
Abstract
Abstract
Yangzong, Sveinung Berntsen, Espen Bjertness, Hein Stigum, Gonggalanzi, Bianba, and Per Nafstad. Lung function among 9- to 10-year-old Tibetan and Han Chinese schoolchildren living at different altitudes in Tibet. High Alt Med Biol 14:31–36, 2013.—Tibetans have lived at high altitude longer than any other high-altitude population. Still little is known about their lung function and especially among children. This study compared lung function values of forced vital capacity (FVC), forced expiratory volume in one second (FEV1), and forced expiratory flow at 50% of FVC (FEF50) in children living at various altitudes in Tibet and with different ancestries. A cross-sectional study of lung function was performed among 9–10-year-old native Tibetan and Han Chinese children living at 3700 meters above sea level, and among native Tibetan children living at 4300 meters above sea level. The adjusted FVC and FEV1 were significantly higher in Tibetan children living at 4300 m above sea level as compared to Tibetans living at 3700 m. Tibetans living at 3700 m had higher FVC and FEV1 than Han Chinese living at the same altitude. All Tibetan children had on average higher FEF50 than Han Chinese. Tibetan children living at an altitude of 4300 m had relatively higher lung function than those living at 3700 m, and there were differences in lung function between Tibetans and Han Chinese who live at the same altitude. It seems likely that genetic factors involved in long-term adaptation to high altitude and cultural attributes could have contributed to the study findings.
Introduction
In the present study we have measured lung function in children of Tibetan and Han Chinese origin living in Lhasa (3700 meters above sea level) and children of Tibetan origin living in Tingri (4300 meters above sea level). The present study aims to describe and compare maximum forced expiratory flow values including FVC, FEV1 and forced expiratory flow at 50% (FEF50) in three different child populations in the Tibet Autonomous Region (TAR), People Republic of China, and explores how conditions like ancestry, altitude of residence, anthropometric measurements, and asthma symptoms influence lung function. We hypothesized that, as part of their long-term adaptation to high altitude, the Tibetans have higher lung function than Han Chinese, and Tibetans living at 4300 meters of altitude have higher lung function in comparison to Tibetans living at 3700 meters of altitude.
Materials and Methods
Study areas
The data for the present study were collected in Lhasa City and Tingri County. Lhasa, the administrative capital of the TAR, is situated at an elevation of about 3700 m above sea level with a population of 400,000, of which around 87% are Tibetans and 13% are of Han and Hui Chinese origin (Lhasa Government, 2011). Tingri is situated in the south of the Shigatse Prefecture close to the border to Nepal. The average altitude is 4300 m above sea level and the county has a population of approximately 50,000, which is largely made up of Tibetans (Tibet Government, 2011).
Study samples
The study population included three groups: Lhasa Tibetan, Lhasa Han Chinese and Tingri Tibetan children.
Lhasa children
Nine out of a total of 20 primary schools in Lhasa City were randomly selected. All children aged 9–10 years were invited to participate in the study. Of the 817 eligible children, 1 child refused and 4 were unable to participate, giving a participation rate of 99%. For unknown reasons, 9 children did not attend the lung function measurement, and 3 children did not attend the anthropometric measures. Furthermore, after a quality check of all flow-volume curves, the curves from 9 of the children were found to be of insufficient quality according to the acceptability criteria of flow-volume curves (Quanjer et al., 1993; Miller et al., 2005). Thus, data from 396 Tibetans (204 boys/192 girls) and 395 Han Chinese (233 boys/162 girls) were included in the analysis. Data collection took place between August and November 2005 and was carried out indoors in separate rooms sheltered from any disturbing elements.
Tingri children
Five out of 14 primary schools located at high altitude were selected. All Tibetan children aged 9–10 years were considered eligible (N=460). A total of 16 children did not attend the school during the days of data collection, giving a participation rate of 97%. For 14 children participating in the survey, their parents decided not to give permission to use their data for research. For unknown reasons, 63 children did not show up for anthropometric measures (n=26), lung function test (n=31), or both (n=6). Furthermore, due to insufficient quality of the flow-volume curves, 6 children's lung function data had to be excluded according to the acceptability criteria of flow-volume curves (Quanjer et al., 1993; Miller et al., 2005). Thus, data from 361 children (181 boys/180 girls) were included in the analysis. Data in Tingri were collected from the end of September to the beginning of December 2007, and according to the same protocol as in Lhasa.
Lung function measurement
FVC, FEV1, and FEF50 values were measured by maximum forced expiratory flow-volume curves (Micro Medical Limited, Rochester, Kent, UK) according to the criteria of the European Respiratory Society and American Thoracic Society (Miller et al., 2005; Wanger et al., 2005). Tests were explained orally and shown visually to the children until they indicated that they understood the procedure and showed that they could perform acceptable maximum forced expiratory flow-volume maneuvres. Lung function was measured while children were seated in an upright position; children wore nose clips during the test. A valid test has to include at least three acceptable manoeuvres. Therefore the test was repeated three to eight times in order to achieve a valid test for all the children. The technicians who were performing the lung function test in Lhasa and Tingri had been trained and guided by the same person. All children's flow-volume curves were reviewed for technical acceptability and the highest value was included in the analysis. Lung function values were presented at body temperature (37°C), pressure, and saturated with water vapor (BTPS).
Covariates
The questionnaire was completed by children under the supervision of field workers. The questionnaire included items of asthma and asthma-related symptoms based on the International Study of Asthma and Allergies in Childhood (ISAAC). It included written and “video” questions about asthma symptoms, as well as questions about environmental exposure such as parental smoking (ISAAC, 1993). The videos were used to give an audiovisual presentation of asthma symptoms (ISAAC, 2011). It showed five video sequences of people who had different manifestations of asthma (wheeze at rest, wheeze after exercise, night waking with wheeze, night waking with cough, and severe asthma attack). For each sequence, the children were asked to fill in whether they had experienced the symptoms. The questionnaire for the present study was translated from English to Tibetan and Chinese, and back to English.
Height and sitting height was measured without shoes (nearest 0.5 cm), using a stadiometer (TZG, Shanghai, China). Weight was measured without shoes and outer clothing (nearest 0.1 kg), using an electronic scale (OMRON, HN-281, Shanghai, China). Chest circumference was measured without outer clothing and sweater at a point crossing both nipples (nearest 0.1 cm), with children standing. Body Mass Index (BMI) was calculated as body weight (kg) divided by height (m) squared. Age was estimated from information on the year of birth for all children.
Ethics
Research clearance and approval was obtained from the Ministry of Health and the Ministry of Education in the TAR. Informed written consent was given by parents. Participations were informed that they could refuse to participate and withdraw from the study at any time without any consequences.
Statistical analysis
Analysis was carried out in SPSS (Statistical Package for Social Sciences, Version 15 for Windows. SPSS Inc. Chicago, USA, 2006). The study was performed to identify difference in lung function between three groups (Lhasa Tibetan, Lhasa Han Chinese, and Tingri Tibetan). Means and 95% confidence interval (CI) were used to describe characteristics of anthropometric measures and lung function outcomes, stratified on gender and population groups. We used P–P plots and the Kolmogorov-Smirnov test to inspect and test for normality distribution, and we found no deviation from normality.
To model the relations between the covariates and lung function values (FVC, FEV1, and FEF50) by ancestry and altitude of residence, the analysis took into account factors that may influence lung function; for example, we adjusted for gender, height, sitting height, weight, BMI, chest circumference, and night waking with cough. Asthma symptoms and other covariates were only included in the models when they were statistically significantly associated with the outcomes. One-Way Anova and Univariate analyses were performed for the outcomes (FVC, FEV1, and FEF50) before and after adjusting for variables mentioned above. The Tukey post-hoc test was used for comparisons in lung function values between three study groups. Level of statistical significance was set to p<0.05.
Results
Table 1 shows anthropometric measurements and unadjusted lung function values in Lhasa Tibetans, Lhasa Han Chinese, and Tingri Tibetans. The height, sitting height, weight, BMI, and chest circumference were higher among Lhasa Tibetans than Han Chinese. Both groups in Lhasa had higher anthropometric measurements than Tingri Tibetans. For the unadjusted lung function of FVC, FEV1, and FEF50, Lhasa Tibetans scored higher than Lhasa Han Chinese. Both groups in Lhasa had higher unadjusted lung function values than Tingri Tibetans in both boys and girls.
BMI, body mass index; CI, confidence interval; FEF50, forced expiratory flow at 50% of FVC; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity.
Figure 1 shows the differences between three study groups with regard to FVC, FEV1, and FEF50 values before and after adjusting for gender, height, sitting height, weight, BMI, chest circumference, and night waking with cough. Night waking with cough was the only asthma symptom that was statistically significantly related to the outcomes and was therefore included in the multivariable models. “Night waking with cough” was reported by 2.6% of the Tingri Tibetans, 6.5% of the Lhasa Tibetans, and 7.2% of the Lhasa Chinese. Before adjustment, Lhasa Tibetans had higher FVC, FEV1, and FEF50 than Lhasa Han Chinese, and Lhasa Han Chinese had higher values than Tingri Tibetans. The difference between the three study populations was statistically significant for FVC and FEV1, but not for FEF50 between Lhasa Han Chinese and Tingri Tibetans. After adjustment, Tingri Tibetans had higher FVC and FEV1 than Lhasa Tibetans, and Lhasa Tibetans had higher values than Lhasa Han Chinese. Lhasa Tibetans still had higher FEF50 than the two other groups, and Tingri Tibetans had higher FEF50 than Lhasa Han Chinese. All comparisons were statistically significant, except for the comparison of FEF50 between Lhasa Tibetans and Tingri Tibetans.
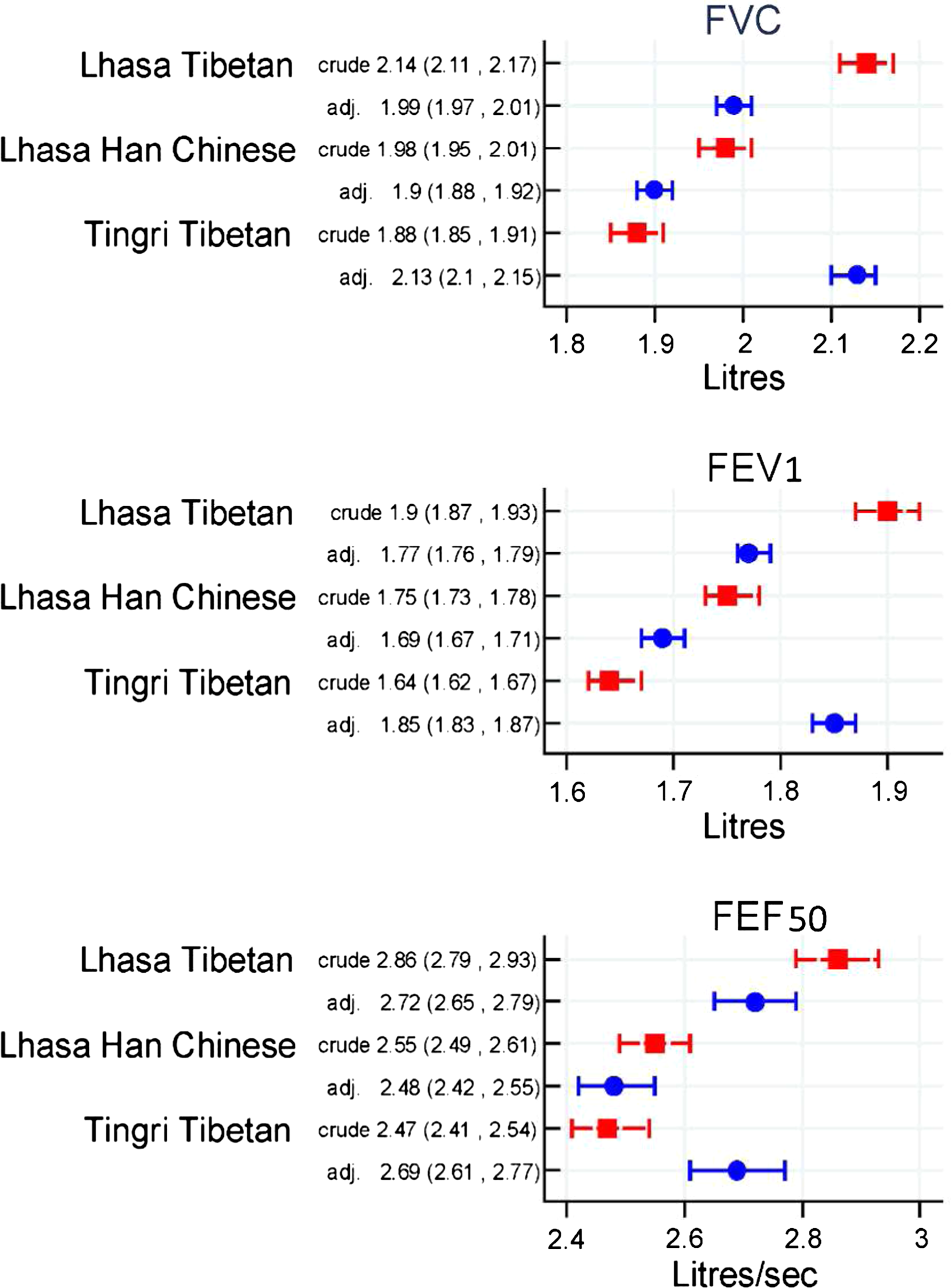
Differences of FVC, FEV1, and FEV50 in the study groups.
Among 395 Han Chinese children, we grouped the duration by year of living in Lhasa for Han Chinese in: <9 years (migrant) and 9–10 years (nonmigrant); there were 74% migrant children and 26% nonmigrant children. Moreover, 56% Han Chinese children reported to have lived more than half of their life in Lhasa. Using One-Way Anova we did not find any difference in FVC, FEV1, and FEF50 between migrant and nonmigrant children or between children that had lived more than half of their life in Lhasa or not.
Discussion
Comparisons of crude lung function parameters could indicate that Tibetan children living at 3700 m had the highest lung function values and that Han Chinese children had higher values than Tingri Tibetans living at 4300 m of altitude. However, after adjustment for gender, anthropometric measures as earlier described and night waking with cough, Tingri Tibetans, the children with the highest altitude of residence, turned out to have statistically significantly higher FVC and FEV1 than Lhasa Tibetans, and that Lhasa Tibetans had higher values than Lhasa Han Chinese.
Altitude of residence has been shown to be related to lung function in several studies (Woolcock et al., 1972; Sun et al., 1990; Droma et al., 1991; Villena et al., 1994; Brutsaert et al., 1999; Chen et al., 1997; Havryk et al., 2002; Weitz et al., 2002;). To our knowledge, no other study has reported lung function measures in Tibetan and Han children living in Tibet, nor compared lung function values in Tibetan children with different altitude of residence. It is likely that the altitude at which people live affects their lung function. We speculate that this is an adaptation in response to hypobaric hypoxia and that it is likely that highlanders who are exposed to hypoxia or low ambient pressure from birth, respond by developing larger sized lungs that facilitates oxygen diffusion capacity (Cerny et al., 1973; Niermeyer et al., 1995; Curran et al., 1997; Wagner et al., 2002; Brutsaert et al., 2004; Hlodan, 2010). Our finding is in agreement with this. Furthermore, there has lately been a substantial immigration of Han Chinese to Tibet. Therefore, we tried to investigate if the duration of having lived at high altitude influences lung function. However, our data could not confirm this. The main reasons for this could be an insufficient sample size of Han Chinese children to address effects of the duration of living at high altitude (Lhasa) properly. Furthermore, we lacked adequate data on duration and age of exposure to high altitude for the Han Chinese children.
Besides addressing altitude of residence, we also wanted to look for potential differences in lung function by ancestry group, having taken altitude of residence into account by comparing lung function levels in Tibetan and Han Chinese living at the same altitude. Our findings showed that lung function in these two ancestry groups living at the same altitude was different. This indicates that there is an effect of ancestry (Brutsaert, 2007; Lum and Aurora, 2010). Findings from the United States support such a view as it has been reported that White children have higher FVC and FEV1 values than African-Americans (Harik-Khan et al., 2004), and that Asian-Americans have lower lung function values than European-Americans (Brutsaert et al., 2004; Lum and Aurora, 2010). As in most studies, our study also can not fully address if all the observed differences are related to genes. The differences between Tibetans and Chinese are likely to be partly genetic. However, we were reluctant to claim that it is only genes or only altitude that separate the groups, as other living conditions and culture could potentially contribute to the differences we observed. We have therefore chosen to use the expression ancestry. It is possible that living at high altitude for generations could level out the recorded lung function differences between Tibetans and Han Chinese. If so, adaptation to the high altitude could be an explanation.
It is well known that lung function values depend on anthropometric measures and should be adjusted for when comparing lung function values between individuals and populations (Lazarus et al., 1997; Krause et al., 2005). Crude lung function and anthropometric measures were differently distributed in the three populations and adjustments for anthropometric factors had dramatic effects on the comparisons of lung function between the three child populations in the present study. Anthropometric measures were quite different in the three study populations. The differences could be due to difference in altitude of residence as previous studies have reported associations between altitude of residence and childhood growth (Yip et al., 1988; Niermeyer et al., 1995; Moore et al., 2001; Dang et al., 2008). These issues point towards the necessity to address overall growth in these children.
There are some limitations in the present study that deserve further consideration. The investigators who measured lung function were different in Lhasa and Tingri. To reduce the chance of investigator bias, the investigators were trained by the same person and the same equipment was used for all tests. Furthermore, the one and same person went through and assessed all the lung function curves according to the standardized and international acceptability criteria. There were 63 Tibetan children from Tingri who were not included in the final analysis because of missing information for one or more anthropometric or lung function measures. However, the available results from anthropometric and lung function measures among these children did not indicate that these children were different from those included in the analysis. Studies have indicated that there are life style factors that could affect lung function such as nutritional status socio-economic status, and environmental exposures to air pollution. However, we lacked precise information about several such exposures, which makes it difficult to address these issues further in the present study.
Conclusion
To our knowledge, this is the first population based study of lung function among children aged 9–10 years living in Tibet. Our findings indicated that Tibetan children living at an altitude of 4300 m had relatively higher lung function values than those living at 3700 m. Furthermore, we found differences in lung function between children of different ancestry groups, despite living at the same altitude. It seems likely that genetic factors involved in long-term adaptation to high altitude as well as cultural attributes could have contributed to the study findings. However, the cross-sectional study design, and potential other unmeasured differences between the study populations, warrant careful conclusions. The observations should be confirmed in future research with more optimal study design and data.
Footnotes
Acknowledgments
We thank the children and parents who participated in this survey and the school staff for their help. This study was supported by the Network for University Cooperation Tibet-Norway and Tibet University Medical College.
Author Disclosure Statement
All authors declared no financial conflicts.