
Abstract
Abstract
Meyer, Joel. Twice-daily assessment of trekkers on Kilimanjaro's Machame route to evaluate the incidence and time-course of acute mountain sickness. High Alt Med Biol 13:281–284, 2012.—Acute mountain sickness (AMS) in high altitude trekkers is common, often trek-limiting, and occasionally fatal. The incidence of AMS can be modified by prudent ascent profile and route selection. It is not known whether the 6-day Machame route may enhance acclimatization on Kilimanjaro (5895 m) by ‘sleeping low’ on the third day. This report presents real time twice-daily AMS data from 28 healthy adult trekkers on the Machame route. The incidences of AMS and severe AMS were: 0% and 0% (day 1); 11% and 4% (day 2); 25% and 4% (day 3); 25% and 0% (day 4); 86% and 61% (summit day 5); and 7% and 0% (day 6), respectively. High altitude cerebral edema occurred in 4 of 28 trekkers (14%). On summit day, the median Lake Louise Symptom Score (LLSS) was 8 (range 2 to 15). Twice-daily measurements of AMS symptoms provide detailed insight into the time-course and evolution of AMS during ascent on Kilimanjaro. The 6-day Machame route may delay the onset but does not ultimately protect against AMS. The extremely high incidence and severity of AMS on summit day is of major concern to trekkers, portering staff, expedition medical staff, and leaders.
Introduction
One such trek is the popular ascent of Mount Kilimanjaro, about which safety concerns have been voiced (Karinen et al., 2008; Davies et al., 2009; Jackson et al., 2010; Shah et al., 2011). Over 30,000 trekkers attempt the summit each year (Daniels, 2011) and there have been numerous fatalities due to the serious sequelae of AMS (Hauser et al., 2004). Several routes exist to the summit of 5895 meters, ranging from 5 to over 10 days. Longer routes may be associated with a lower incidence of AMS (Mackie et al., 2009). Reasons for choosing a shorter itinerary may include: limited availability of huts and campsites, the pro rata nature of the Kilimanjaro national park fee, commercial pressures, competitiveness among groups, disproportionate expectation and desire to succeed, and limited experience of expedition organisers. Few routes include a rest day, despite consensus guidelines recommending that ascent over 3000 m should be graded (no more than 500 m per day) and interrupted (rest day every 3 to 4 days) (Luks et al., 2010). On this basis, at least 10 days would be required for a safe ascent of Kilimanjaro.
The most rapid and most popular ascent route is the Marangu route, which typically takes 5 days and is associated with appreciable high altitude morbidity. It is hypothesized that the Machame route may enhance acclimatization because trekkers sleep in camps at a similar altitude on both the second and third nights, adhering to the “climb high sleep low” paradigm for that 24 hour period (Karinen et al., 2008). There are no published data for this route, although it is the second most popular route up Kilimanjaro (Shah et al., 2011). This article presents real-time twice-daily AMS data from a moderately large trekking group attempting Kilimanjaro via the six day Machame route.
Materials and Methods
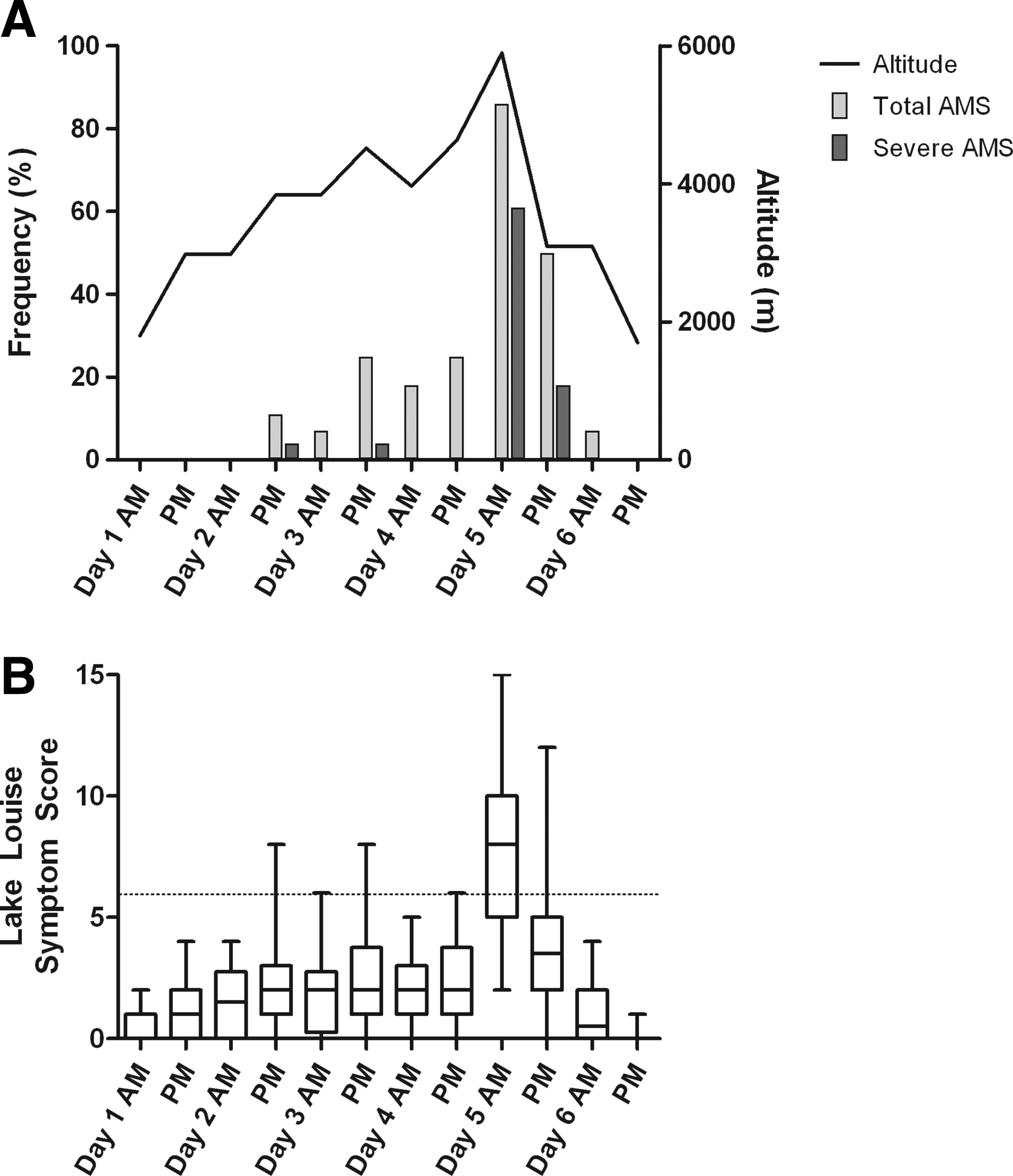
In June 2010, 28 healthy unacclimatized lowland adults from the UK attempted an ascent of Kilimanjaro by the 6-day Machame route (ascent profile depicted in Fig. 1A). Only two participants had previously trekked above 3000 m. All 28 were nonsmokers and had been deemed suitably healthy to participate in the trek by their general practitioner. As part of the daily routine medical supervision provided to the trekkers by the expedition team, symptoms of AMS were recorded in real-time every morning and evening for the duration of the 6-day trek. Symptoms were rated according to the Lake Louise Symptom Score (LLSS) (Roach et al., 1993). All trekkers consented to have their data collected as part of the medical care on the trek. Acetazolamide and other medication including analgesics, taken by trekkers, were also solicited (but not controlled). AMS was defined as the presence of headache plus one or more symptoms of AMS and LLSS>3; severe AMS was defined as headache and LLSS>6 or evidence of cerebral or pulmonary edema (Maggiorini et al., 1998).
Results
The trekking group comprised 28 adults (11 females, 17 males) with a median age of 33 (range 22–68). All trekkers reached Barafu camp (4633 m), the base for the day 5 summit attempt. On summit day, three trekkers did not reach Stella Point (5685 m) due to exhaustion, and one other trekker did not reach the summit (5895 m) due to ataxia.
The incidence of AMS during the trek (as defined by presence of headache and LLSS>3) was 0% on day 1 (1800 to 2980 m), 11% on day 2 (2980 to 3840 m), 25% on day 3 (3840 to 3970 m via 4520 m pass), 25% on day 4 (3970 to 4630 m), and 86% on summit day 5 (4630 to 5895 m). By morning of day 6 (3090 m), the incidence was 7%. These data are summarized in Figure 1A. Only two trekkers experienced no AMS.
The incidence of severe AMS (as defined by LLSS>6) was 0% on day 1, 4% on day 2, 4% on day 3, 0% on day 4, 61% on day 5, and 0% on day 6 (Fig. 1A). HACE (as defined by headache, ataxia, marked lethargy, and altered mental status) occurred in 4 of 28 trekkers (14%). All four cases were diagnosed between 1 hour before and 2 hours after reaching the summit and recovered completely following emergency descent and treatment with acetazolamide and dexamethasone. There were no cases of HAPE.
From days 1 to 4, the severity of AMS is approximately constant (median LLSS=2, range 0–8), then increases sharply on summit day when median LLSS=8 (range 2–15) (Fig. 1B). Alongside headache, the most common reported AMS symptoms were difficulty sleeping and fatigue or weakness. 50% of trekkers took regular prophylactic acetazolamide doses (125 mg or 250 mg twice-daily) according to their own wishes from the evening of day 2. Paradoxically, this group had increased severity of AMS on summit day compared to those abstaining from acetazolamide or using it for treatment of established AMS only (median LLSS 9 vs. 6, p=0.01 Mann Whitney U test).
Discussion
This report provides the first published analysis of the incidence and evolution of AMS on Kilimanjaro's Machame trekking route, attempted by over 7000 trekkers per year. AMS was extremely frequent, having occurred in a quarter of trekkers by day 4 (at 4000 m) and rising to almost 86% on summit day. The peak incidences of the life-threatening conditions severe AMS and HACE were 61% and 14%, respectively. This compares with published studies which estimate the overall incidence of AMS on the Marangu route to be between 41% and 84 % (Karinen et al., 2008; Kayser et al., 2008; Davies et al., 2009; Kalson et al., 2009; Jackson et al., 2010) and the summit incidence of HACE via the Marangu route to be 18% (Karinen et al., 2008). The median LLSS on summit day was 8, comparable with a median summit score of between 6 and 7.8 in other Kilimanjaro studies (Stokes et al., 2008; Kalson et al., 2009).
These data add to the weight of evidence that Kilimanjaro is a hazardous trek with the great majority of trekkers suffering significant symptoms of AMS, regardless of acetazolamide usage. This is of importance to trekking agents, portering staff, expedition medical experts, and trekkers, as increasing awareness of AMS can reduce its incidence (Vardy et al., 2005). There is a crucial need for routes with more conservative ascent profiles and which provide additional opportunities to acclimatize (including the option of a pre-acclimatization trek on the nearby 4566 m high Mount Meru).
The twice-daily data permit a detailed analysis of the evolution and time-course of AMS on the 6-day Machame route. Figures 1A and 1B show that AMS stayed constant rather than increasing between day 3 and day 4, contrary to expectations on a steadily ascending summit route, such as Marangu. This plateau is a followed by a worryingly sharp rise in AMS and HACE incidence on day 5. This could represent the delayed effect of similar sleep altitudes on day 2 and day 3. It also reflects the challenging ascent profile of the mountain which makes Kilimanjaro particularly hazardous. Thus, the Machame route may temporarily improve acclimatization by abrogating AMS on day 4, but with no ultimate protective effect on AMS once very high altitude is reached.
The main limitation of this study was lack of controlled design; therefore the apparent association between prophylactic acetazolamide use and increased AMS scores should be treated cautiously. The impact of concomitant analgesic usage by trekkers in this cohort could not be accurately estimated. The findings are also of limited generalizability as the data are from a single group of just 28 participants and Kilimanjaro is unusual in being a free-standing mountain that presents little opportunity to achieve early acclimatization, in comparison with other popular trekking destinations. Additionally, severe AMS, HACE, and HAPE might be underdiagnosed on group treks because of under-reporting of symptoms, lack of self-awareness of symptoms (a feature of HACE), inadequate medical supervision, and poor recognition by staff. The strengths of this study include the real-time twice-daily nature of the data collection, ensuring a near-continuous and complete data set as opposed to typical ‘point-prevalence’ studies at altitude where the incidence of AMS is measured at one or more ‘checkpoints'. In these studies participants are lost to follow up and there is a reliance on symptom recall which could lead to under-estimation. Daily or twice-daily soliciting of symptoms may provide a better estimate of cumulative incidence, severity and evolution, as well as real-time recognition and treatment of AMS.
Conclusion
There was a very high incidence of AMS and severe AMS/HACE during the summit phase of the Machame route on Kilimanjaro, despite suggestions that this route might enable better acclimatization. Sleeping at similar altitudes on days 2 and 3 may temporarily stall the onset of AMS but has no eventual protective effect. These findings are of relevance to the tourist trekking community. The high incidence of severe AMS and HACE is of particular concern given the pressure to summit on such treks, combined with the malignant nature of these conditions if left untreated.
Footnotes
Acknowledgments
The trekkers of St Andrew's Hospice, Airdrie, Lanarkshire are thanked for their kindness, enthusiasm, and cooperation; Nicola Smith and Kenneth Lord, trek leaders, for their expertise, support, and assistance with the data collection; the porters, guides, and staff of Ahsante Tours; and the staff at Action Challenge UK.
Disclosure Statement
No competing financial interests exist.