
Abstract
Abstract
Wagner, Dale R., Masaru Teramoto, Jonathan R. Knott, and Jack P. Fry Comparison of Scoring Systems for Assessment of Acute Mountain Sickness. High Alt Med Biol. 13:245–251, 2012.—The purpose of this study was to compare three commonly used scoring systems of acute mountain sickness (AMS)—the 5-item Lake Louise Self-report (LLS), the 11-item abridged version of the Environmental Symptoms Questionnaire (ESQ-III), and a 100 mm visual analog scale (VAS)—on climbers (N=63; 34.6±9.9 years) making a 1-day ascent of a 5640 m peak after a rest of ∼10 h at 4260 m. The prevalence of AMS was 63% when defined as LLS ≥3, 49% when defined as either LLS ≥5 or ESQ-III ≥0.7, and 41% when defined as the combined LLS and ESQ-III criteria. Despite the agreement in prevalence between the LLS ≥5 and ESQ-III ≥0.7, there was a discrepancy in AMS classification in 16% of the cases. A VAS cut-off point corresponding to the combined LLS and ESQ-III criteria was 16 mm. The sensitivity and specificity of the VAS for diagnosing AMS compared to combined LLS and ESQ-III criteria were 85% and 92%, respectively. All of the scoring systems were significantly correlated (τ=0.60 to 0.73, p<0.01); however, residual scores were large. We cannot recommend interchanging the diagnostic results from the LLS, ESQ-III, and VAS, and standardization is needed for the administration of the VAS.
Introduction
Presently, there is no validated laboratory test or other objective method to diagnose AMS. Identifying the presence and severity of AMS depends on the subjective rating of the severity of symptoms by the afflicted person. Over the years, researchers have developed questionnaires and rating systems in an attempt to assess AMS. The initial efforts were by Evans (1966) and Hackett et al. (1976). In the late 1970s and early 1980s, the United States military developed and refined an inventory of expected physiological and psychological symptoms when traveling to altitude called the Environmental Symptoms Questionnaire (ESQ) (Kobrick and Sampson, 1979; Sampson and Kobrick, 1980). The current version of this inventory, called the ESQ-III (Sampson et al., 1983), includes 67 items and an AMS rating scale. A shortened, 11-item, version of the ESQ-III limited to questions pertaining to cerebral function has been validated and is commonly used to assess AMS (Beidleman et al., 2007). Additionally, in 1991, a consensus committee met in Lake Louise, Canada, and agreed on a new, simplified, scoring system for AMS. This 5-item, self-report questionnaire has become known as the Lake Louise Self-report (LLS) (Roach et al., 1993), and it is one of the most commonly used methods to assess the presence and severity of AMS.
Despite the wide-spread use of the ESQ-III and the LLS, experts have questioned whether these scoring systems can accurately diagnose AMS, and neither is considered a “gold standard” (Bärtsch et al., 2004; Roach and Kayser, 2007). Recently, some researchers have required that the criteria of both tests be reached (i.e., LLS ≥5 and ESQ-III ≥0.7) to define AMS, creating a more rigorous standard (Schommer et al., 2010). It has been recommended that the specificity and sensitivity of AMS assessment be improved (Bärtsch et al., 2004). Both the ESQ-III and the LLS are ordinal, Likert-style, scales of measurement that require the subject to make a subjective ranking of the severity of symptoms. A continuous scale, such as choosing any point on a 100-mm line used as a continuum, would allow for smaller gradations in subjective judgment and might improve the sensitivity of AMS assessment. In fact, this type of visual analog scale (VAS) has been used to detect clinically relevant changes in pain in emergency rooms (Todd et al., 1996; Gallagher et al., 2001, 2002). We previously demonstrated that when a VAS is used in the field to quantify AMS symptoms the test-retest and interrater reliability are extremely high, and the VAS is significantly correlated to the LLS (Wagner et al., 2007). Roach and Kayser (2007) have recommended that researchers consider applying a VAS to high altitude studies and make comparisons to the LLS and abridged version of the ESQ-III. Thus, the purpose of this study was to assess AMS of climbers making a rapid ascent of a 5640 m peak using the 5-item LLS, 11-item ESQ-III, and a 100-mm VAS, to make comparisons of the three assessment scales, and to identify a VAS distance that corresponds to the combined LLS and ESQ-III criteria for AMS.
Materials and Methods
Setting and participants
Data collection took place inside the Piedra Grande climbers hut (4260 m) on the north side of Pico de Orizaba (5640 m), the highest point in Mexico. Every climber arriving to the hut intending to make a summit attempt was informed about the study and invited to participate. A letter of information and consent document were presented in both English and Spanish, and voluntary informed consent was obtained. One of the investigators was bilingual, and climbers who did not understand either English or Spanish were excluded from the study. The institutional review board of Utah State University approved this study.
Assessment scales
Three AMS assessment scales were administered. The LLS is a 5-item, 4-point, ordinal scale. The 5 symptoms are headache, gastrointestinal distress, fatigue or weakness, dizziness or lightheadedness, and difficulty sleeping. Each is scored 0 (not present) through 3 (severe or incapacitating) for a combined minimal score of 0 and maximal score of 15. The criterion for AMS is a headache with at least one other symptom and a total score of ≥3 (Roach et al., 1993); however, some researchers have used and recommended a total score of ≥4 or ≥5 to define AMS (Maggiorini et al., 1998; Dellasanta et al., 2007).
The short form of the ESQ-III is an 11-item, 6-point, ordinal scale. The 11 symptoms are lightheadedness, headache, dizziness, sensation of fainting, dim vision, reduced coordination, weakness, nausea, loss of appetite, feeling sick, and a “hungover” feeling. Each is scored 0 (not present) through 5 (extreme or maximum intensity). Each symptom has a factor weight assigned to it. The symptom score is multiplied by the factor weight, and then the products are summed. This sum is divided by 25.95 and multiplied by 5 to produce an AMS score. AMS is defined as a total score of ≥0.7 (Sampson et al., 1983). The lowest possible score is 0, and the highest possible score is 5.
The VAS, a continuous scale, is a 100-mm line anchored by the words “none” at one end and “severe/incapacitating” at the other. The instruction given to the subjects was to “place a single mark on the line at the point that best describes the magnitude of your sickness.” The VAS was scored by measuring the distance in millimeters from the “none” end of the line to the mark.
Procedures
Climbers traveled by truck from the village of Tlachichuca (2650 m) to the Piedra Grande hut (4260 m). As a result of this mode of travel, they rapidly gained 1610 m of elevation within about 2 h. Climbers arrived at the hut in the afternoon, went to sleep early, and got up to depart for the summit attempt in the middle of the night. The median time spent in the hut before the summit attempt was 9.9 h, and the median round-trip time from hut-summit-hut was 13.3 h. Thus, many of the climbers went from 2650 m (Tlachichuca) to 5640 m (Pico de Orizaba summit) and back to 2650 m in about a day and a half. The date and time of each participant's arrival to the hut was noted, and the initial data collection occurred within 30 min. The LLS, ESQ-III, and VAS were all administered at the same time in random order. The data collection was repeated immediately before the climbers departed for their summit attempt and immediately upon their return to the hut from their summit attempt for a total of 3 collection periods. The post-ascent data collection was retrospective and phrased so as to describe the climbers' perceived symptoms of sickness throughout the duration of their ascent above the hut.
Statistical analyses
A total of 73 climbers (64 males, 9 females) were examined in this study. As mentioned previously, AMS was assessed at three time points: upon arrival to the hut, immediately before departing the hut for the summit attempt, and immediately upon return to the hut from the summit attempt. It takes some time for AMS to develop after arrival at a high altitude, and most climbers spent less than 12 h in the hut. Although many climbers had started to develop AMS symptoms in the hut and the symptom scores during the second data collection were higher than upon arrival (Table 1), there were few cases that met the criteria for AMS during the first two data collections. Therefore, the analysis comparing the three AMS scoring systems was performed only on the post-ascent data. There were missing values for 10 climbers at this time, and these cases were excluded from the analysis. Consequently, the data of 63 climbers (34.6±9.9 years) were used for the analyses.
Values are Mean±SD (lowest score–highest score). AMS, acute mountain sickness; ESQ-III, environmental symptoms questionnaire III; LLS, Lake Louise Self-report; VAS, visual analog scale.
Arrival, upon arrival to the hut; Departure, immediately before departing the hut for the summit attempt; Return, immediately upon return to the hut from the summit attempt.
The relationships among the LLS, ESQ-III, and VAS were examined using a scatterplot and Kendall's tau (τ) rank correlation coefficient. In order to determine the VAS cut-off point corresponding to the AMS criteria for both LLS and ESQ-III (i.e., LLS=5; ESQ-III=0.7), a linear regression analysis was conducted to develop separate linear equations for predicting VAS (=outcome variable) from: 1) LLS, 2) ESQ-III, and 3) combined LLS and ESQ-III (=predictor variables). The preliminary analysis indicated that there appeared to be large and nonconstant residual scores between the LLS or ESQ-III scores and the predicted VAS scores (i.e., heteroscedasticity of residuals). Therefore, a weighted least squares regression analysis was used (Cohen et al., 2003; Tabachnick and Fidell, 2007) to develop the regression equation from LLS or ESQ-III, as the weight for each case was calculated by the reciprocal of the predictor variable raised to a power ranging −2 through 2. Then, a LLS value of 5 and an ESQ-III value of 0.7 were entered in each equation to determine the corresponding VAS scores. With respect to determining the VAS cut-off point from the combination of LLS and ESQ-III, it was found that a multiple linear regression analysis would not be appropriate for this data set due to multicollinearity (i.e., high correlation between LLS and ESQ-III), as the absence of multicollinearity is one of the assumptions of a multiple linear regression analysis (Cohen et al., 2003; Tabachnick and Fidell, 2007). Instead, we performed a Z-score transformation to combine the LLS and ESQ-III variables (Haynes et al., 2011). The scores on LLS and ESQ-III were transformed into Z-scores, and the Z-scores of the two variables for each subject were added together to form a single, composite variable (Z_LLS_ESQ-III). Then, a linear regression analysis was performed using Z_LLS_ESQ-III as a predictor variable and VAS as an outcome variable. After developing a linear equation for predicting VAS, the Z_LLS_ESQ-III score corresponding to a LLS value of 5 (Z=−0.11) and an ESQ-III value of 0.7 (Z=−0.36) was calculated (Z=−0.47) and entered in the regression equation to determine the corresponding VAS score. Furthermore, the specificity and sensitivity of the obtained VAS cut-off point were calculated for evaluating its ability to correctly identify AMS and non AMS cases, given that the AMS diagnosis was made by the combined LLS and ESQ-III criteria. All statistical analyses were done at the alpha level of 0.05 using IBM® SPSS® Statistics Version 19 (SPSS, Inc., IBM Corporation, Armonk, New York).
Results
A summary of the AMS scores for each data collection are summarized in Table 1. For the final data collection, there was a positive relationship (p<0.01) among all three scoring systems. The criterion of LLS ≥3 with a headache and at least one additional symptom resulted in 63% of the climbers being diagnosed with AMS. Increasing the cut-off to LLS ≥5 reduced the diagnosis of AMS to 49%, the same percentage as those with an ESQ-III score of ≥0.7. Despite the LLS and ESQ-III being positively correlated, there was a discrepancy in the diagnosis of AMS in about 16% of the cases regardless of which LLS cut point was used. The relationship between the LLS and ESQ-III is depicted in Figure 1.
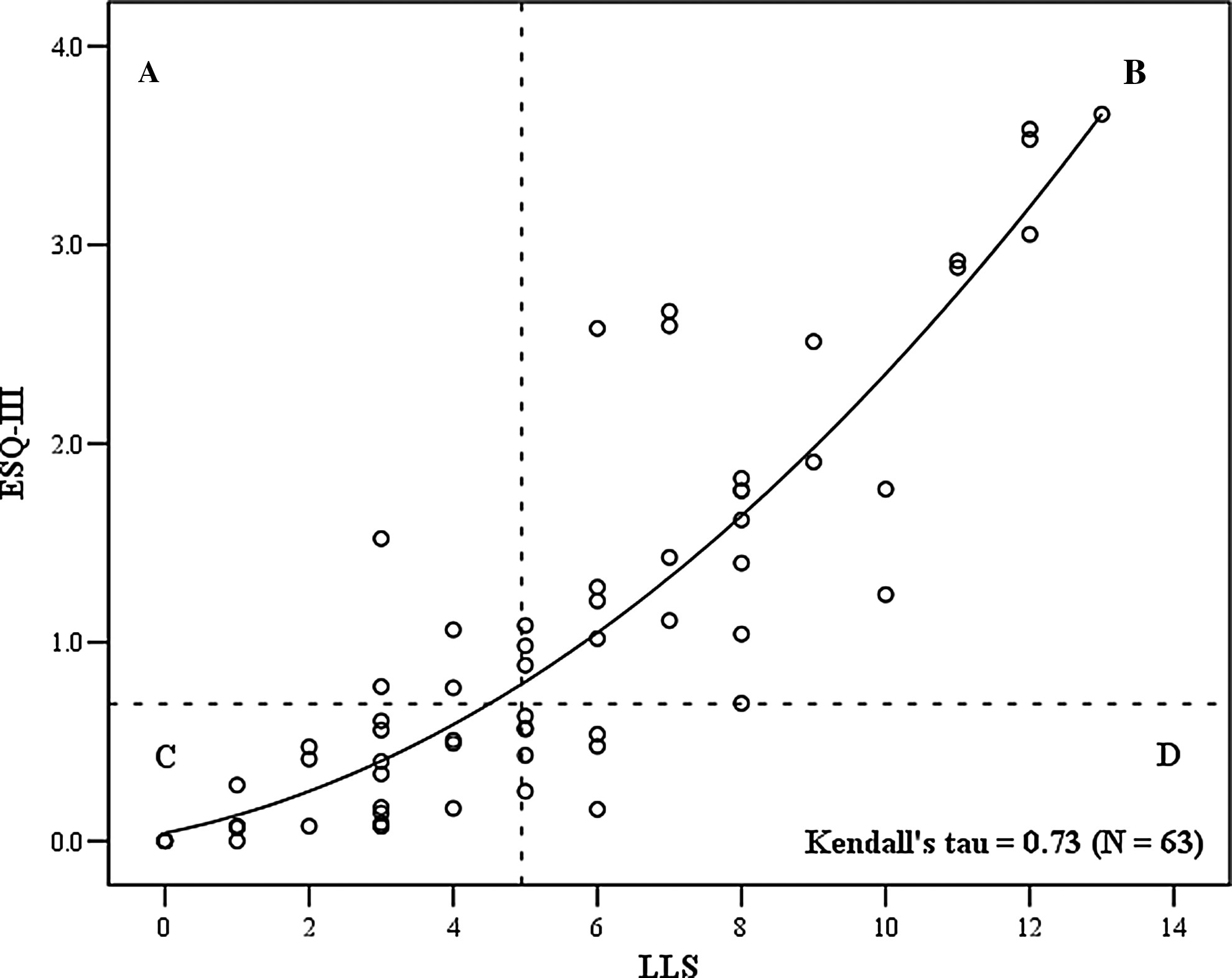
Relationship between the Lake Louise Self-report (LLS) and the environmental symptoms questionnaire (ESQ-III) for the assessment of acute mountain sickness (AMS). Dashed lines represent AMS criterion scores of ≥r5 for LLS and ≥0.7 for ESQ-III. There is a differential diagnosis discrepancy in AMS classification between LLS and ESQ-III for cases in
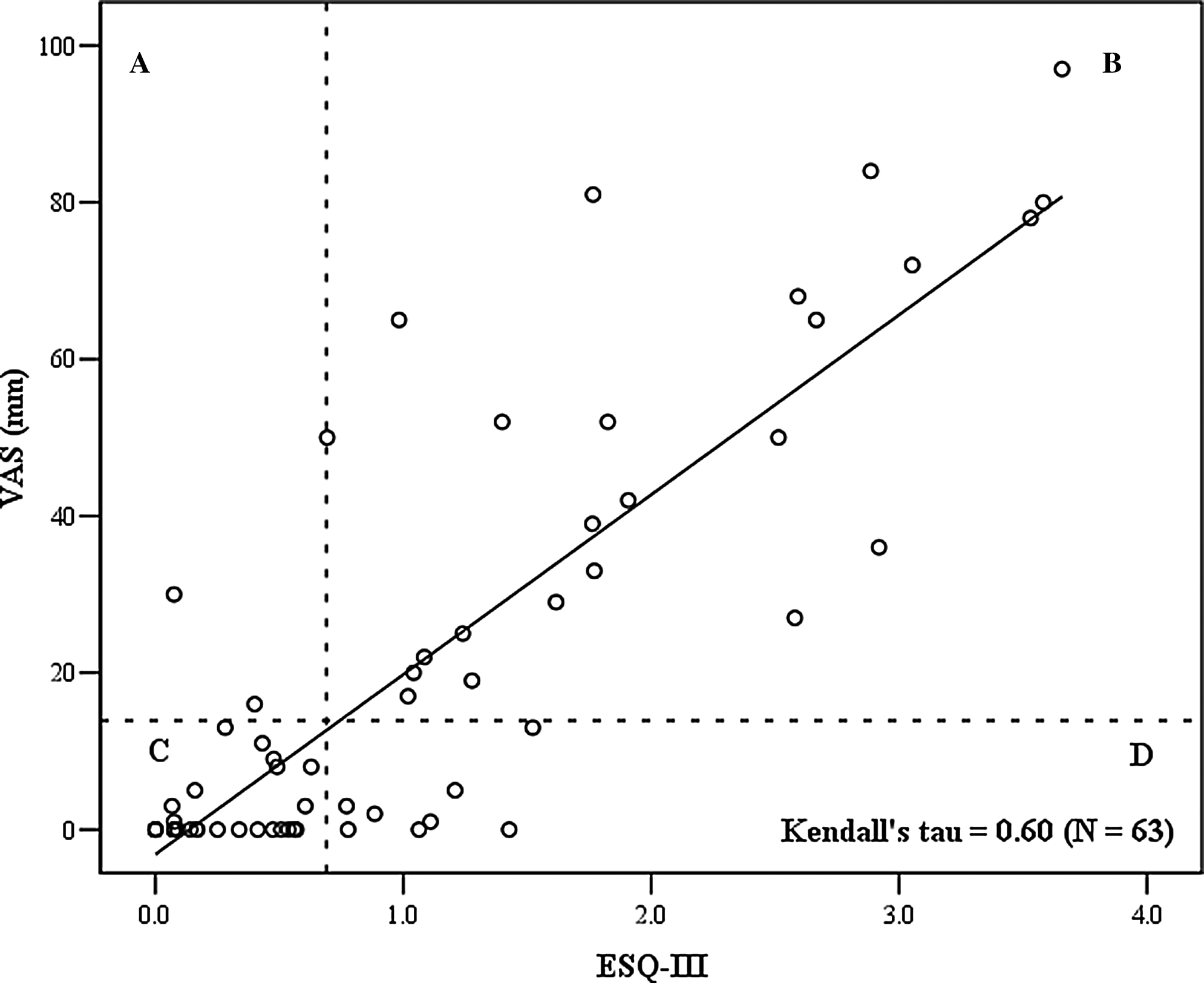
The scatterplots illustrating the relationships between LLS or ESQ-III and VAS are depicted in Figures 2 and 3; the correlations were significant (p<0.01). According to the linear regression analysis, the LLS [F(1, 58)=46.29, p<0.01, R2=0.444] and ESQ-III [F(1, 57)=92.51, p<0.01, R2=0.619] were significant predictors of VAS, explaining 44.4% and 61.9% of the variability in VAS by LLS and ESQ-III, respectively. The weighted normal probability and residual plots indicated that the assumptions of a linear regression analysis, normality, linearity, and homoscedasticity of the residuals, were not violated. In addition, no apparent outlying cases were identified, as standardized residuals of all cases were within the range of±3.3 (Tabachnick and Fidell, 2007). The VAS cut-off points corresponding to LLS of 5 and ESQ-III of 0.7 obtained from the regression equations (VAS=4.574×LLS – 4.822; VAS=21.364×ESQ-III – 1.037) were 18 mm and 14 mm, respectively. The sensitivity and specificity of these VAS cut-off points for AMS diagnosis were 63.9% and 96.3% (LLS ≥5) and 74.2% and 90.6% (ESQ ≥0.7), respectively.
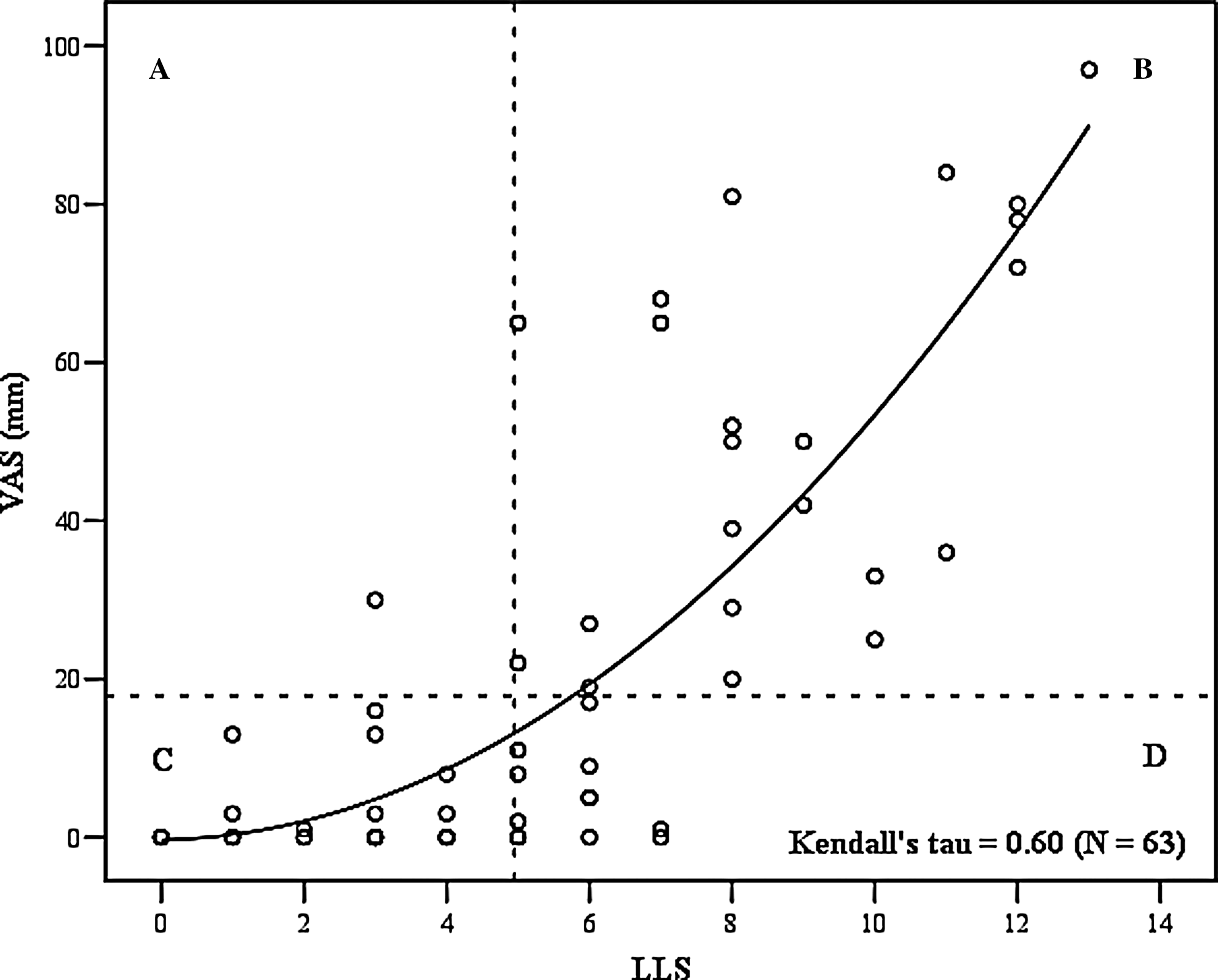
Relationship between the Lake Louise Self-report (LLS) and the visual analog scale (VAS). Dashed lines represent AMS criterion scores of ≥r5 for LLS and ≥14 18 mm for VAS. Assuming that LLS is the standard,
Relationship between the Lake Louise Self-report (LLS) and the square root of the visual analog scale (√VAS). Dashed lines represent AMS criterion scores of ≥r5 for LLS and ≥14 mm for VAS (or 3.74 for √VAS). Assuming that LLS is the standard,
The relationship of Z_LLS_ESQ-III to VAS is presented in Figure 4. There was a significant positive correlation between the two variables (p<0.01). According to the linear regression analysis, Z_LLS_ESQ-III was a significant predictor of VAS [F(1, 61)=144.00, p<0.01, R2=0.702], explaining 70.2% of the variability in VAS. Normality, linearity, and homoscedasticity of the residuals were ensured by the inspection of the normal probability and residuals plots (Cohen et al., 2003; Tabachnick and Fidell, 2007). Standardized residuals of all cases were within the range of±3.3, indicating no apparent outlying cases (Tabachnick and Fidell, 2007). The VAS cut-off point corresponding to the combined LLS and ESQ-III criteria (i.e., LLS=5 and ESQ-III=0.7; Z=−0.47) obtained from the regression equation (VAS=11.988×Z_LLS_ESQ-III+21.175) was 16 mm. The sensitivity and specificity of the VAS cut-off point for AMS diagnosis were 85.2% and 91.7%, respectively. There were 23 climbers who scored zero on the VAS; despite a zero score, one of them exceeded the AMS criteria on both the LLS and ESQ-III.
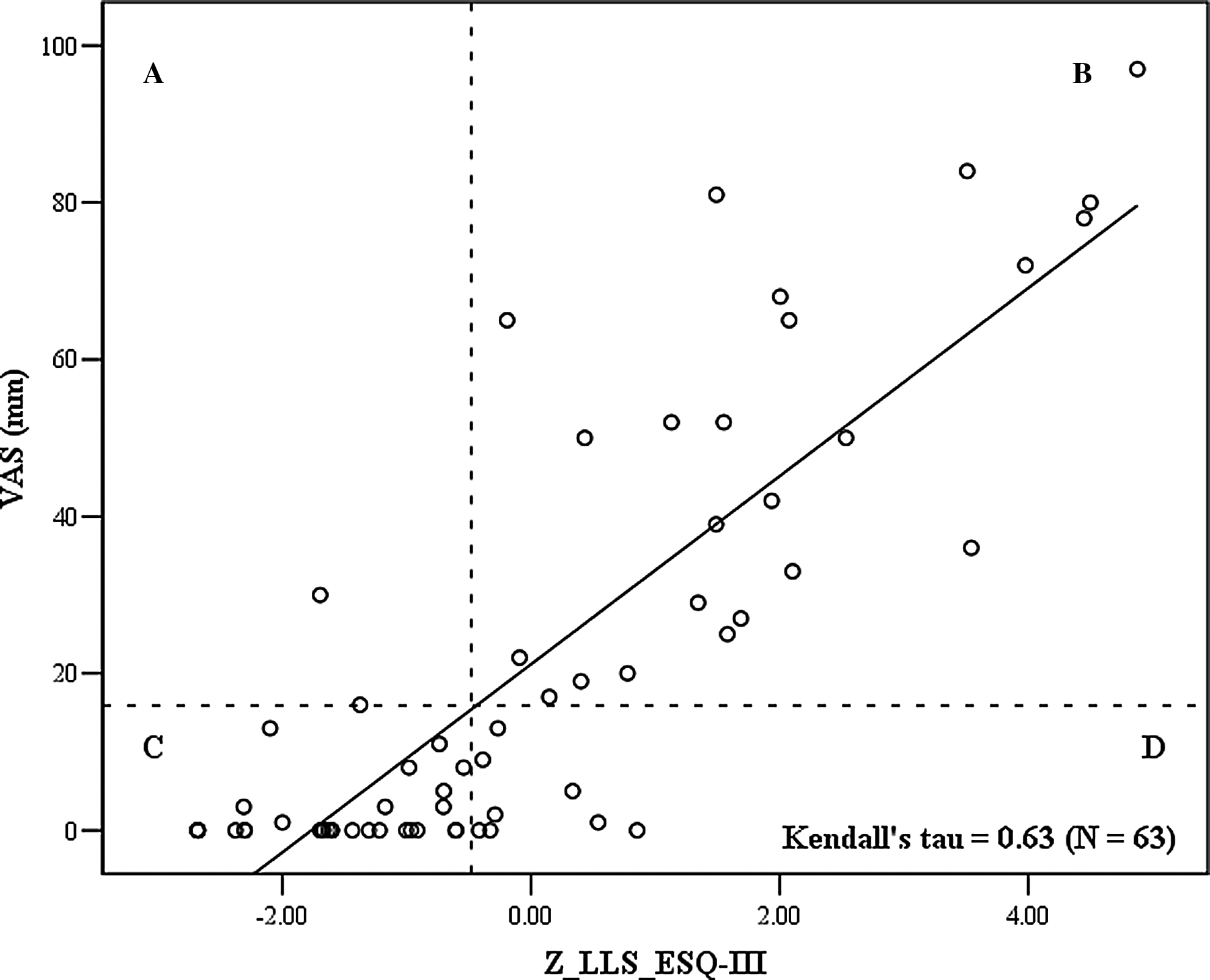
Relationship between the Z-score composite of the Lake Louise Self-report and the environmental symptoms questionnaire (Z_LLS_ESQ-III) and the visual analog scale (VAS). Dashed lines represent AMS criterion scores of −0.47 for the Z_LLS_ESQ-III and ≥r16 mm for the VAS. Assuming that Z_LLS_ESQ-III is the standard,
Discussion
High altitude and a rapid ascent rate combine to create an environment conducive to developing AMS. Such a combination existed on Pico de Orizaba resulting in a high prevalence of AMS among mountaineers; furthermore, AMS was often severe. This scenario allowed for the comparison of commonly used AMS scoring systems. Previous researchers have made comparisons between LLS and ESQ-III (Maggiorini et al., 1998; Dellasanta et al., 2007), LLS and VAS (Wagner et al., 2007; Kayser et al., 2010; Hext et al., 2011; Van Roo et al., 2011), and ESQ-III and VAS (Hext et al., 2011); however, this is the first published study to make quantitative comparisons among all three scoring systems.
LLS compared to ESQ-III
Historically, the most widely-used scales for assessing the presence and severity of AMS have been the ESQ-III and the LLS. An LLS ≥3 with a headache as one of the symptoms (Roach et al., 1993), or an ESQ-III ≥0.7 (Sampson et al., 1983) are both accepted definitions of AMS. However, experts acknowledge that neither scale should be regarded as a “gold standard” (Bärtsch et al., 2004; Roach and Kayser, 2007). Despite widespread use of these criteria, Maggiorini et al. (1998) stated that a fixed LLS criterion score was inadequate to define AMS in their study of 490 climbers who stayed at 4 huts at altitudes of 2850 m to 4559 m. Furthermore, Bärtsch et al. (2004) stated that these definitions identify different grades of AMS with the LLS ≥3 detecting mild AMS and the ESQ-III ≥0.7 indicative of more severe AMS. This was certainly the outcome of the present study as the prevalence of AMS was greater when using the LLS ≥3 definition compared to an ESQ-III ≥0.7. When the AMS cut-off was increased to LLS ≥5, the prevalence of AMS was equal between the two scoring systems; however, there was still a different AMS diagnosis for some subjects. These findings are nearly identical to those of other researchers who have compared the ESQ-III and the LLS (Maggiorini et al., 1998; Dellasanta et al., 2007). The discrepancy in AMS classification between the two scales in about 16% of the cases in the present study is similar to the 20% reported by Dellasanta et al. (2007; N=266). Additionally, the description and illustration of the relationship between the LLS and ESQ-III in the Dellasanta et al. (2007) report is very similar to the slight curvilinear relationship (see Fig. 1) that we observed.
VAS compared to LLS and ESQ-III
The medical community have used VAS for a number of years to assess pain (Todd et al., 1996; Gallagher et al., 2001, 2002), and to detect clinically significant changes in nausea (Hendey et al., 2005), sleep quality (Zisapel and Nir, 2003), and headache (Lines et al., 2001), which are symptom components of AMS. However, a VAS was not applied to the assessment of AMS until 2007 (Wagner et al.). As espoused by other researchers, the VAS offers advantages over the other AMS scoring systems and is an attractive option because it is a continuous measure allowing for smaller gradations of assessment, requires few words which would simplify translation when applied to multiple languages, is brief and simple to use (Roach and Kayser, 2007; Wagner et al., 2007; Van Roo et al., 2011).
Only recently have researchers made comparisons of the VAS to the LLS and ESQ-III. Consistent with the present study, there is agreement among researchers that the VAS is strongly correlated to the LLS (Wagner et al., 2007; Kayser et al., 2010; Hext et al., 2011; Van Roo et al., 2011) and the ESQ-III (Hext et al., 2011). However, Kayser et al. (2010; N=14) was critical of using a VAS to assess AMS because of a nonlinear relationship between the LLS and VAS. A nonlinear relationship between these two scoring systems was also observed in the present study (see Fig. 2), while the composite Z-score of LLS and ESQ-III (=Z_LLS_ESQ-III) seemed linear to VAS (see Fig. 4). In contrast, both Hext et al. (2011; N=23) and Van Roo et al. (2011; N=46) showed a linear relationship between the VAS and LLS, and like the current study (see Fig. 3), Hext et al. (2011) also reported a linear relationship between the VAS and ESQ-III. Inspection of the figures in the current study, as well as the figures from these other studies, reveals that the relationship between LLS or ESQ-III and the VAS is consistently linear when above the AMS threshold (i.e., LLS ≥5, ESQ-III ≥0.7). An increasing AMS score is indicative of an increasing degree of sickness. Thus, we suggest that the VAS could be used to detect and track clinically relevant changes in the severity of AMS once AMS has been confirmed. As Bärtsch et al. (2004) stated, “it is important to consider the level of illness that is investigated, because the underlying pathological processes may change when going from mild to severe disease.” This application of the VAS in AMS research has yet to be studied and is a potential area for future research.
From the results of the data analysis, it was determined that the VAS score for AMS identification corresponding to the combined LLS and ESQ-III criteria (i.e., LLS=5 and ESQ-III=7) was 16 mm. This VAS cut-off point would correctly identify approximately 85% of the climbers with AMS and almost 92% of them with no AMS in our study, given that the combined LLS and ESQ-III criteria were used to define AMS. The sensitivity and specificity of the VAS for identifying AMS is similar to that reported by others (Hext et al., 2011; Van Roo et al., 2011). However, our criterion value of 16 mm is substantially less than the cut-off values recently identified by Hext et al. (2011), who reported cut-off points of 22 mm compared to an LLS ≥3 and 33 mm for an ESQ-III of 0.7. Van Roo et al. (2011) suggested values of 35 to 43 mm for an LLS ≥5. Methodological differences in the administration of the VAS likely contribute to the differences in cut-off points among the studies. Hext et al. (2011) and Van Roo et al. (2011) both included VAS for individual AMS symptoms as well as an overall VAS for AMS in their studies; we used only an overall VAS. Also, Van Roo et al.'s instructions for completing the VAS used the words “altitude sickness,” and the instruction given to our subjects was to “place a single mark on the line at the point that best describes the magnitude of your sickness.” In hindsight, we recognize that many mountaineers with headaches, nausea, or other AMS symptoms may not have interpreted this as being “sick”; consequently, it was likely that many of the participants in our study underestimated their VAS values. Thus, although one of the benefits of the VAS is that few descriptive words are necessary, it is critically important that the instructions and anchor words for the VAS be standardized. Using the specific words “altitude sickness” for a global AMS VAS assessment would reduce ambiguity and likely lead to a more valid assessment, but this assumes that all participants are knowledgeable about AMS.
Finally, there was a considerable amount of scatter of VAS scores for a particular LLS or ESQ-III score. This is evident in the other studies as well (Wagner et al., 2007; Kayser et al., 2010; Hext et al., 2011; Van Roo et al., 2011;). As Van Roo et al. (2011) pointed out, a certain amount of scatter is to be expected when comparing a continuous scale with ordinal scales. Nevertheless, the residual scores between the VAS and LLS or ESQ-III are large, indicating considerable variability in the individual prediction of one from the other. There were also large and somewhat nonconstant residual scores observed between Z_LLS_ESQ-III (composite Z-score of LLS and ESQ-III) and VAS. Regarding the regression analysis, the presence of large and nonconstant residuals at each level of the predictor variable (i.e., Z_LLS_ESQ-III) can weaken the analysis by increasing the size of standard errors of regression coefficients (Cohen et al., 2003; Tabachnick and Fidell, 2007). We suspect that some individuals do not comprehend the concept of continuum scoring. Some standardized instruction with an example should be given on how to mark a VAS, and this might reduce some of the inter-individual variability.
Strengths and limitations
Our sample sizes for the linear regression analysis (N=63) was barely large enough for a regression analysis with one independent variable (Tabachnick and Fidell, 2007), limiting the generalizability of the results. Even so, our sample was larger than previously published studies that have evaluated the validity of the VAS for AMS assessment (Kayser et al., 2010, N=14; Hext et al., 2011, N=23; Van Roo et al., 2011, N=45). Furthermore, the severity of AMS in the present study was distributed fairly evenly across an LLS range of 0 to 13. This was a strength of the study as previous researchers have acknowledged that their studies were limited by a low number of severe AMS cases (Hext et al., 2011; Kayser et al., 2010; Van Roo et al., 2011), whereas 27% of participants in our study had LLS ≥8. The limitations of this study included not being able to obtain baseline measurements at a low altitude and retrospective, rather than real-time, analysis of symptoms following an ascent. It is possible that their perception of AMS symptoms during the ascent could have been clouded by post-climb euphoria, exertion, a “machismo” attitude minimizing their suffering, or a boasting attitude exaggerating their triumph over pain. Furthermore, there was no physician available to make an expert “diagnosis” of AMS which would have added some subjective bias but also provided an independent standard. Finally, as mentioned previously, the difference in the phrasing of the instructions for completing the VAS between the words “sickness” and “altitude sickness” make it difficult to compare VAS values across studies.
Conclusions and Recommendations
Despite significant positive correlations among all three AMS scoring systems, we cannot currently recommend interchanging the diagnostic results from the LLS, ESQ-III, and VAS. In agreement with previous research (Maggiorini et al., 1998; Dellasanta et al., 2007), we observed better agreement between ESQ-III ≥0.7 and LLS ≥5 than between ESQ-III ≥0.7 and LLS ≥3. This suggests that consideration should be given to changing the AMS criterion from LLS ≥3 to LLS ≥5 for better AMS classification agreement among scoring systems. Nevertheless, some subjects are still likely to receive a different AMS diagnosis when evaluated by both scoring systems. Expert physician assessment has been recommended to validate refinements of these scales (Maggiorini et al., 1998; Dellasanta et al., 2007). The VAS score corresponding to AMS, as defined by the combined LLS and ESQ-III criteria (both LLS ≥5 and ESQ-III ≥0.7), was 16 mm. This is substantially less than the diagnostic cut-off distances recently identified by others (Hext et al., 2011; Van Roo et al., 2011). The variability in cut-off points among studies are likely the result of how the VAS was administered, and this highlights the importance of the need for standardization. Given the wide variability in VAS cut-off points among studies, we have no confidence in using the VAS as an assessment of AMS at this time. Finally, we suggest that future research focus on using the VAS at multiple time points to track clinically relevant changes in severity once AMS has already been confirmed. This would help medical personnel identify those who are beginning to recover versus those who might be progressing to the more serious condition of cerebral edema.
Footnotes
Acknowledgments
We thank the climbers who took the time to participate in this study, and we are grateful to the following for providing financial support for the data collection: Wilderness Medical Society (Herbert N. Hultgren Award), American Alpine Club (standard research grant), and Mazamas (standard research grant).
Author Disclosure Statement
The authors have no conflict of interest to report.