
Abstract
Abstract
Lawley, Justin Stevan, Samuel James Oliver, Paul Mullins, Daniel Morris, Naushad Ali Junglee, Charlotte Jelleyman, and Jamie Hugo Macdonald. Optic nerve sheath diameter is not related to high altitude headache: a randomized controlled trial. High Alt Med Biol. 13:193–199, 2012.—The mechanism of high altitude headache (HAH) remains unknown. The aim of this study was to determine experimentally whether optic nerve sheath diameter (ONSD), as an indicator of intracranial pressure, is related to HAH. Following sea level measurements at 3 and 12 hours (SL), 23 subjects were passively transported to high altitude (3777 m, HA) via cable car. HAH, ONSD, arterial oxygen saturation (Sp
Introduction
Headache (and other symptoms associated with altitude exposure) may be a direct or indirect result of hypoxia-induced intracranial hypertension (Houston and Dickinson, 1975; Singh et al., 1969). However, despite the longevity of this hypothesis and evidence linking elevated intracranial pressure with severe altitude illness such as cerebral edema (Singh et al., 1969), evidence of a similar mechanism in mild to moderate HAH or AMS remains limited. Initial investigations utilizing tympanic membrane displacement, telemetric monitoring, and lumbar catheter have reported no changes or only minor increases in intracranial pressure at rest during hypobaric hypoxia, and no association between intracranial pressure and HAH (Bailey et al., 2006;Hartig and Hackett, 1992; Wilson and Milledge, 2008; Wright et al., 1995). Unfortunately, the majority of these techniques are invasive (i.e., lumbar catheter) and as such have limited research within this area, especially within a hypobaric field environment. Thus, recent research identifying optic nerve ultrasonography as a noninvasive surrogate of intracranial pressure (Blaivas et al., 2003; Geeraerts et al., 2007), has led to a small number of studies utilizing optic nerve sheath ultrasonography in the investigation of AMS and/or HAH (Fagenholz et al., 2009; Sutherland et al., 2008).
The sheath surrounding the optic nerve is continuous with cerebral dura and subarachnoid mater. Therefore, elevated intracranial pressure is transmitted downstream within the subarachnoid mater, superficial to the optic nerve, leading to optic nerve sheath enlargement, which is quantifiable by ultrasonography. Sutherland et al. (2008) and Fagenholz et al. (2009) have recently taken advantage of this technique and reported associations between optic nerve sheath diameter (ONSD), altitude, and HAH or AMS. However, to our knowledge, no experimental study has been designed to alleviate illness at altitude and examine the relationship between ONSD and HAH over the time course of symptomatology (i.e., before, during, and after the relief of symptoms). Furthermore, previous field-based investigations have failed to control for confounding variables such as hydration status, height gain, sleeping altitude, rate of ascent, exercise intensity, or other altitude-related illnesses with potentially different etiologies [such as migraine susceptibility (Schoonman et al., 2006) or high altitude cerebral edema (Bartsch et al., 2004)].
Therefore, the aim of this study was to examine serial indirect measurements of intracranial pressure as estimated by optic nerve sheath diameter over the time course of HAH development and amelioration via acetazolamide (a recognized treatment of altitude illness (Grissom et al., 1992) and via acclimatization. We tested the hypothesis that ONSD would increase on exposure to high altitude in individuals who develop HAH, as compared to individuals who are nonsymptomatic. Furthermore, we hypothesized that ONSD would be reduced in those allocated to acetazolamide compared to placebo and would decrease with acclimatization in parallel to the resolution of HAH.
Materials and Methods
Participants
Twenty-three participants (17 males and 6 females; age=21±2 yrs; body mass=69±11 kg; height=175±9 cm) were recruited to take part in this study and gave written informed consent. Importantly, no participant reported suffering from migraine nor had been above 1500 m in the previous 6 months. Apart from contraceptives, no participants were prescribed any medications and did not take any medications or analgesics during the study. This study was approved by the Bangor University Ethics Committee, conformed to the Declaration of Helsinki (2008) and was registered as a clinical trial (registration number NCT01288781, www.clinicaltrials.gov).
Procedures
All participants were examined over a 12-hour period at sea level (SL, 0 m, Bangor, North Wales) and then during 36 h at high altitude (HA, 3777 m, Aiguille du Midi, Chamonix, France; see Fig. 1 for schematic representation of study protocol). Sea level and altitude exposures were separated by 2 weeks, and participants were transported to HA by cable car. Prior to and during sea level and high altitude exposures, participants were required to abstain from personal exercise or alcohol for a period of 24 h and to follow standardized fluid and nutritional intake. Fluid consumption was prescribed relative to body mass (40 ml·kg−1), divided into five equal amounts and consumed every 3 h while participants were awake. Nutritional intake was prescribed relative to gender and body mass, based on basal metabolic rate plus 8 h of occupational activities (75% standing or sitting, and 25% standing or moving) (World Health Organisation, 2004). Caffeine intake was prescribed based on individual daily consumption to avoid the possibility of caffeine withdrawal headache (Shapiro, 2008) confounding the diagnosis of HAH. In addition, a standardized walking protocol was completed twice daily during both exposures following a course of 1 km at a set pace of 4 km/h.
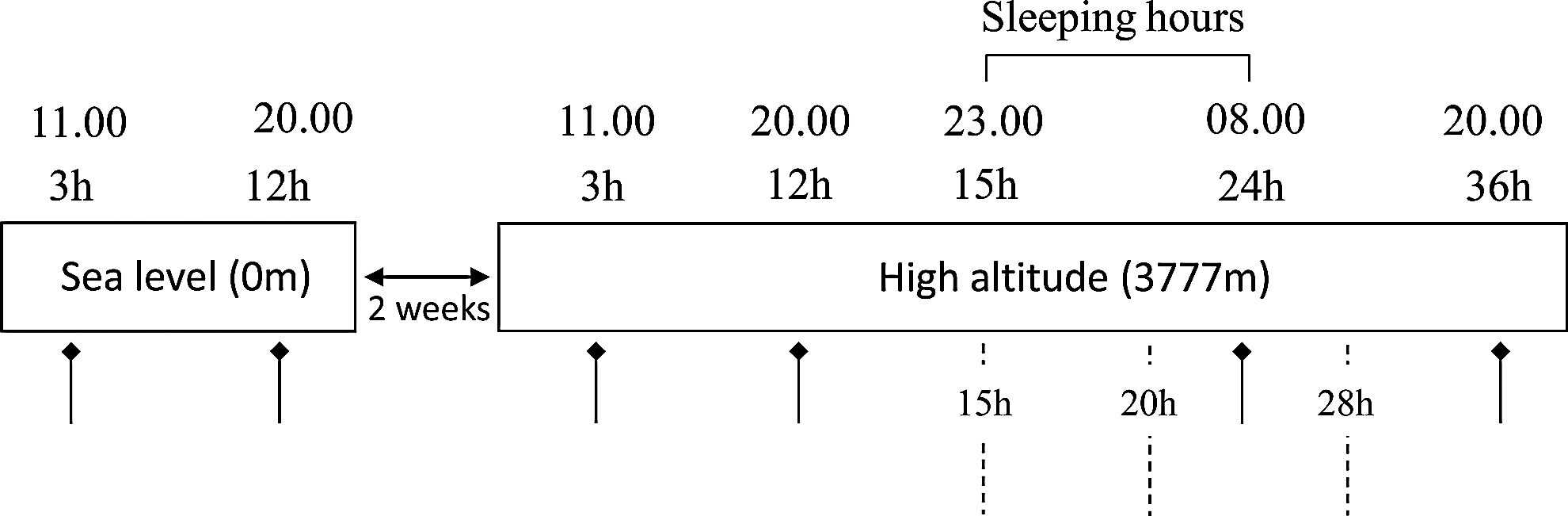
Diagrammatic representation of study protocol. —–▪, measurement of optic nerve sheath diameter, oxygen saturation, heart rate, and fluid balance; —–, administration of acetazolamide (250 mg) or placebo.
After 12 h of high altitude exposure, participants were classified into two HAH groups, based on self-reported headache intensity. Participants were asked to rate their headache intensity by adding a mark on to a 0–100 mm visual analogue scale (VAS). The VAS has been used previously to examine HAH and AMS (Harris et al., 2003; Wagner et al., 2007) and was utilized rather than other categorical verbal rating scales (such as the Lake Louise Questionnaire) due to increased sensitivity and benefits of continuous data (Price et al., 1983). Furthermore, investigation of HAH rather than summation of nonspecific symptoms, as in the diagnosis of AMS, is beneficial due to an increase in signal-to-noise ratio when examining pathological mechanisms (Max and Lynn, 2011; Roach et al., 2011). Headache severity was determined by measuring the distance from 0 on the 100 mm scale (Harris et al., 2003). Participants were consequently classified as HAH positive (HAH+; VAS≥1, n=12, mean VAS=19±14), range=4–38 mm) or HAH negative (HAH-, VAS<1, n=11, mean VAS=0±0), range=0).
After 15 h of high altitude exposure, HAH was experimentally manipulated in a double-blind placebo controlled trial using a recognized treatment for altitude sickness (Grissom et al., 1992). All participants were randomized to receive either acetazolamide (250 mg) or placebo (lactose monohydrate in identical opaque gelatine capsules; Boots Contract Manufacturing, Nottingham, UK) dosed at 15, 20, and 28 hours. The HAH- group served as an appropriate control arm. Randomization was completed by SJO using a permuted blocks design generated by www.randomization.com. Participants were stratified for gender and HAH presence (Fig. 2).
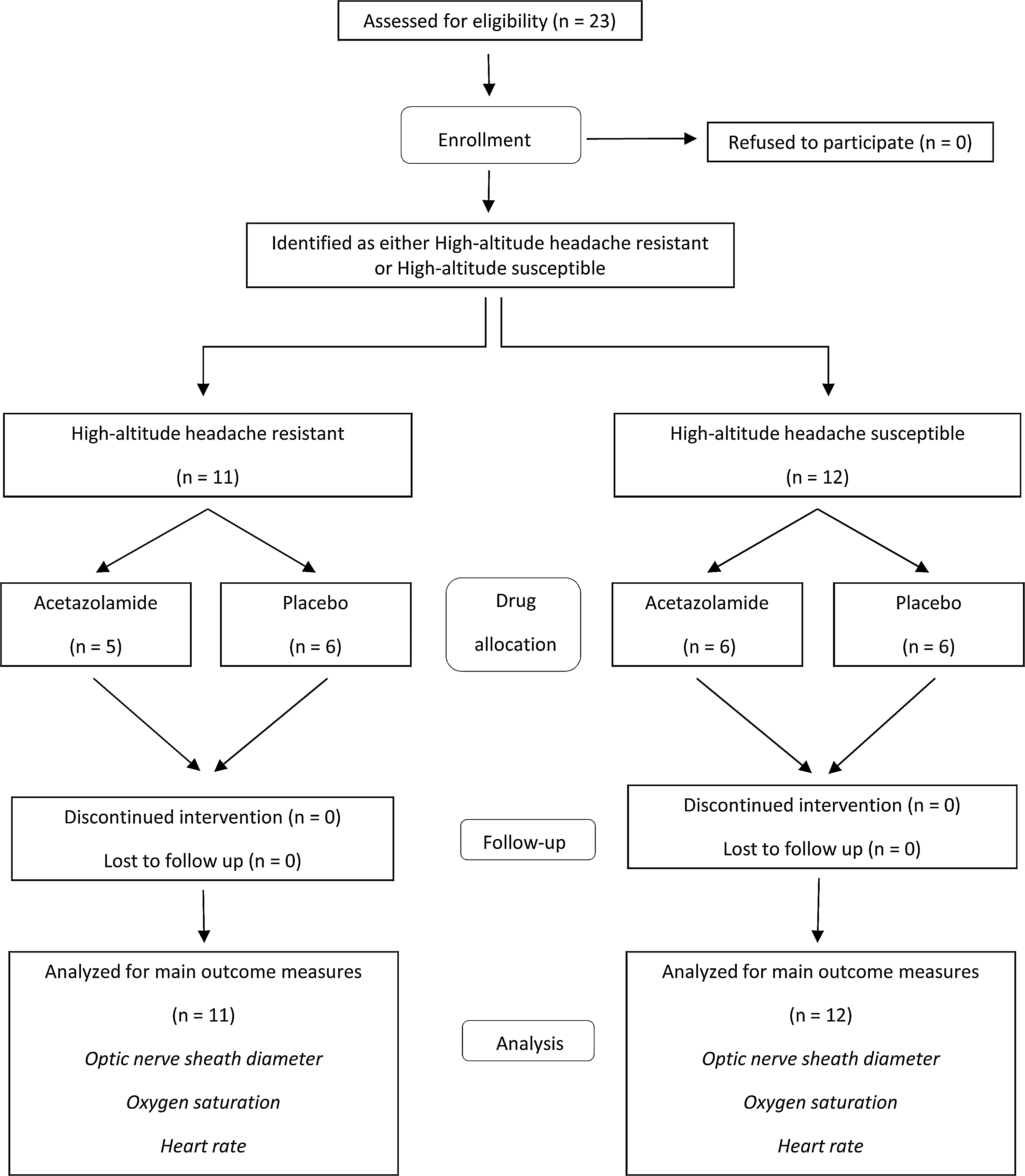
Participant flow through the drug study.
Finally, participants continued to be observed up to 36 h until acclimatization was complete and headache symptoms had returned to sea level values.
Measurements
Outcome variables were measured during SL (3 and 12 h) and HA (3, 12, 24, and 36 h, whereby 24 and 36 h represented 9 and 21 h after drug administration) in a comfortable, quiet, and temperate living area separated from other participants. All measurements were taken and analyzed by investigators blinded to headache severity and drug allocation.
Optic nerve sheath diameter
ONSD was measured by B-scan ultrasound (Micromaxx, Sonosite Inc., Bothell, WA) as described previously (Blaivas et al., 2003; Geeraerts et al., 2007). Briefly, after 30 min of supine rest, the rear of the optic globe was imaged in triplicate by placing a 7.5 MHz transducer lightly over the right closed eyelid. ONSD was measured perpendicular, 3 mm behind the optic globe, and subsequently calculated as the arithmetic mean of the three scans performed at each time point. Calculation of intra-observer variability revealed a mean difference between repeat SL scans of 0.1±0.02 mm and coefficient of variation of 4%.
Oxygen saturation and heart rate
Following quantification of optic nerve sheath diameter, oxygen saturation (Sp
Headache
HAH was assessed by visual analogue scale, as described above. Investigation of HAH rather than more severe altitude illness was confirmed by negative heel-to-toe walking and Sharpened Romberg Tests (Bird et al., 2011; Wu et al., 2006), in all participants, at 3, 12, 24, and 36 h during HA.
Hydration status
Urine output and osmolality were measured throughout SL and HA. Participants were given a container in order to collect urine volume over every 3 h period during waking hours, and osmolality was taken from the final sample at each time point (Osmocheck, Vitech, Scientific Ltd, Japan). During sleeping hours, cumulative overnight urine volume was added to the 8
Statistical analyses
All data are means and standard deviations (SD) and all statistical procedures were carried out on SPSS version 18 for Windows (Statistical Package for Social Sciences, IBM, Chicago, IL). Statistical significance was accepted at p=0.05. Following assumption checks including assessment of normality, main outcome measures were compared via 2 (acetazolamide vs. placebo) x 2 (HAH+ vs. HAH-) x 6 (time; SL, 3 and 12; HA, 3, 12, 24, and 36 h) analysis of variance with repeated measures on the third (time) factor. However, as there were no significant three factor interactions, for clarity only the two factor interactions are presented herein (drug x time and headache presence x time). Adjustments to the degrees of freedom were made when assumptions of sphericity were violated. Post Hoc ANOVA's and Tukey's t-tests were used to follow up significant differences. Statistical analyses were also run on the extremes of HAH scores, that is, those who suffered no headache throughout the entire HA exposure were compared to those with the greatest headache scores (HAH-, n=5, VAS=0/100±0) mm; HAH+, n=5, VAS=20/100±10) mm). As no differences were observed in interpretation of results, data are not shown. Confidence intervals (CI) and effect sizes are presented where appropriate to aid interpretation. Relationships between variables were analyzed by longitudinal linear regression analyses calculated using generalized estimation equations (Twisk, 2003).
To determine sample size, an un-blinded pilot study was completed in 2009 at the same location, using a similar protocol, on 16 participants, in whom headache intensities were obtained by Lake Louise Questionnaire. From these data, two sample size calculations providing a power of 0.8 were completed using the tables of Bausell and Li (2002). First, for the drug (acetazolamide vs. placebo)×time (baseline, 12, 24, 36 h) interaction, effect size was estimated to be 1.01 (calculated by combining the headache susceptibility groups and the sea level and high altitude time points and thus collapsing the analysis to a 2×2 interaction, with adjustment for the actual correlation between the dependent measures of r=0.9), giving a required sample size of 5 participants per cell (total n=20). Second, for the headache susceptibility (susceptible vs. resistant) x time interaction, effect size was estimated to be 1.79, giving a required sample size of three participants per cell (total n=12).
Results
Effect of altitude exposure
As expected, exposure to altitude decreased oxygen saturation (main effect of time, F=204.4, p<0.01), increased heart rate (main effect of time, F=13.3, p<0.01), and promoted diuresis (main effect of time, F=53.4, p<0.01: Table 1).
Values are means±SD. SpO2, oxygen saturation. *, indicates difference (P=< 0.05) compared to sea level average.
Effect of high altitude headache susceptibility
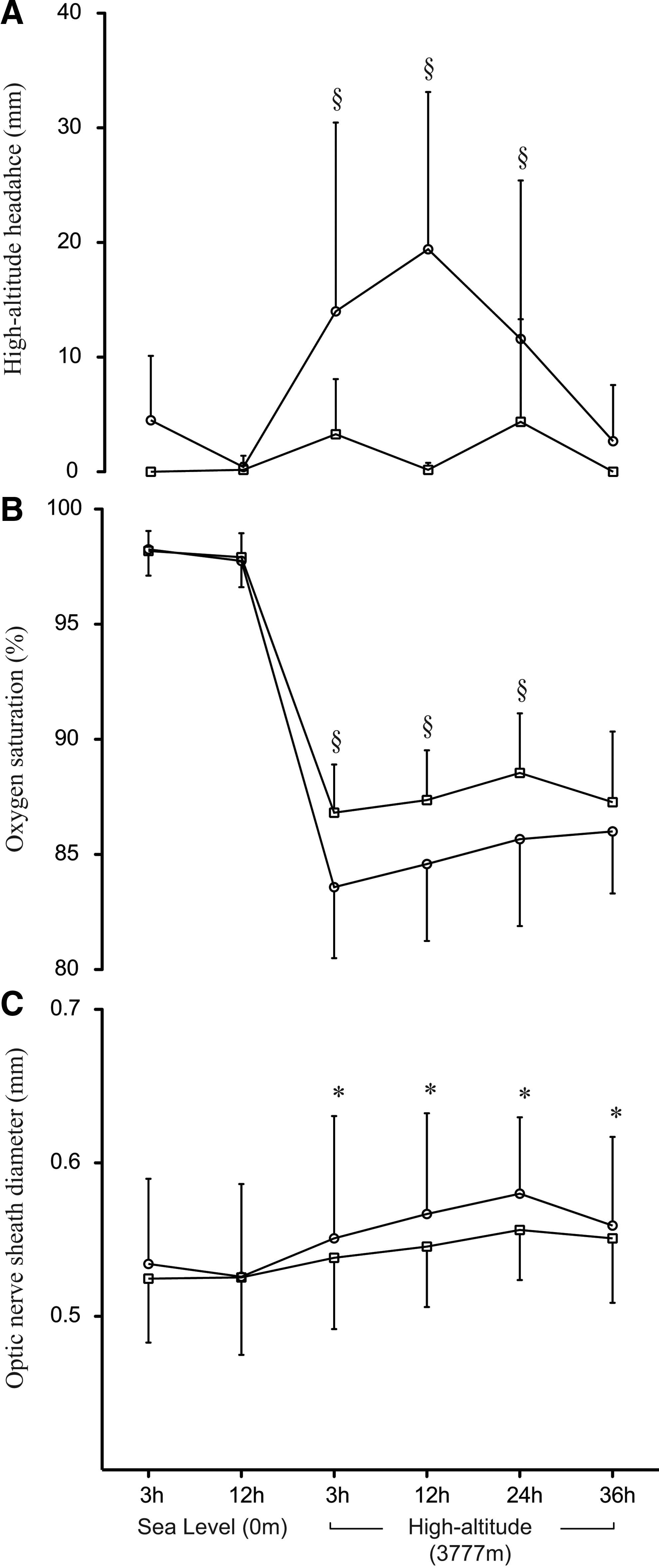
In comparison to HAH-, HAH+ reported elevated headache during HA from 3 to 24 hours (susceptibility by time interaction, F=4.23, p<0.01: Fig. 3A) and had lowered oxygen saturation (susceptibility by time interaction, F=2.93, p=0.03: Fig. 3B). Conversely, although ONSD was significantly increased at all altitude time points (main effect of time, F=4.09, p<0.01), this increase occurred in both groups with no difference in response between HAH-r and HAH-s (susceptibility by time interaction, F=0.31, p=0.90. Fig. 3C). Of note, for ONSD, effect sizes (Cohen's d) between groups at each time point were small (3 hours, 0.16; 12 hours, 0.40; 24 hours, 0.50, 36 hours, 0.12) and confidence intervals between groups at each time point overlapped (e.g., 95% CI at 24 hours: HAH+=5.4–5.8 mm; HAH-=5.5–6.1 mm).
Headache intensity
Effect of drug allocation
Acetazolamide promoted diuresis during HA at 24 h (drug by time interaction, F=9.72, p<0.01), and consequently decreased urine osmolality (drug by time interaction, F=4.01, p<0.01, Table 2). Indeed, during HA at 24 h, urine output increased to 1.4 L in the acetazolamide group compared to only 0.6 L in the placebo group.
Values are means±SD. ONSD, optic nerve sheath diameter, HAH, high-altitude headache, SpO2, oxygen saturation, Act, acetazolamide; Pla, placebo. Drugs were administered at 15, 20 and 28 hrs.
In contrast, HAH (drug by time interaction, F=0.52, p=0.63), ONSD (drug by time interaction, F=0.14, P=0.98), and heart rate (drug by time interaction, F=1.24, p=0.29) remained unaffected by drug allocation (Table 2). Statistically, arterial oxygen saturation remained unaffected by drug allocation (drug by time interaction, F=1.55, p=0.20). However, unplanned post hoc ANOVA's suggested that arterial oxygen saturation was significantly increased at 36 hours in participants allocated to acetazolamide.
Effect of acclimatization
When examining HAH over time, headache intensity increased from 3 to 24 h, where after intensity was attenuated by acclimatization to SL values (main effect of time, F=6.51, p<0.01, Table 3). However, despite this amelioration in HAH, ONSD remained significantly elevated throughout exposure to HA (Table 3).
Values are means±SD, plus 95% CI (confidence interval). Effect sizes (by Cohen's d) refer to each time point in comparison to average at sea level, and can be interpreted as small (>0.3), medium (>0.5) and large (>0.8). ONSD, optic nerve sheath diameter, HAH, high-altitude headache. *, indicates difference compared to sea level average, p≤0.05.
Longitudinal regression analyses
Finally, although a 1% decrease in oxygen saturation was associated with an increased headache intensity of 1.4 mm (longitudinal regression coefficient, β=−1.39, p<0.01), no relationships were detected between changes in ONSD and HAH (longitudinal regression coefficient, β=0.59, P=0.57).
Discussion
After 12 hours, our model induced headaches ranging from mild to moderate in half of the 23 participants, which is a similar incidence as observed in previous studies at this altitude (Maggiorini et al., 1990). Furthermore, although no previous data have reported headache intensity via a visual analogue scale at this altitude, we observed a 20-fold increase in headache score in comparison to sea level.
The finding that ONSD and thus indirectly intracranial pressure increased with altitude exposure in this study is consistent with previous investigations examining intracranial pressure in hypobaric hypoxia (Fagenholz et al., 2009; Hartig & Hackett, 1992; Singh et al., 1969; Sutherland et al., 2008; Wilson & Milledge, 2008; Wright et al., 1995). The reason for such an increase remains to be determined, but considering that raised intracranial pressure represents an increase in one or more of the cranial compartments (brain, blood, cerebrospinal fluid, or intra/extracellular water), elevations in intracranial pressure may reflect the increased cerebral blood flow observed in some studies at this altitude (Jensen et al., 1990; Severinghaus et al., 1966). It has also been suggested that venous hypertension may have a role to play in elevating cerebral blood volume and thus intracranial pressure (Wilson et al., 2009; Wilson et al., 2011). Finally, it is possible that the minor increase in brain edema observed previously (albeit at higher simulated altitude) may contribute to elevated intracranial pressure and expansion of the optic nerve sheath (Kallenberg et al., 2007; Schoonman et al., 2008).
However, our data provide three pieces of evidence seemingly in contrast with the hypothesis that intracranial pressure is causally associated with illness at altitude. First, in the present study, ONSD increased similarly in participants irrespective of HAH development. This data is supported by a recent study using ophthalmodynamometry to predict intracranial pressure at altitude (Querfurth et al., 2010), but is in contrast to the two previous investigations reporting a correlation between ONSD, HAH, and/or AMS (Fagenholz et al., 2009; Sutherland et al., 2008). Assuming the previous findings were not an artifact of a cross-sectional analysis, other explanations for the disparate data must exist. For example, it may be possible that mild HAH does not share the same mechanism with moderate to severe AMS and high altitude cerebral edema (which has been more consistently associated with raised intracranial pressure) (Houston & Dickinson, 1975; Singh et al., 1969). Supporting this speculation, participants with mild AMS studied previously (Fagenholz et al., 2009) had similar ONSD as nonsymptomatic participants, while those with higher AMS scores had elevated ONSD; meanwhile ataxia was correlated with ONSD, suggesting those participants with higher AMS scores may have had sub-clinical cerebral edema.
Second, HAH decreased with acclimatization, yet ONSD remained elevated. This observation is strikingly similar to that identified previously by Sutherland et al. (2008) during gradual acclimatization to 6400 m. Thus, elevated intracranial pressure per se cannot be the cause of mild to moderate headache, as the ‘stimulus’ remains in participants despite cessation of the ‘symptom’.
Third, in the present data, longitudinal regression analyses revealed that HAH is not correlated with optic nerve sheath diameter, but is correlated with physiological variables such as oxygen saturation. Thus, a 1% decrease in arterial oxygen saturation was associated with an increased headache intensity of 1.4 mm on the 0–100 mm scale, which supports other recent findings (Oliver et al., 2012).
Limitations of the present study include use of an indirect measure of intracranial pressure (optic nerve sheath diameter). However, the technique is noninvasive, portable (allowing use in field studies that are arguably more relevant than laboratory manipulations), and well validated (Blaivas et al., 2003; Geeraerts et al., 2007). Additionally, within the main analysis, acetazolamide used as a treatment did not reduce headache as expected, possibly due to the nature of the mild headaches observed herein. However, acetazolamide had an expected physiologic effect (as evidenced by greater urine output and by post hoc analyses revealing an increase in oxygen saturation). Irrespective of the drug component of this study, the detailed and pre-planned longitudinal analysis including observations completed during acclimatization, and separation of participants into headache-positive and headache-negative groups, provided other reasonable tests of causality. Finally, the sample size of 23 participants could be argued as small, especially as visual analysis of the ONSD data suggests some differentiation between the headache groups (Fig. 2). However, the difference in ONSD between headache groups equated to only 0.2 mm, which is unlikely to be of clinical importance, and effect sizes were small with confidence intervals substantially overlapping. Furthermore, the power calculations from carefully collected pilot data suggested sample size was sufficient to identify differences between groups. Thus, we believe these limitations are outweighed by the study strengths: use of a well-controlled environment, a powerful longitudinal within subjects analysis that also allowed between subjects comparisons with a control group, double baseline data to account for diurnal variations and calculation of inter-observer variability, and most importantly, a specific definition of HAH.
Conclusion
The present findings, interpreted together with previous data, raise intriguing possibilities about the cause of altitude illness. Currently it remains unclear whether HAH and AMS, of differing severities, share similar etiologies. Whether transient elevations in intracranial pressure play a role in altitude illness has also received little investigation. Nonetheless, the present study does not support the hypothesis that all HAHs are due to elevations in intracranial pressure.
Footnotes
Acknowledgments
This research was supported by the North Wales Grants Committee. We thank the Compagnie du Mont-Blanc for their hospitality and the opportunity to conduct research at the Aiguille du Midi; SonoSite for providing the use of ultrasound equipment, and Goldshield Pharmaceuticals Limited for providing acetazolamide to complete pilot studies. We would also like to show our grateful appreciation to all study participants and researchers.
Disclosure Statement
The authors do not have any conflicts of interest or financial disclosures to declare.