
Abstract
Abstract
Heissen, Mohamed. Improved glycemic control in moderate altitude type II diabetic residents. High Alt Med Biol 14:27–30, 2013.—Exposure to altitude hypoxia may elicit changes in glucose homeostasis. This work is designated to investigate the glycemic control in type II diabetic patients (DMII) permanently resident at moderately high altitude (2400 m), and to investigate whether the arterial oxygen-related parameters are different in DMII patients living at altitude compared to those living at low altitude. Blood glucose, HbA1c, hemoglobin concentration, and hematocrit (HCT) were measured in moderate altitude type II diabetics and compared with both altitude nondiabetics and diabetic patients living at normoxic and normobaric conditions. The data revealed that fasting blood glucose was lower in altitude diabetic patients compared to diabetics living at low altitude (157±33 mg/dL and 176.81±15.98 mg/dL, respectively, p<0.01). Also, glycemic control was improved in altitude diabetic patients, where their HbA1c was lower than the corresponding low altitude diabetic patients (8.68±0.79% and 9.30±1.02% respectively, p<0.01). Low oxygen tension at altitude was compensated in both diabetics and nondiabetics by a significant increase in both hemoglobin and HCT (17.33±0.72 mg/dL and 50.7±2.20%, respectively) compared to the corresponding groups living at low levels (15.53±0.55 mg/dL and 45.8±1.64%, respectively). The underlying disease neither affected the arterial oxygen tension (Pa
Introduction
Healthy nondiabetic people, permanently living at high altitude appear to have lower blood glucose levels and decreased incidence of diabetes. In HA pregnant women, fasting C-peptide levels and β-cell function were similar to sea level pregnant women, whereas insulin and proinsulin were lower. Insulin sensitivity was higher and fasting plasma glucose was lower at high altitude (4370 m) than at sea level in the presence of similar insulin secretion (Krample et al., 2001). Also, after moderate altitude exposure, subjects suffering from metabolic syndrome had significant improvements in glycemic parameters where the glucose concentration was significantly lower compared to the basal values (Schobersberge et al., 2002). Living at moderate altitude (1500–2000 m) is well tolerated for the majority of diabetics. Beyond 2500 m, hypoxia-induced anorexia, side effects of medications, and the higher incidence of mountain sickness, can make diabetes control difficult (Thalmann et al., 2007).
Diabetic retinopathy is known as one of the major complications of long-standing uncontrolled diabetes mellitus. Although diabetic climbers going to high altitude may have an increasing risk for development of retinopathy (Leal et al., 2008), long-term residence at moderate altitude did not induce significant difference in retinopathy incidence (Sayarlioglu et al., 2005). Subsequently, glycemic control plays an important role in prevention of such complications. Several studies have investigated the risk of high altitude short-term residents such as mountains climbers. No studies, however, were undertaken at Assir province to investigate the effect of chronic altitude exposure on patients with pre-existing type II diabetes mellitus. Asir mountains extend along the western province of Kingdom of Saudi Arabia, where El Namas (2400 m) is considered one of the highest cities located onto these mountain series. In this report, type II diabetic permanent residents of this city were studied to investigate the glycemic control compared to diabetics living in normobaric conditions. The data presented in this work monitored blood glucose level, glycemic control, represented as HbA1c, hemoglobin concentration and HCT, in addition to Pa
Materials and Methods
Patient population and grouping
This study included 34 type II diabetic patients and 34 nondiabetic healthy subjects aged 50.06±9.8 years, range: 28–70 years. Subjects were 64 male and 4 female. They were categorized into four groups (Table 1). Groups I and II (n=18, each) included diabetic patients and nondiabetic subjects, living at moderate altitude (El Namas city, 2400 m above the sea level, standard barometric pressure 577 mmHg (77 kPa) (Fig. 1). Diabetic patients of group I were randomly selected from diabetic outpatients, regularly monitored for blood glucose at El Namas General Hospital. Groups III and IV (n=16 each) included diabetic and nondiabetic patients, respectively, living at normobaric condition (300 m). Group III patients were randomly selected from outpatients monitored for diabetes enrolled at El-Magarda General Hospital. As diabetic patients (groups I and III) were selected from 2 hospitals belonging to the same governorate (Assir Department for Health Management), the same protocol of diabetes monitoring and laboratory techniques were applied. Also, diabetics were selected according to the history of the disease and the level of fasting blood glucose (>130 mg/dL), only patients diagnosed with DM between 5–10 years ago were included. Patients treated with insulin and those with extremely high fasting glucose level, which may predispose diabetic complications, were excluded. All patients were native Saudis, not practicing exercises and not suffering from kidney, heart, or chest complications; samples were taken under informed consent following applied ethical regulations.
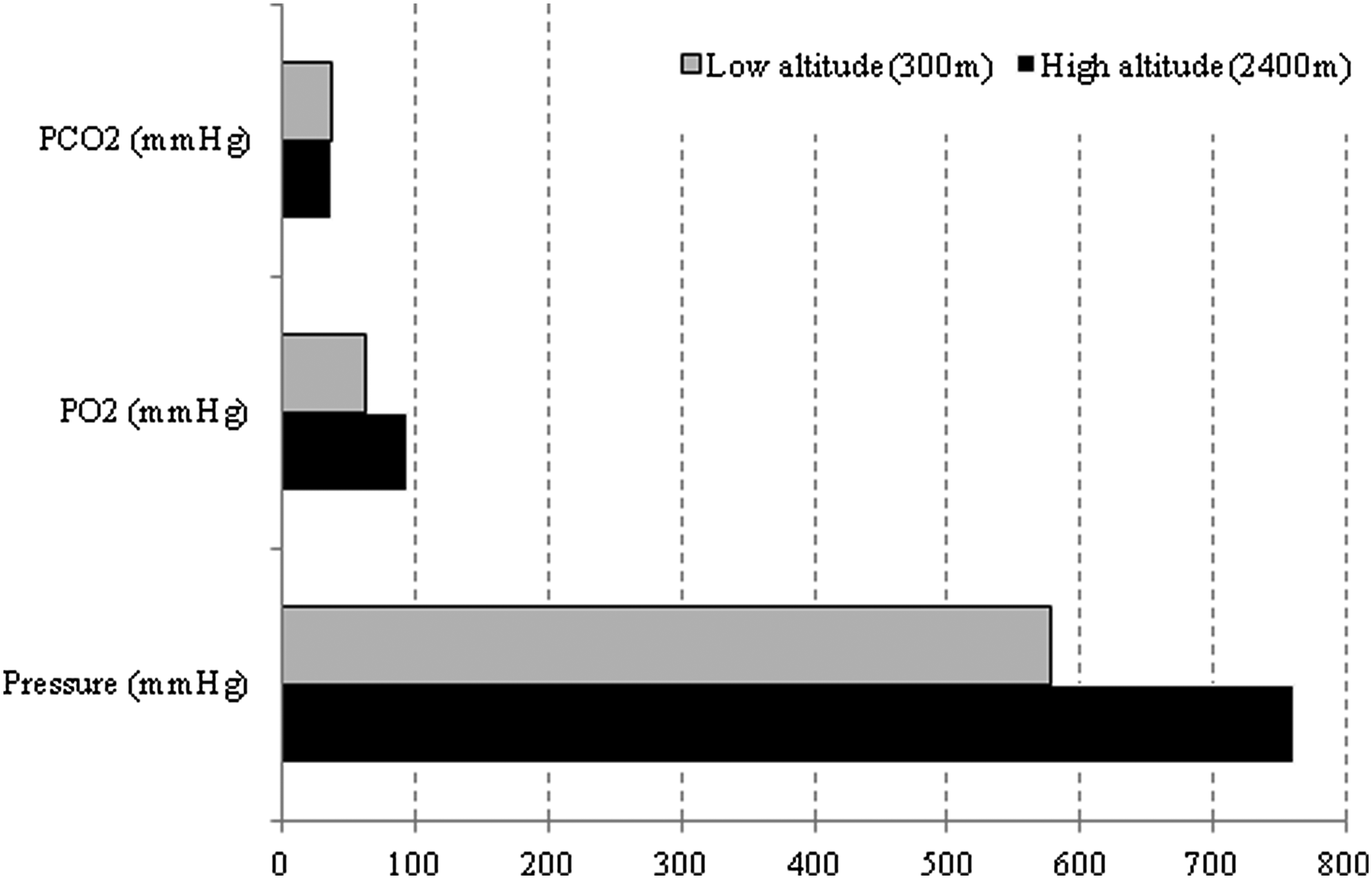
Barometric pressure and oxygen and carbon dioxide tensions at low (300 m) and high (2400 m) altitudes.
DM, diabetes mellitus; LA, low altitude.
Biochemical and hematologic investigations
Glycohemoglobin (HbA1c) was determined by fast ion exchange resin separation method, using a Human diagnostic kit (Human Diagnostics, Germany). According to this method, red blood cells were lysed with lysing reagent (I mol/L borate and 0.025% detergent). The hemolysate was mixed with ion exchange resin, where HbA0 binds to the resin. A special resin separator was used to remove the resin from the supernatant, which contains HbA1. HbA1 percentage of total hemoglobin was determined by measuring its absorbance and the absorbance of total hemoglobin fractions for both sample and standard hemoglobin at 415 nm. Patients with poor glycemic control were defined as those with HbA1c values above 8.5 percent. Blood glucose was estimated in fasting blood samples by enzymatic colorimetric test using “Glucose liquicolor” kit (Human Diagnostics) following the manufacturer instructions. Hematologic parameters, hemoglobin concentration, and hematocrit (HCT) were estimated using blood cell counter (Humacount Plus, Human Diagnostics).
Arterial blood gases
Blood samples for arterial blood gas analysis were obtained under informed consent, using heparin as an anticoagulant, from patients with type II diabetes and healthy subjects. Samples were immediately used to determine: oxygen tension (Pa
Statistical analysis
Data were expressed as mean±standard deviation. Comparison between means was analyzed by ANOVA test. P values less than 0.05 were considered significant. The correlations between different variables were performed by Person or Spearman correlation test. Statistical analysis was performed by Graphpad Instat software (Graphpad, San Diego, CA).
Results
Fasting blood glucose levels in groups I, II, III, and IV were: 157.33±12.3, 84.0±6.2, 176.81±15.90, and 89±6.55 mg/dl, respectively. As expected, glucose concentrations in groups I and III (ranged 125–182 mg/dL and 158–213 mg/dL, respectively) were significantly higher than the corresponding nondiabetic patients living at the same altitude (group I vs. group II: p<0.001; group III vs. group IV: p<0.001) (Table 2). Also, the glucose concentration of diabetic patients in groups I (HA diabetics) was significantly lower than diabetic patients living at low altitude (group I vs. group III, p<0.001), where moderate altitude diabetic patients have 11% less glucose compared to low altitude diabetics.
Significant difference between the indicated group and the corresponding low altitude group.
Significant difference between the indicated group and the corresponding nondiabetic group at the same altitude.
Assessment of glycemic control revealed that diabetic patients in groups I and III had mean HbA1c of 8.68% (±0.79) and 9.3% (±1.02) and ranges 6.7%–9.8% and 7.9%–11%, respectively, whereas HbA1c was higher in diabetic patients compared to healthy subjects in both groups II and IV (p<0.001, p<0.001). Altitude diabetics (group I) showed slightly but significantly lower (P<0.05) HbA1c than diabetic patients at low altitude (group III) (Table 2).
Significant increase in both hemoglobin concentration and HCT was observed in groups I and II compared to groups III and IV (Table 2). Also, no differences in hemoglobin and HCT were observed between diabetics and nondiabetics living in the same altitude (group I vs. group II, p>0.05; group III vs. group IV, p>0.05).
Partial pressure of arterial oxygen (Pa
Significant difference between the indicated group and the corresponding low altitude group.
Significant difference between the indicated group and the corresponding nondiabetic group at the same altitude.
Discussion
Altitude illnesses usually occur at altitude over 1500 m and are caused primarily by hypoxia. Chronic high altitude-induced hypoxia may lead to retinal disorders, which are well known long-term complications of diabetes mellitus. Type II diabetics were randomly assigned from native nonathletic Saudis, permanently living at moderate altitude. Chronic exposure to hypoxic condition affected the glucose level and glycemic control in diabetic patients (group I). Glucose level of diabetics living at moderate altitude was lower than those living at low altitude (mean: 157.33±12.30 and 176.81±15.88 mg/dL, respectively; p<0.001), where the mean glucose level of altitude diabetic patients was 11.1% lower than diabetic patients living at low altitude (p<0.001). Chronic hypoxia may increase insulin sensitivity and insulin-stimulated glucose uptake (Gamboa et al., 2011). This may explain the reduction of glucose in group I.
Long-standing hyperglycemia leads to the formation of glycohemoglobin, which is formed when glucose, nonenzymaticaly and irreversibly, interacts with the amino groups of valine and lysine of the hemoglobin. (Bry et al., 2001). As the level of HbA1c in the red blood cell depends on the blood circulating glucose concentration, measuring HbA1c provides a measurement of long-term glycemic control in diabetic patients (Yue et al., 1993). Diabetics permanently living at moderate altitude (group I) showed a better glycemic control, where their HbA1c was lower than the corresponding diabetic patients living at normoxic and normobaric conditions (group III). This is supported by some reports that indicated that high altitude could produce a beneficial effect on glucose tolerance, and high altitude possibly is a potential natural medicine for treatment of type II diabetes (Bry et al., 2001). Also, chronic hypoxia has increased insulin-stimulated glucose uptake in mouse soleus muscle (Gamboa et al., 2011) and improved insulin action in mountain climbers on a prolonged altitude expedition (Chen et al., 2010). In contrast, short-term exposure to altitude and the altitude level (moderate, high, or extremely high) change glucose homeostasis. Exercise at short-term exposure to high altitude, for instance, induces impairment in glycemic control in type 1 diabetics (Brubaker, 2005). Very high altitude (5000 m) largely affects the glycemic control in both type I and II, where it increased insulin requirements during exercise in type 1 diabetes (deMol et al., 2011).
Permanent living in hypoxic conditions is physiologically compensated by a marked increase in hemoglobin and HCT. Groups I and II had 11.8% and 10.4% higher hemoglobin concentrations compared to the corresponding groups living at normoxic condition, and a similar changing pattern was observed in HCT percent by Palmer (2011).
Arterial oxygen pressure (Pa
Factors decreasing hemoglobin–oxygen affinity shift the oxygen dissociation curve to the right. High altitude-related increase in glucose uptake and the increased insulin sensitivity will increase the level of cellular glycolytic intermediate 2,3-diphosphoglycerate (2,3-DPG). When it binds to hemoglobin, 2,3-DPG causes a molecular configuration in hemoglobin that lower its affinity with oxygen, subsequently improving tissue oxygenation (Farber et al., 1991).
In conclusion, the study supports the notion that moderate (not extreme) altitude living may improve glycemic control in type II diabetic patients compared to diabetics living at low altitude. The study is limited to native Saudis, nonathletic, permanently living at moderate altitude. More studies are needed to confirm these findings.
Footnotes
Acknowledgments
The author would like to thank medical staff members of the medical laboratory department of El Namas General Hospital for providing samples and arterial blood gas analysis in this study.
Author Disclosure Statement
The data presented in this study is not influenced by author's personal or financial relationship with other people or organizations. Also, he declares that he has no competing interests.