Insalaco, Giuseppe, Salvatore Romano, Adriana Salvaggio, Luca Pomidori, Gaia Mandolesi, and Annalisa Cogo. Periodic breathing, arterial oxyhemoglobin saturation, and heart rate during sleep at high altitude. 13:258–262, 2012.—The aim of this study was to investigate the effects of acclimatization to high altitude on periodic breathing (PB), arterial oxygen saturation (Sao2), and heart rate (HR). Nine male elite climbers, age 24–52 years underwent overnight cardiorespiratory monitoring at sea level and at Everest North Base Camp (5180 m), during the first (BC1) and the tenth (BC2) nights. PB was commonplace in all subjects at high altitude. PB cycle duration increased (p<0.0001) from BC1 (21.7±1.9 s) to BC2 (26.7±2.1 s). Mean Sao2 from BC1 to BC2, significantly increased during wakefulness (77.4±3.4% vs. 82.5±2.8%; p<0.001) and during sleep regular breathing (73.3±3.8% vs. 77.8±2.9%; p=0.022). During PB, mean higher Sao2 was 75.3±3.6% at BC1 and 82.4±2.9% at BC2 (p<0.001); mean lower Sao2 was 68.2±4.0% at BC1 and 74.5±4.3% at BC2 (p<0.01). During PB, mean higher HR was 72.4±8.8 b/min at BC1 and 63.3±6.0 b/min at BC2 (p<0.0002); mean lower HR were 53.6±7.5% at BC1 and 43.6±7.3% at BC2 (p<0.0001). The mean Sao2 during PB compared with Sao2 at night without PB was unchanged. Acclimatization to high altitude resulted in an overall increase in Sao2 along with an increase in the PB cycle duration and a decrease in HR.
Introduction
High-altitude environments are characterized by a low partial pressure of oxygen due to the progressive decrease in barometric pressure. Soon after ascent to altitude, the resulting hypoxia generates physiological changes that counteract the negative effects resulting from the decreased oxygen availability and limit the decrease in arterial oxygen content (West et al., 2007). These changes include increased ventilatory responsiveness to chemical stimuli, hyperventilation, and increased plasma bicarbonate urinary excretion (Crawford et al., 1978; White et al., 1987; Sato et al., 1994; Insalaco et al., 1996). As a result, hypocapnia appears and arterial hypoxemia is attenuated. Despite the acclimatization process, healthy subjects ascending to high altitude experience dyspnea and tachycardia after moderate efforts and complain of a poor quality of sleep (Reite et al., 1975; Sutton, 1982; Salvaggio et al., 1998; Johnson et al., 2010) which is characterized by the presence of periodic breathing (PB). Hypocapnic hypoxia seems to be the main determinant of the appearance of PB during sleep in the subjects acutely exposed to high altitude (Berssenbrugge et al., 1983; Weil, 2004; Bloch et al., 2010). System stability is decreased by hypoxia, increased lung washout times, prolonged lung-chemoreceptor delays, and high controller sensitivity (Khoo et al., 2000).
The alterations in sleep breathing pattern have been described in healthy subjects at high altitude up until a 1-month stay (Lahiri, 1972; West et al., 1986; Salvaggio et al. 1998; Insalaco et al., 2000; Nussbaumer-Ochsner Y, 2012). Sleep studies showed that the major phenomenon occurring at high altitude, in relation to the state of hypocapnic hypoxia, was PB during nonrapid eye movement (NREM) sleep (Salvaggio et al., 1998; Johnson et al., 2010). An increase in PB has been reported during a stay at 5050 m (Salvaggio et al., 1998). In this condition, owing to the highly hypoxic environment, arterial oxygen saturation (Sao2) is low and decreases further during sleep (Anholm et al., 1992; Salvaggio et al., 1998; Bloch et al., 2010). Conversely, other studies performed in a small number of subjects have provided conflicting results on the trends of breathing pattern changes during moderate to high-altitude acclimatization, reporting reduction (White et al., 1987) or no change in periodic breathing (Zielinski et al., 2000). It has been proposed that PB, despite determining large swings in Sao2, could sustain Sao2 at an average level higher than that resulting from stable breathing (Salvaggio et al., 1998). However, the effect of PB on mean overnight Sao2 during sleep is still unclear.
Few data are available on heart rate (HR) during sleep-induced PB in normal subjects at high altitude; HR was found to decrease during the respiratory pause of PB cycles proportionally to the Sao2 fall and to fluctuate during the PB cycles with the lowest values found during apnea and the highest during hyperpnea. (Masuyama et al., 1990; Insalaco et al., 2000).
The purposes of this study were to investigate PB at high altitude and its effect on Sao2 and HR both at the beginning of the acclimatization process and after 10 days.
Methods
Nine male elite climbers, aged between 24 and 52 years (mean 37±8), body mass index 23±9 kg/m2, and with normal respiratory function test (FVC 110±5%; FEV1 104±8% of predicted values; FEV1/FVC 0.89±0.04) have been studied with overnight cardiorespiratory monitoring at sea level and at Everest North Base Camp (5180 m), during the first (BC1) and the tenth (BC2) night. Baseline evaluation was performed in Ferrara (9 m) within 4 weeks before departure. The altitude of 5180 m was reached by jeep after a 4-day journey from Lhasa (3600 m) which had been reached by plane. Between the two measurements, all subjects climbed up to 7000 m and spent ≥2 nights at 6100 m with no use of oxygen and no symptoms of acute mountain sickness. No subject was allowed to consume medication known to modify the control of breathing, such as acetazolamide, theophylline, or benzodiazepines. The protocols were reviewed by the institutional review committee and informed consent was obtained.
Nocturnal monitoring was performed by the LifeShirt system (LifeShirt; VivoMetrics, Ventura, CA), an ambulatory multi-sensor, continuous monitoring system that we used to collect physiologic data throughout the night study via various sensors, including respiratory inductive plethysmography bands, body position, electrical activity of the myocardium via a 1-lead electrocardiogram, arterial oxygen saturation (Sao2) by pulse oximetry, and snoring by a microphone on the sternal notch. The sensor array of the LifeShirt System is embedded in a sleeveless undergarment. Signals were continuously recorded on a compact flash memory card inserted in the LifeShirt monitor before each overnight recording. Data cards were downloaded into a computer at the end of the recording period. The LifeShirt monitor was powered by batteries allowing up to 24 hours of continuous recordings. Batteries were recharged during daytime by generators available at base camp. VivoLogic, a proprietary personal computer-based software, was used for viewing and reporting features. Timestamps identifying the nocturnal rest period were recorded in the LifeShirt monitor. Respiratory signals were subsequently analyzed to identify PB cycles using software developed in our laboratory written in MATLAB R2008B (The MathWorks; Natick, MA). PB was defined as a cyclic increase in the amplitude of thoraco-abdominal movements, followed by respiratory pauses (absence of respiration lasting at least 4 s), or transient reduction in breathing amplitude (reduction in the thoraco-abdominal movements ≥50% of the maximum amplitude during the preceding hyperpneic phase of the PB cycle). Ribcage, abdomen, and sum signals were visually analyzed to distinguish epochs with and without PB. As regard respiration without PB, mean respiratory rate and mean Sao2 were calculated. Subsequent analysis of HR and Sao2 related to PB was performed. In each PB cycle, we measured highest and lowest Sao2 and HR. A mean of all Sao2 and HR values of all PB cycles was performed in each subject.
Statistical analysis
The results between BC1 and BC2 were compared using the Mann-Whitney test. Data are reported as mean±SD. A p<0.05 was considered significant. Statistical analysis was performed by commercial software (JMP 8.0 SAS Institute Inc.).
Results
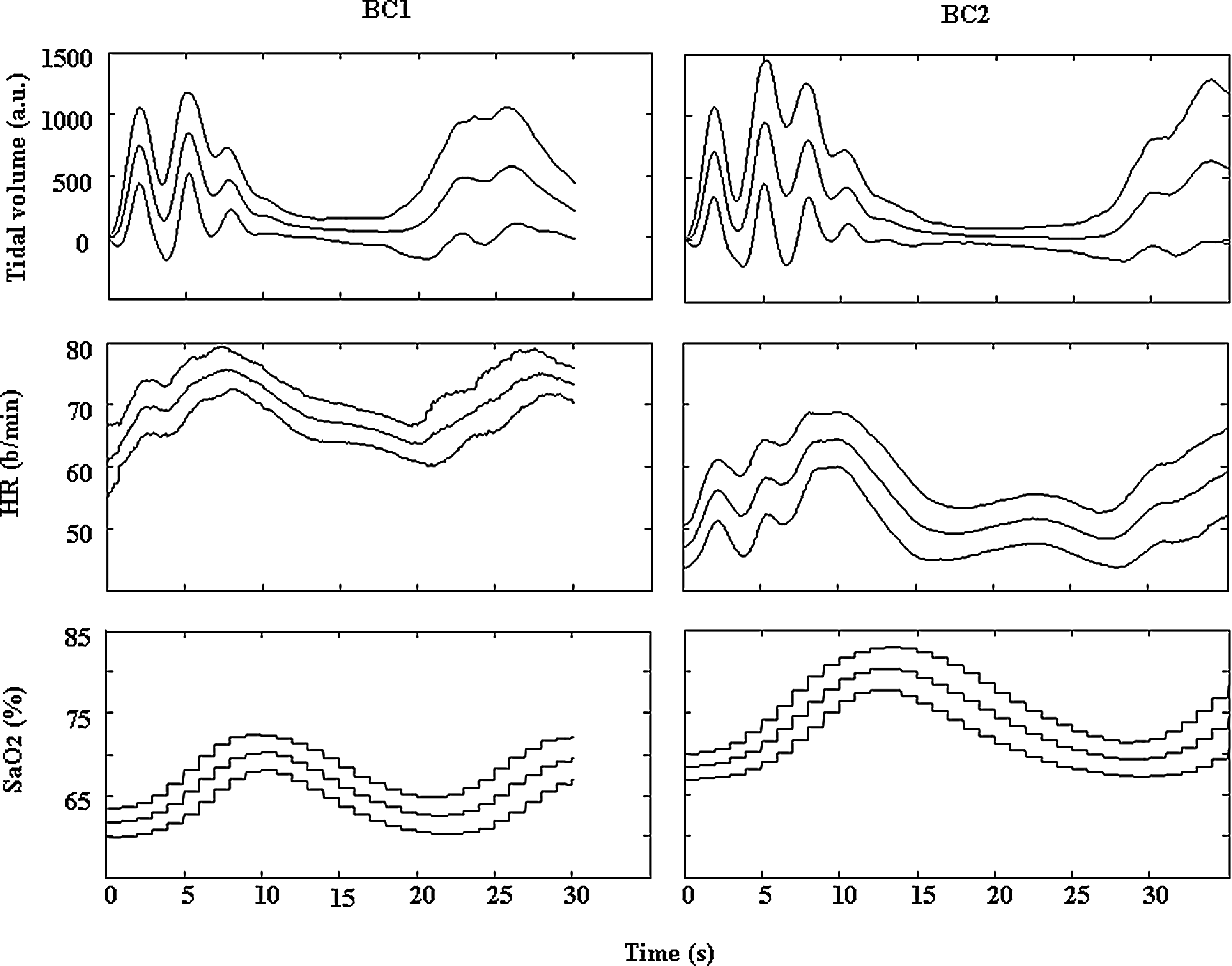
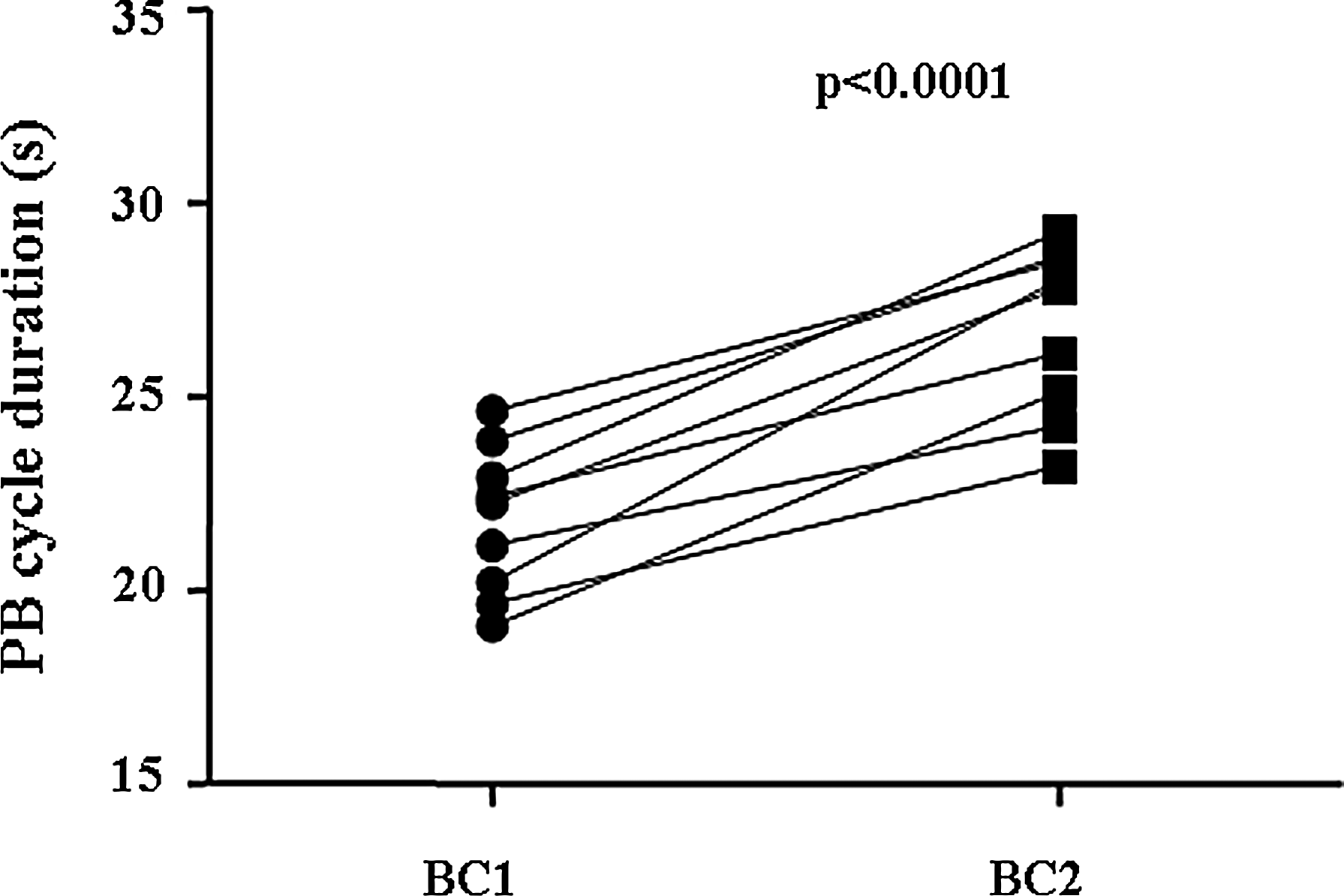
At sea level, no respiratory disturbances were observed, mean and lower Sao2 of all subjects during sleep were 96.3±0.6% and 93.3±0.8%, respectively. PB was commonplace in all subjects at Everest North Base Camp. A representation of PB and associated variables is reported in Figure 1. In all high-altitude studies, both regular breathing and PB were observed to a variable extent among subjects. In 7 out of the 9 subjects, an increase of percent time in bed with PB was found from BC1 to BC2. In all subjects, range of percent of time in bed with PB was 6.0%–64.5% at BC1 and 29.3%–78.5% at BC2 (NS). PB cycle duration in all subjects significantly increased from BC1 (21.7±1.9 s) to BC2 (26.7±2.1 s) (p<0.0001) (Fig. 2). Mean Sao2 from the BC1 to the BC2 significantly increased during wakefulness (77.4±3.4% vs. 82.5±2.8%; p<0.001). During sleep regular breathing, the mean Sao2 of all subjects was 73.3±3.8% at BC1 and 77.8±2.9% at BC2 (p=0.022), and the mean respiratory rate was 18.0±3.2 breaths/min at BC1 and 16.7±2.4 breaths/min at BC2 (NS).
Mean±SD of tidal volume, heart rate, and arterial oxygen saturation during periodic breathing in one subject at Everest North Base Camp (5180 m), at the 1st (BC1), and the 10th (BC2) night.
Mean periodic breathing cycle duration at Everest North Base Camp (5180 m), at the 1st (BC1) and the 10th (BC2) night for all subjects.
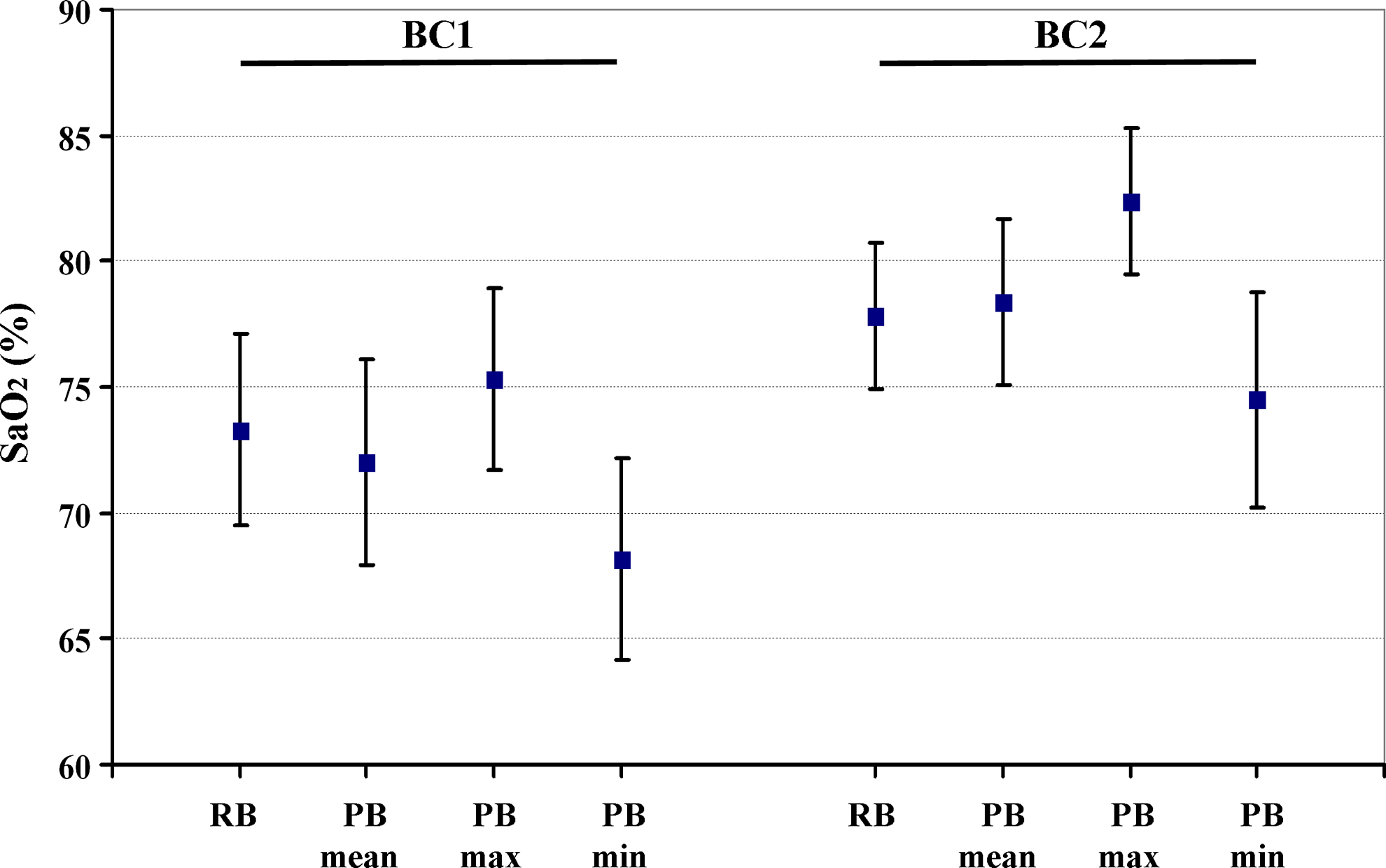
During PB, the mean higher Sao2 levels of all subjects was 75.3±3.6% at BC1 and 82.4±2.9% at BC2 (p<0.001), and the mean lower Sao2 levels with PB of all subjects was 68.2±4.0% at BC1 and 74.5±4.3% at BC2 (p<0.01) (Fig. 3). However, changes in amplitude of Sao2 swing during PB at BC1 (7.1±2.2%) and at BC2 (7.8±2.7%) were not statistically different.
All subjects mean±SD values of arterial oxygen saturation (Sao2) during sleep regular breathing, lowest Sao2, highest Sao2, and the average of the low and high Sao2 during sleep periodic breathing (PB), at Everest North Base Camp (5180 m), at the 1st (BC1) and the 10th (BC2) night.
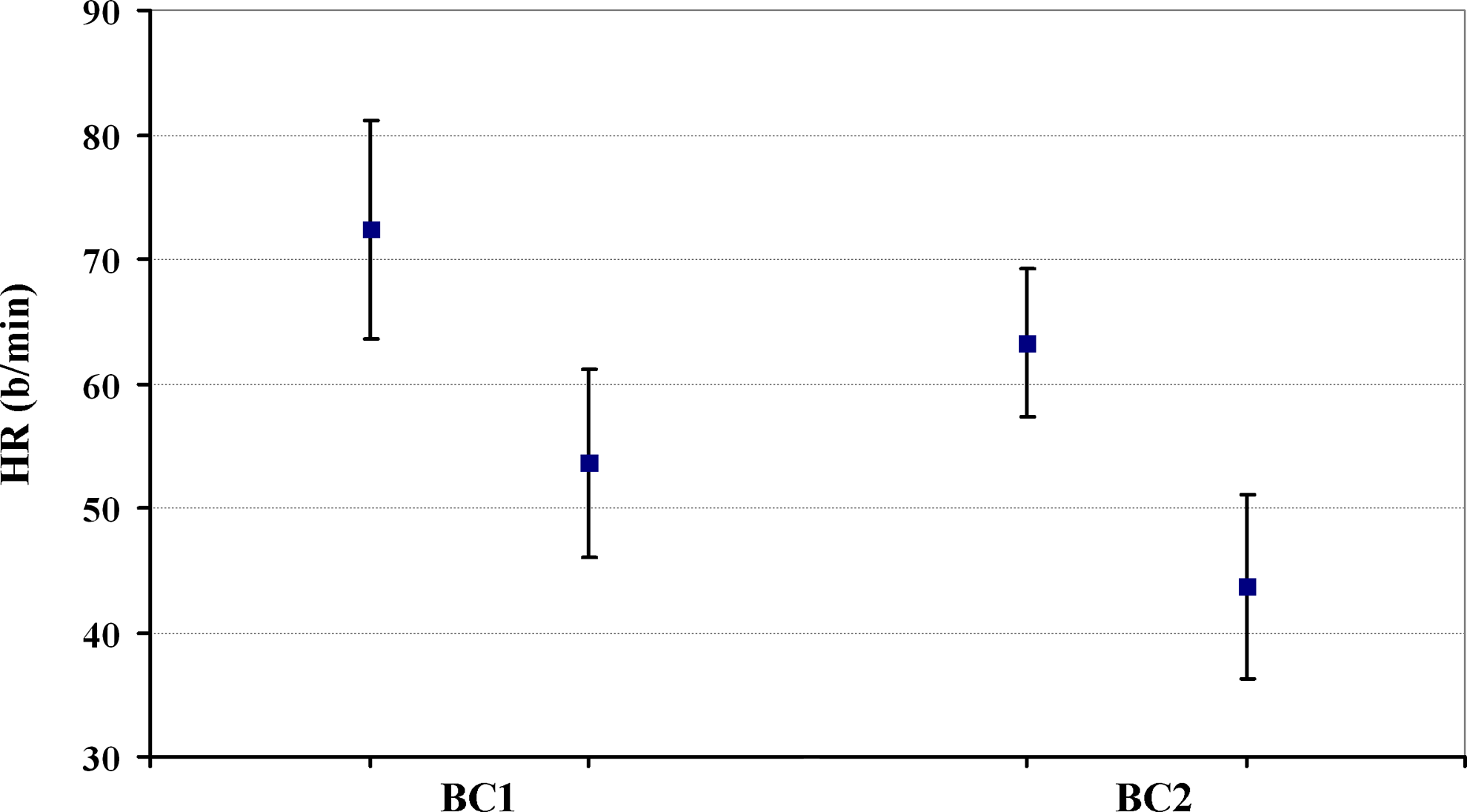
HR fluctuated with ventilation, with an increase whenever ventilation resumed either after a respiratory pause or transient reduction in breathing amplitude. HR reached a peak before the end of the hyperpneic phase. During PB, the mean higher HR was 72.4±8.8 b/min (range 56.7–88.0 b/min) at BC1 and 63.3±6.0 b/min (range 52.8–71.0 b/min) at BC2 (p<0.0002) and the mean lower HR was 53.6±7.5 b/min (range 41.7–64.9 b/min) at BC1 and 43.6±7.3 b/min (range 31.6–53.2 b/min) at BC2 (p<0.0001). Changes in amplitude of HR fluctuations during PB at BC1 and BC2 were not statistically different (18.7±4.6 b/min vs. 19.9±6.8 b/min) (Fig. 4).
All subjects mean±SD values of lowest heart rate (HR) and highest HR during periodic breathing (PB) at Everest North Base Camp (5180 m), at the 1st (BC1) and the 10th (BC2) night.
Discussion
The main goal of our study was to assess the relationship of PB during sleep at high altitude with both Sao2 and HR behavior to possibly identify effects of hypoxia and acclimatization on these variables during sleep. In fact, it is well known that healthy subjects at high altitude exhibit PB while asleep, and our study reports the analysis of PB data during sleep and the relationship with Sao2 and HR resulting from a three-step evaluation (once at SL and twice at HA) of nine elite climbers ascending to high altitude and staying there for 10 days. As oxygen saturation increases from BC1 to BC2, our experimental design of paired studies at two different times of acclimatization allows comparisons between different levels of hypoxemia. In fact, the 10-day period of acclimatization was associated with an improvement in hypoxemia during both wakefulness and sleep, without any consistent effect of PB on overnight Sao2. However, PB does not vanish, but rather increases in most subjects during the same period. This is consistent with the persistence of PB observed in 34 mountaineers who climbed from 3750 m within 19–20 days to the summit of Muztagh Ata at 7546 m (Bloch et al., 2010), in five subjects during 28 days at 5050 m (Salvaggio et al., 1998), and by another report on nine subjects showing, despite increasing Sao2, no reduction in PB over the course of 5 days at 3200 m (Zielinski et al., 2000). PB occurs from a disbalance of the negative feedback loop of ventilation control (Kupper T, et al., 2008).
We found an increase in PB cycle time after a 10 days sojourn at high altitude. This finding is in according with the PB model suggesting that cycle time should increase as saturation increases (Khoo et al., 1982) and consistent with the findings that cycle time decreases with ascent to high altitude (shorter cycle length with increasing hypoxia) (West et al., 1986).
Malconian et al. (1990) showed during sleep in normal young subjects at high altitude, cycling of the heart rate with periodic breathing. Our analysis of the HR during PB at high altitude shows that, in healthy subjects, HR fluctuates with ventilation, with an increase whenever ventilation increases after a respiratory pause or transient reduction in breathing amplitude, as it occurs during PB in various pathological conditions (Cirignotta et al., 1987; Van de Borne et al., 1998). HR behavior is highly reproducible in each subject and similar at both stages of acclimatization. HR responses usually showed brisk changes (i.e., a peak during the ventilatory phase), as well as periods with minor changes during respiratory pauses or transient reduction in breathing amplitude.
Previous study in healthy subjects showed HR fluctuations similar to ventilatory fluctuations during voluntary normoxic PB (Lorenzi-Filho et al., 1999). At high altitude, hypoxia could also be involved in the increasing HR behavior during the ventilatory period because it causes HR to accelerate through stretch receptor stimulation while ventilation is maintained (pulmonary inflation reflex) (Coleridge et al., 1991). An additional factor operating during the ventilatory phase could be the arterial baroreflex, whose activation is suggested by the sudden drop of HR in the second portion of the ventilatory phase. Similar to the ventilatory phase, factors like hypoxemia and baroreceptor activity could influence cardiocirculatory behavior during the respiratory pause. A possible hypothesis is that hypoxia plays a role in the HR decrease, since hypoxia induces bradycardia in the absence of ventilation (diving reflex) (Coleridge et al., 1991).
Another possible factor is a central influence on the cardiocirculatory and respiratory activities, as previously suggested (Hanly et al., 1989; Franklin et al., 1997), which could be represented by arousals (Davies et al., 1993), a well-recognized cause of HR increase during sleep. Therefore, it is possible that central influences other than arousal mechanisms take place.
Conclusion
The current study provides data of the breathing pattern obtained in a sample of elite climbers ascending to high altitude on nocturnal Sao2 and on HR. The data show that during the 10-day exposure to high altitude, the process of adaptation to the environmental hypoxia is characterized by an increase in SaO2 values, both during wakefulness and sleep. PB tends to increase during the stay at high altitude in association with a longer cycle time, and a reduced HR with fluctuations associated with PB, despite improvements in Sao2 due to acclimatization. We have shown, during sleep at high altitude in elite climbers, the occurrence of PB with related repetitive HR swings that are synchronous with the PB cycle. The hyperpneic part of PB consists of breaths of high tidal volume in which the Pao2 rises and Paco2 falls, but without any consistent effect on increasing overnight arterial oxygen saturation.
Footnotes
Acknowledgments
The authors would like to thank A. da Polenza (Ev-K2-CNR Project, Head of “K2-2004 50 years later” Italian Expedition to Everest and K2) on behalf of all members of the Expedition, and Ente Italiano per la Montagna for funding this study and for providing technical and logistical support.
Author Disclosure statement
All authors declare that they have no institutional, commercial, or other interests that could pose a conflict of interest regarding the publication of the study.
References
1.
AnholmJD, PowlesACP, DowneyRIII, HoustonCS, SuttonJR, BonnetMH, CymermanA. 1992. Operation Everest II: Arterial oxygen saturation and sleep at extreme simulated altitude. Am Rev Respir Dis, 145:817–826.
2.
BerssenbruggeA, DempseyJ, IberC, SkatrudJ, WilsonP. 1983. Mechanisms of hypoxia-induced periodic breathing during sleep in humans. J Physiol, 343:507–524.
3.
BlochKE, LatshangTD, TurkAJ, HessT, HeftiU, MerzTM, BoschMM, BarthelmesD, HeftiJP, MaggioriniM, SchochOD. 2010. Nocturnal periodic breathing during acclimatization at very high altitude at Mount Muztagh Ata (7,546 m)Am J Respir Crit Care Med, 182:562–568.
4.
CirignottaF, MondiniS, SchiavinaM, ZucconiM, CoccagnaG, LugaresiE. 1987. Cheyne-Stokes breathing and systemic arterial pressure periodic pattern during sleep in central alveolar hypoventilation. Bull Eur Physiopathol Respir, 23:409–412.
5.
ColeridgeHM, ColeridgeJCG, JordanD. 1991. Integration of ventilatory and cardiovascular control systems. The Lung. CrystalRG, WestJB. Raven, New York, 1405–1418.
6.
CrawfordRD, SeveringhausJW. 1978. CSF pH and ventilatory acclimatization to altitude. J Appl Physiol, 45:275–283.
7.
DaviesRJ, BeltPJ, RobertsSJ, AliNJ, StradlingJR. 1993. Arterial blood pressure responses to graded transient arousal from sleep in normal humans. J Appl Physiol, 74:1123–1130.
8.
FranklinKA, SandstromE, JohanssonG, BalforsEA. 1997. Hemodynamics, cerebral circulation, and oxygen saturation in Cheyne-Stokes respiration. J Appl Physiol, 83:1184–1191.
9.
HanlyPJ, MillarTW, SteljesDG, BaertR, FraisMA, KrygerMH. 1989. Respiration and abnormal sleep in patients with congestive heart failure. Chest, 96:480–488.
10.
InsalacoG, RomanoS, SalvaggioA, BraghiroliA, LanfranchiP, PatrunoV, DonnerCF, BonsignoreG. 1996. Cardiovascular and ventilatory response to isocapnic hypoxia at sea level and at 5,050 m. J Appl Physiol, 80:1724–1730.
11.
InsalacoG, RomanoS, SalvaggioA, MarroneO, BonsignoreMR, BraghiroliA, LanfranchiP, PatrunoV, DonnerCF, BonsignoreG. 2000. BP and HR during periodic breathing at high altitude. J Appl Physiol, 89:947–955.
12.
JohnsonPL, EdwardsN, BurgessKR, SullivanCE. 2010. Sleep architecture changes during a trek from 1400 to 5000 m in the Nepal Himalaya. J Sleep Res, 19:148–156.
13.
KhooMC, KronauerRE, StrohlKP, SlutskyAS. 1982. Factors inducing periodic breathing in humans: A general model. J Appl Physiol, 53:644–659.
14.
KhooMC. 2000. Determinants of ventilatory instability and variability. Respir Physiol, 122:167–182.
15.
Küpper, SchöfflV, NetzerN. 2008. Cheyne Stokes breathing at high altitude: A helpful response or a troublemaker?Sleep Breath, 12:123–127.
16.
LahiriS. 1972. Dynamic aspects of regulation of ventilation in man during acclimatization to high altitude. Respir Physiol, 16:245–258.
17.
Lorenzi-FilhoG, DajaniHR, LeungRST, FlorasJS, BradleyTD. 1999. Entrainment of blood pressure and heart rate oscillations by periodic breathing. Am J Crit Care Med, 159:1147–1154.
18.
MalconianM, HultgrenH, NittaM, AnholmJ, HoustonC, FailsH. 1990. The sleep electrocardiogram at extreme altitudes (Operation Everest II)Am J Cardiol, 65:1014–1020.
19.
MasuyamaS, ShinozakiT, KohchiyamaS, OkitaS, KimuraH, HondaY, KuriyamaT. 1990. Heart rate depression during sleep apnea depends on hypoxic chemosensitivity. Am Rev Respir Dis, 141:39–42.
20.
Nussbaumer-OchsnerY, UrsprungJ, SiebenmannC, MaggioriniM, BlochKE. 2012. Effect of short-term acclimatization to high altitude on sleep and nocturnal breathing. Sleep, 35:419–423.
21.
ReiteM, JacksonD, CahoonRL, WeilJV. 1975. Sleep physiology at high altitude. Electroencephalogr Clin Neurophysiol, 38:463–471.
22.
SalvaggioA, InsalacoG, MarroneO, RomanoS, BraghiroliA, LanfranchiP, PatrunoV, DonnerCF, BonsignoreG. 1998. Effects of high altitude periodic breathing on sleep and arterial oxyhemoglobin saturation. Eur Respir J, 12:408–413.
23.
SatoM, SeveringhausJW, BicklerP. 1994. Time course of augmentation and depression of hypoxic ventilatory responses at altitude. J Appl Physiol, 77:313–316.
24.
SuttonJR. 1982. Sleep disturbances at high altitude. Physician Sports Med, 10:79–84.
25.
Van de BorneP, OrenR, AbouassalyC, AndersonE, SomersVK. 1998. Effect of Cheyne-Stokes respiration on muscle sympathetic nerve activity in severe congestive heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am J Cardiol, 81:432–436.
26.
WeilJV. 2004. Sleep at high altitude. High Alt Med Biol, 5:180–189.
27.
WestJB, PetersRMJr, AksnesG, MaretKH, MilledgeJS, SchoeneRB. 1986. Nocturnal periodic breathing at altitudes of 6,300 and 8,050 m. J Appl Physiol, 61:280–287.
28.
WestJB, SchoeneRB, MilledgeJS. 2007. High Altitude Medicine and Physiology. Hodder Arnold: London, UK.
29.
WhiteDP, GleesonK, PickettCK, RannelsAM, CymermanA, WeilJV. 1987. Altitude acclimatization: Influence on periodic breathing and chemoresponsiveness during sleep. J Appl Physiol, 63:401–412.
30.
ZielinskiJ, KoziejM, MankowskiM, SarybaevAS, TursalievaJS, SabirovIS, KaramuratovAS, MirrhakimovMM. 2000. The quality of sleep and periodic breathing in healthy subjects at an altitude of 3,200 m. High Alt Med Biol, 1:331–336.