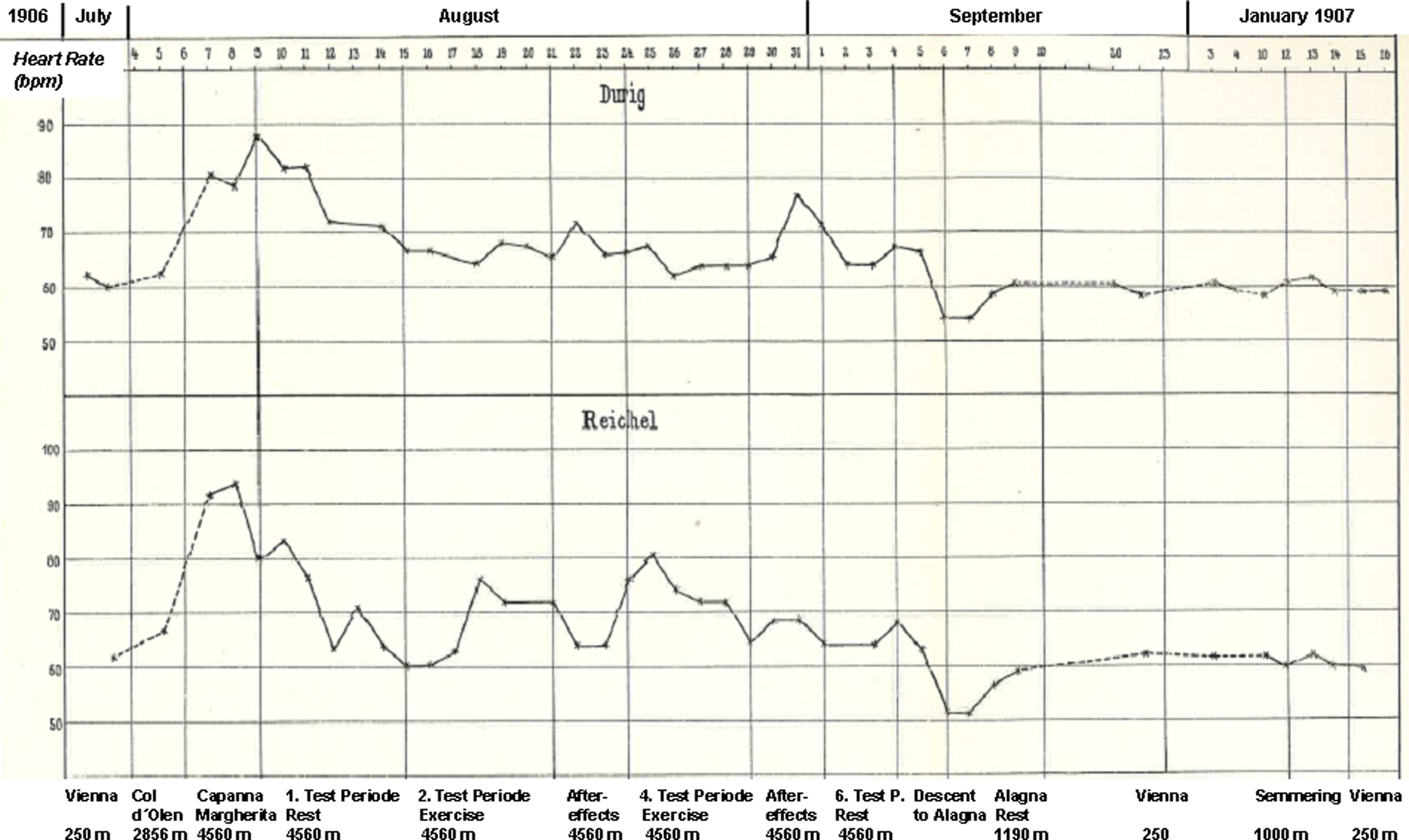
Resting heart rates during the course of high altitude exposure (Monte Rosa, 4560 m) in two study participants (modified according to Durig, 1911).
A similar time course as observed for heart rate was found for body temperature, measured under strictly resting conditions (Durig, 1911). With regard to acute mountain sickness (AMS), Durig highlighted that in a subject suffering from AMS resting heart rates and the increase of heart rate during exercise were highest, whereas the initial increase in body temperature was lowest (Fig. 3). Similar observations have recently been explained by exaggerated sympathetic activation in AMS sufferers accompanied by more pronounced regional vasodilation and resulting heat loss (Loeppky, 2003).
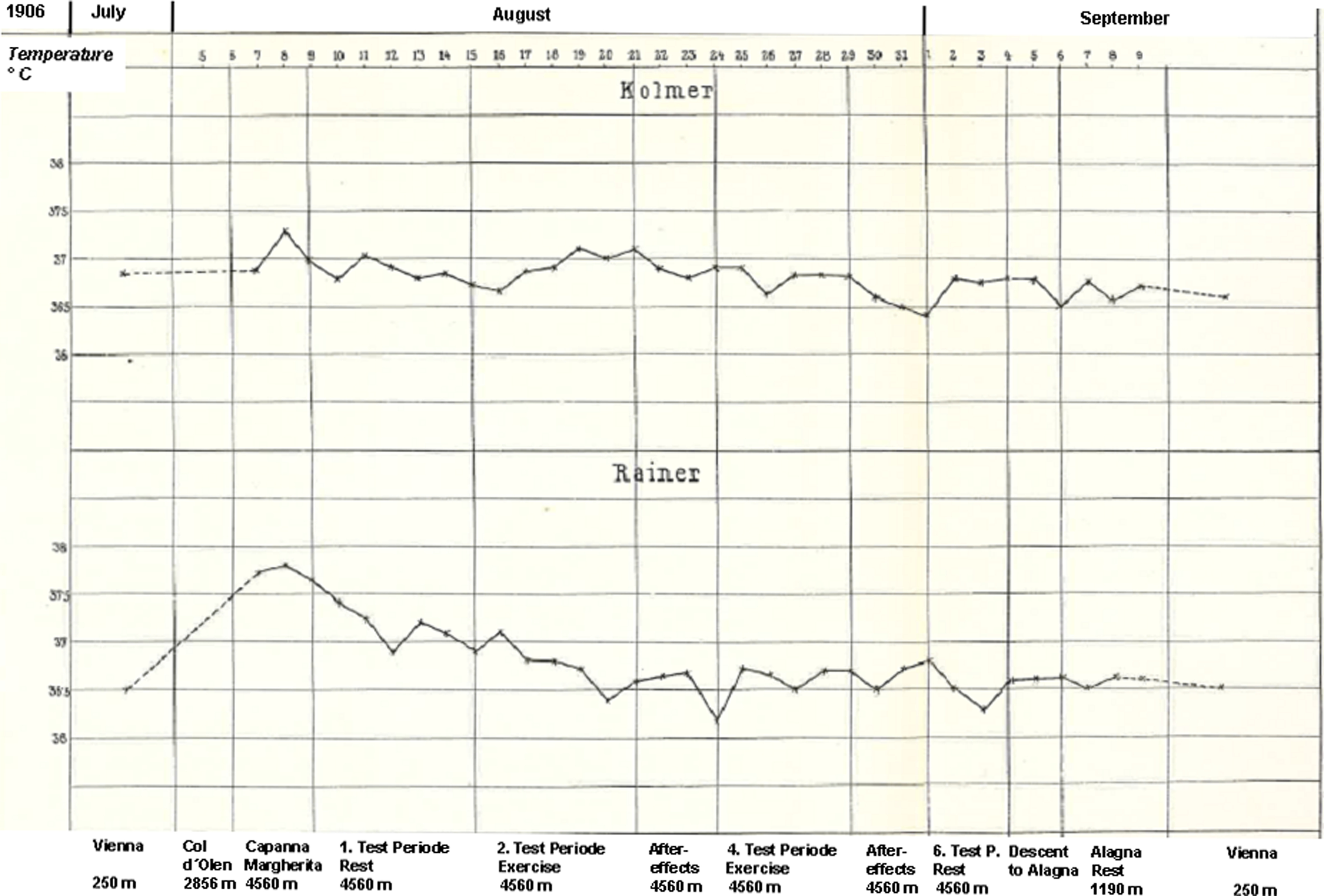
Different courses in body temperature during the high altitude exposure (Monte Rosa, 4560 m) in a participant suffering from AMS (Kolmer) and in a participant who remained healthy (modified according to Durig, 1911).
Respiratory responses
Durig and colleagues confirmed the observations on reduced vital capacity during short-term exposure to high altitudes as reported by Mosso, Zuntz, and others (Durig, 1911). In addition, they did not observe any improvement during the one-month stay at 4560 m. Furthermore, ambient temperature did not affect vital capacity, and no association between vital capacity, endurance performance, and AMS were found. Fatigue of respiratory muscles and hypoxia-related changes in respiratory control were assumed to be underlying mechanisms for the reduction in vital capacity. Many subsequent studies performed during the following decades confirmed these early observations. In addition, increases in thoracic blood volume and interstitial fluid were suggested as important mechanisms contributing to the reduction of vital capacity at high altitude (Rahn and Hammond, 1952).
With regard to resting minute ventilation determined under BTPS conditions, Durig did not see essential changes at 2850 m compared to low altitudes, although minute ventilation was increased at 4560 m in all subjects. This increase seemed to be due to an elevated tidal volume rather than to respiratory frequency. Subjects who demonstrated increased respiratory frequency during acute exposure to high altitude showed a decline during the 1-month stay on the Monte Rosa. In comparison to low altitude, increases in exercising minute ventilation occurred already at 2850 m and were more pronounced at 4560 m. When minute ventilation was calculated for STPD conditions, resting values were lower and values during exercise were essentially the same at high altitude. Durig also recognized that increasing paCO2 values must primarily cause hyperventilation at low altitude and that the reduced paO2 may increasingly contribute to hyperventilation at high altitude (Durig, 1911). The sustaining hyperventilation at rest and during exercise throughout the 1-month stay at high altitude was not influenced by symptoms of AMS or prior exercise. Durig's observations on ventilatory responses at rest and during exercise at high altitude were confirmed, although exact mechanisms of control of breathing at high altitude remained unclear at that time. Decades later, the increased neural output from peripheral chemoreceptors, mainly the carotid bodies, were established as the most important stimulatory mechanism in acute hypoxia (Hornbein and Severinghaus, 1969).
Alveolar O2 and CO2 partial pressures
Durig continued to measure alveolar gases during various conditions at low and high altitude using the transportable dry gas meter developed by Zuntz and colleagues. He found decreasing paO2 and paCO2 values at altitudes as low as 1000 m. On the Monte Rosa (4560 m), paO2 decreased to 50–60 mmHg and paCO2 to about 20 mmHg (Durig, 1911). He also demonstrated that paCO2 values decreased after exercise, whereas paO2 values remained unchanged. He did not see an association between alveolar gas concentrations and symptoms of AMS. At that time Durig was not able to investigate changes in lung diffusion capacity during acute and prolonged exposure to high altitude. About 7 decades later, the multiple inert gas elimination method was developed that allowed a VA/Q mismatch to be distinguished from diffusion limitation (Evans and Wagner, 1977).
Energy expenditure during walking on horizontal and inclining tracks
Due to his prior work with Zuntz and colleagues and his studies at moderate altitude (Bilkengrat Study), Durig was experienced in measuring energy expenditure during exercise. He also was well aware of the fact that submaximal exercise, such as walking, is purely aerobic. Therefore, the transportable dry gas meter enabled Durig to determine oxygen consumption and thus energy expenditure during various activities at low and high altitudes.
Durig compared the many available results of walking trials in the laboratory and the field (e.g., trials by Zuntz and colleagues, A. Katzenstein, and J. Loewy, Frentzel, Reach, Bürgi, Schumburg), investigating the energy expenditure during horizontal and ascending walking (Durig, 1911). He carefully studied applied methods and discussed their potential limitations. He tried to optimize methods and focused mainly on field studies in order to determine energy expenditure under real life conditions. It was to Durig's advantage that towards the end of the 19th century essential measurement methods were developed for quantifying human movement. Beside dry gas meters (Zuntz, 1906), cinematographical methods (e.g., Braune and Fischer, 1891; Muybridge, 1887) and kinetic methods (Marey, 1889) were developed and in particular applied to human gait. Durig was among the first scientists who measured oxygen consumption during walking at high altitude and calculated energy expenditure and movement efficiency. Up to now, energy consumption of walking has been broadly investigated (e.g., Margarina, 1936; Minetti et al., 2002). In contrast to Durig's approach, these measurements were predominately conducted in laboratory setups using treadmills and sophisticated technical collection equipment. Astonishingly, the results provided by Durig are in line with these measurements. Moreover, the basic considerations on metabolic energy consumption and external work are still the same as in Durig's work.
Durig performed walking trials on horizontal and ascending tracks, during summer and winter seasons, at low and high altitude, at different walking velocities, and after alcohol consumption. He found an average of 0.55 kcal per 1000 mkg on the horizontal track and of 7.5 cal for 1 mkg on the ascending track at a moderate walking velocity. At an optimal walking velocity, the calculated walking efficiency amounted to 30–31%. Based on many measurements, Durig suggested that energy expenditure would exponentially increase above the individual optimal walking velocity. He found the following relationship between energy expenditure and walking velocity:
Based on this relationship he showed that energy expenditure increased by 1.2%–1.5% per m/min increase in walking velocity. He found a tendency of increased oxygen consumption at high altitude under comparable track conditions, incline, and walking velocity. However, he noted large inter-individual variations. Nowadays, these variations can be attributed to inter-individual differences in mitochondrial performance, strongly correlating with mitochondrial oxygen affinity but quite surprisingly not related to mitochondrial density or proton leak (Larsen et al., 2011). Furthermore, Durig showed that oxygen consumption can be maintained during submaximal exercise up to 4560 m. This is generally accepted 100 years later. More recent studies demonstrated, for example, that the reduced oxygen delivery at high altitude is compensated by increased oxygen extraction in the working muscles, without conspicuous changes in mitochondrial respiratory performance measured after 9–11 days in the Capanna Regina Margherita hut (Jacobs, Boushel, Wright-Paradis, Calbet, Robach, Gnaiger and Lundby, submitted). Nevertheless, influences of various environmental conditions on energy expenditure are still matter of debate. A still remarkable observation of Durig's studies on alcohol effects during exercise was the markedly reduced walking efficiency and thus increased oxygen consumption for the same work after alcohol consumption (Durig, 1906b). These effects should also be recognized nowadays by the millions of hikers and skiers visiting mountains around the world every year.
Neuropsychological testing
To analyze effects of high altitude exposition on neuropsychological parameters, time measurements (reaction times) were executed. By this means, the speed of nervous conduction was determined. A device called neuramoebimeter was used to exactly determine either mere reaction times (cue to reaction) or differential reaction times (different cues to specific reaction). Durig's co-worker Reichel concluded on the basis of general observations and the results of these measurements that no major measurable impact of high altitude climate (4560 m) on reaction time and psychic behavior can be assumed (Durig, 1911). But he was not entirely able to exclude minor disrupting effects of high altitude exposure on the human psyche. However, it was not possible to measure such effects due to their small magnitude and due to unavoidable variations in test conditions. Many observations during the following decades have complemented these findings also considering effects of extreme altitudes (Hornbein, 2001).
Study on Pico Teide (Tenerife) in 1910
To obtain a better understanding of the effects of temperature and radiation on physiological responses at high altitude, Durig participated, together with Zuntz and others, in an expedition led by Pannwitz to Tenerife (Canary Islands) in the spring of 1910. Already when crossing from Hamburg to St. Cruz on Tenerife, Durig and Zuntz performed several studies on effects resulting from the sea climate (Gunga, 2009). They did not see any differences between the known effects at low altitude in Berlin and Vienna. In the Tenerife expedition, the participants went to the observatory on the Cañadas del Teide (2100 m) and after 1 week they ascended to the Alta Vista (3260 m), even exploring the summit region of Pico del Teide (3718 m). Beside the observation of heart rate, blood pressure, and body temperature, they especially studied the influences of radiation on respiratory mechanisms and gas exchange to compare the results with the data gathered on the Monte Rosa. The prolonged exposure of the whole body to sun radiation elicited relatively severe health problems of the participants. Durig reported symptoms of severe sun burning and sunstroke (Gunga, 2009).
Although significant changes on respiratory mechanisms and gas exchange were observed, this was due to large inter-individual variations rather than to generally applicable physiological changes. They found a reduced alveolar CO2 tension and increased heart rate during radiation at high altitude. The CO2 tension was similar as observed about 1000 m higher on the Monte Rosa. This was obviously due to sunburn-related hyperventilation rather than to the altitude. From these findings it was concluded that several environmental conditions, such as altitude, temperature, radiation, and wind, impinge on individual cardiorespiratory and metabolic responses. This simple but important conclusion has still to be considered by healthy and even more by diseased subjects visiting high altitudes.
Some Remarks from a Recent Point of View
As discussed, at the end of the 19th century, the pioneers of high altitude research, including Arnold Durig, mainly focused on adjustments of the human respiratory and circulatory systems to high altitude (hypoxia). With the onset of mass tourism to high altitude regions all over the world after 1945, altitude-related medical problems increased and high altitude research was “rediscovered” (Scherrer et al., 2010). On the one hand, high altitude became a natural laboratory for cardiovascular and respiratory physiology and pathophysiology (Scherrer et al., 2010) and on the other hand, researchers extended their activities to extreme altitudes (West, 1982; West 1984). For example, Pugh accompanied the successful 1953 British Everest Expedition as a physiologist and he was the research leader of the 1960–1961 Himalayan Scientific and Mountaineering Expedition (the Silver Hut) completing an ambitious program of studies close to 6000 m (Ward and Milledge, 2002). In 1984, John West reported data collected up to the summit of Mount Everest (8848 m). He demonstrated that extreme hypoxia can only be tolerated by an enormous increase in ventilation, which results in an alveolar partial pressure of CO2 of 7.5 mmHg on the summit of Mount Everest accompanied by an arterial pH of over 7.7, the arterial partial pressure of oxygen was less than 30 mmHg, and maximum oxygen uptake was about 1 L/min. Nearly all aspects of exposures to the extreme altitudes (simulated and real) of Mount Everest were covered by additional research activities during the following 3 decades: Operation Everest II, Operation Everest III: COMEX '97, and Caudwell xtreme Everest expedition (Grocott et al., 2010; Houston et al., 1987; Richalet, 2010).
Arnold Durig's perspective of ‘healthy aging’ reads like a modern account of life style and quality of life, with a connection to traditional alpine farming which belongs to history today, and written in the spirit of an enthusiastic mountaineer: “This rapid loss in physical power is typical of the industrial worker, while the farmer retains his strength undiminished far into old age. A true proof of the social value of a system is the length of life before invalidism. The longer this period extends, the better one finds the working and living conditions to have been. Of course, there are many other factors which are not in the realm of physiological research but which are responsible for the premature exhaustion of the industrial worker. These include unhygienic shops, industrial disease, unhealthy homes, bad habits of life, the desolating effects of alcoholism, and other excesses. Also psychical influences, the monotony of much machine labor, the noise of the machines, worry for the future, the compulsion to work, and many other mental influences can act upon the duration of the period of joy in work and thereby also reduce the power to work. We know that work accomplished against personal wish requires a greater expenditure of energy than that accomplished out of love and desire” (Durig, 1916; translated in Lusk, 1928).
Note: The authors'interest in Durig's work is based on some similarities with regard to their career. All the contributing authors have roots in Vorarlberg, all received their academic degree from the University of Innsbruck, and they share a fascination for the mountainous environment.
Author Disclosure Statement
The authors disclosed no financial ties or conflicts of interest.
Contribution to K-Regio project MitoCom Tyrol funded by the Tyrolian Government and the European Regional Development Fund.