
Abstract
Abstract
Staab, Janet E., Beth A. Beidleman, Stephen R. Muza, Charles S. Fulco, Paul B. Rock, and Allen Cymerman. Efficacy of residence at moderate versus low altitude on reducing acute mountain sickness in men following rapid ascent to 4300 m. High Alt Med Biol 14:13–18, 2013.—To determine if residence at moderate (∼2000 m) compared to low (<50 m) altitude reduces acute mountain sickness (AMS) in men during subsequent rapid ascent to a higher altitude. Nine moderate-altitude residents (MAR) and 18 sea-level residents (SLR) completed the Environmental Symptoms Questionnaire (ESQ) at their respective baseline residence and again at 12, 24, 48, and 72 h at 4300 m to assess the severity and prevalence of AMS. AMS cerebral factor score (AMS-C) was calculated from the ESQ at each time point. AMS was judged to be present if AMS-C was ≥0.7. Resting end-tidal CO2 (PETco2) and arterial oxygen saturation (Sa
Introduction
Previous studies have reported that long-term (3 months to life) moderate-altitude residence (i.e., 1500 to 2600 m) induces sustained ventilatory and hematologic responses that allow individuals (e.g., troops) to acclimatize to higher altitudes more rapidly than sea-level residents (SLR) (Boning et al., 2001; Brothers et al., 2007; Brothers et al., 2010; Muza et al., 2004; Reeves et al., 1993; Schmidt et al., 2002). Previous studies, for example, reported a smaller decrement in both maximal and prolonged exercise performance in the first few days following rapid ascent to 4300 m in moderate-altitude residents (MAR) compared to SLR (Fulco et al., 2005; Fulco et al., 2007; Maresh et al., 1983). The degree that the severity and prevalence of AMS might also be improved at a higher altitude by first living for prolonged periods of time at moderate altitudes is largely unknown.
Several studies of short-term (i.e., 2–6 days) residence at moderate altitudes of 1600–3400 m have indicated that AMS is reduced by 20%–60% during the first few days at a higher altitude (Beidleman et al., 2009; Hansen et al., 1967; Stamper et al., 1980); presumably, longer-term moderate-altitude residence should reduce AMS symptoms even more, since many physiologic and hematologic adaptations may take as long as 17 months to develop fully at moderate altitude (Brothers et al., 2007). This hypothesis, however, has never been systematically and quantitatively assessed.
Therefore, the purpose of this study was to determine the extent that beneficial ventilatory and hematologic adaptations resulting from long-term (i.e., 5–46 months) moderate-altitude residence (i.e, 1800–2200 m) would reduce AMS severity and prevalence over the first several days at 4300 m following rapid ascent. To that end, we retrospectively analyzed data from two previous studies of SLR and MAR rapidly exposed to 4300 m that were conducted by our laboratory using identical procedures, equipment, and facilities (Fulco et al., 2007; Hagobian et al., 2006).
Methods
Study volunteers
Nine active duty military men (mean±SD; 30±3 yr, 74±6 kg, 179±5cm, 41±5 mL/kg/min) living in Colorado Springs, CO (MAR) and 18 physically active men (25±5 yr, 78±8 kg, 179±5cm, 57±7 mL/kg/min) living in the vicinity of Palo Alto, CA (SLR) volunteered to participate in these two studies. Prior to the study, MAR resided at 1800 to 2200 m for a mean of 21±3 mo (range: 5–46 months) while the SLR had not resided at altitudes greater than 2000 m for the 6 months immediately prior to the study. All participated in regular physical training for 3 to 6 days a week. All were nonsmokers and in good health as determined by medical history and evaluation. Each provided written informed consent before participating. Both studies were approved by the institutional review board (IRB) at the U.S. Army Research Institute of Environmental Medicine. The MAR study was also approved by the IRB for the U.S. Air Force Academy (USAFA) and the SLR study was approved by the IRB for the Veterans' Administration Palo Alto Health Care System (VAPAHCS). Investigators adhered to the policies for protection of human subjects as prescribed in Army Regulation 70-25 and the research was conducted in adherence with the provisions of 32 CFR Part 219.
Study overview
Both studies used a prospective design in which the participants were first evaluated at their respective baseline residence and then evaluated again following a rapid ascent to the same laboratory located at the summit of Pikes Peak, CO (4300 m, 458–464 mmHg).
MAR study design
The MAR reported on 3 separate days to the Human Performance Laboratory at the USAFA (2200 m, 589–596 mmHg) for testing, which was conducted in a room maintained at a temperature and relative humidity of 21±2°C and 45±5%, respectively. Volunteers were familiarized with all test procedures on day 1, AMS and body weight (BW) measurements were conducted after the first morning void each day, peak oxygen uptake (
SLR study design
The SLR reported on 3 separate days to the Clinical Studies Unit at the VAPAHCS (15 m, 748–762 mmHg) for testing in a room where the temperature and relative humidity were maintained at 21±2°C and 45±5%, respectively. Volunteers were familiarized with all test procedures on day 1, AMS and BW measurements were conducted after the first morning void each day,
Altitude-illness assessment
AMS severity and prevalence were assessed at baseline in the morning and again at 4300 m at 12, 24, 48, and 72 h using the shortened electronic version (Beidleman et al., 2007) of the Environmental Symptoms Questionnaire (ESQ) (Sampson et al., 1994). The ESQ was used to quantify a weighted AMS cerebral factor score (AMS-C) to assess AMS severity. At each time point, AMS was judged to be present if an individual's AMS-C score was ≥0.7 (Sampson et al., 1994).
Ventilatory and cardiovascular assessment
Resting ventilation was measured in the morning prior to breakfast at baseline residence and at 24, 48, and 72 h at 4300 m. Volunteers sat in a semi-recumbent position and breathed through a low-resistance breathing circuit connected to a breath-by-breath open circuit metabolic system (Vmax 229, Sensormedics Inc., Yorba Linda, CA) calibrated with certified gases and volume standard. Each volunteer's resting minute ventilation (
Hematologic assessment
Immediately following the resting ventilation measurements at baseline and at 72 h at 4300 m, venous blood samples were obtained from the forearm without stasis for the measurement of [Hb] and Hct. The samples were analyzed immediately in duplicate using the i-STAT portable clinical analyzer (Abbott Diagnostics, Abbot Park, IL). Percent change in plasma volume (PV) from baseline residence values to 4300 m was calculated according to the Dill equation (Dill and Costill, 1974).
Sleep assessment
During the first night at 4300 m, volunteers wore a small pulse oximeter (Nonin model 3100) on the nondominant wrist with an adhesive finger sensor that measured and recorded SaO2 and HR continuously (beat by beat) averaging over the entire sleep period. Two volunteers in the MAR group and four volunteers in the SLR group did not complete the sleep assessment due to equipment malfunction.
Statistical analyses
For all measurements, a two-way mixed factorial repeated measures ANOVA was used to analyze differences between the independent group factor (MAR vs. SLR) and test conditions (baseline residence, and the 12th, 24th, 48th, and 72nd h at 4300 m using Statistica v11.0 (Statsoft, Tulsa, OK). Significant main effects and interactions were analyzed using Tukey's least significant difference test. The Cochran's Q test was used to evaluate differences in the prevalence of AMS over test conditions within each group. For all tests, statistical significance was set at p<0.05. Data are presented as means±SD when appropriate.
Results
Altitude-illness measures
There were no significant differences in AMS-C scores between MAR and SLR, and no individuals in either group had scores indicative of AMS at baseline (Fig. 1). Both AMS-C scores and the prevalence of AMS were significantly lower in the MAR compared to the SLR throughout the altitude exposures (Fig. 1).
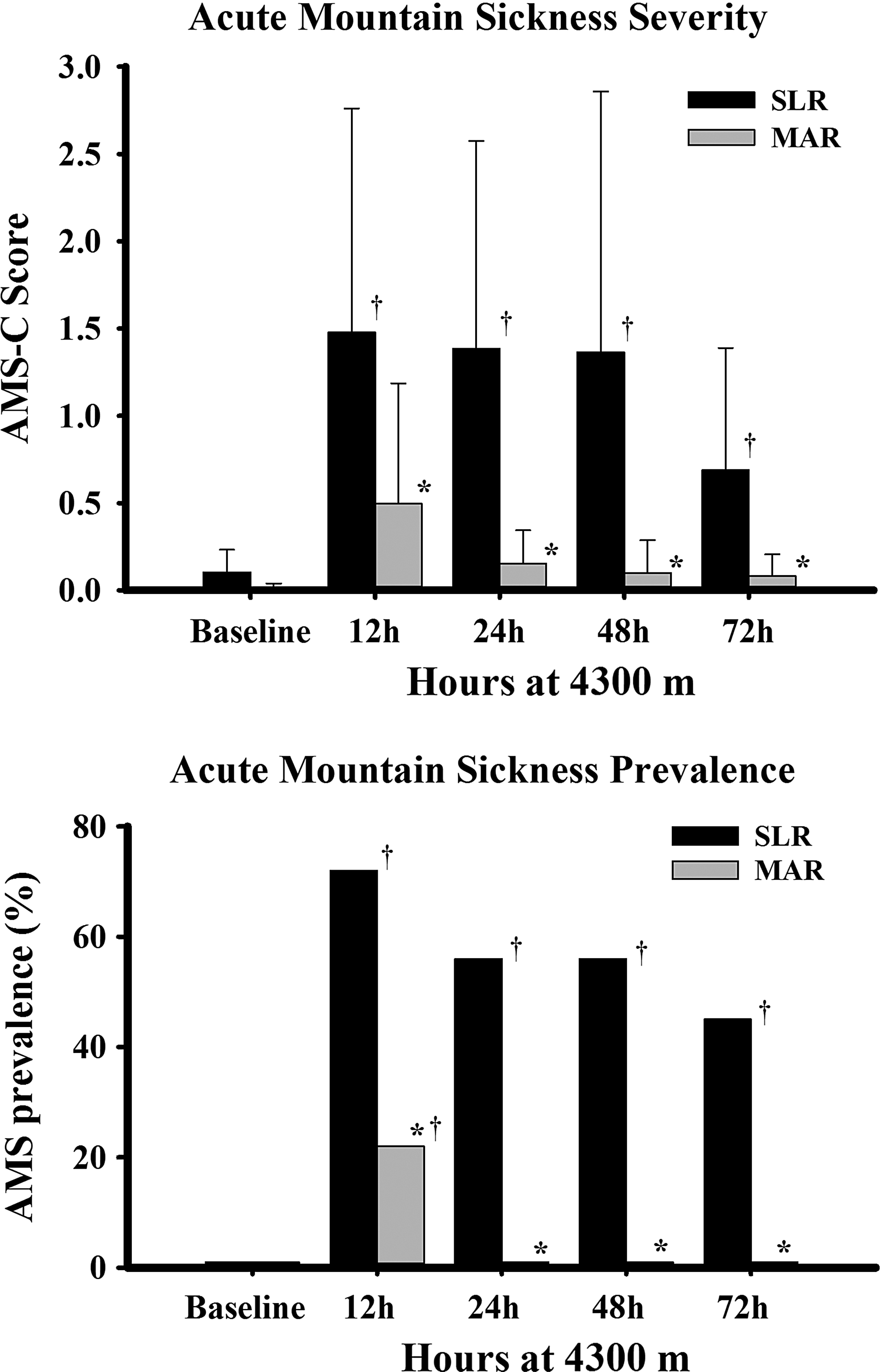
Acute mountain sickness severity scores (AMS-C) and prevalence (%) of moderate-altitude residents (MAR) and sea-level residents (SLR) at their baseline residence and on the summit of Pikes Peak (4300 m) after 12, 24, 48, and 72 hours. Values for AMS-C are presented as mean±SD, and values for AMS prevalence are presented as proportions. *p<0.05 between groups; †p<0.05 from baseline.
Resting ventilatory and cardiovascular measures of acclimatization
Both ventilatory and cardiovascular measures were higher in the MAR group relative to the SLR group at baseline (Table 1). In addition, ventilatory and cardiovascular measures were increased in both groups in the first few days at 4300 m, but the increase was less dramatic in the MAR. PET
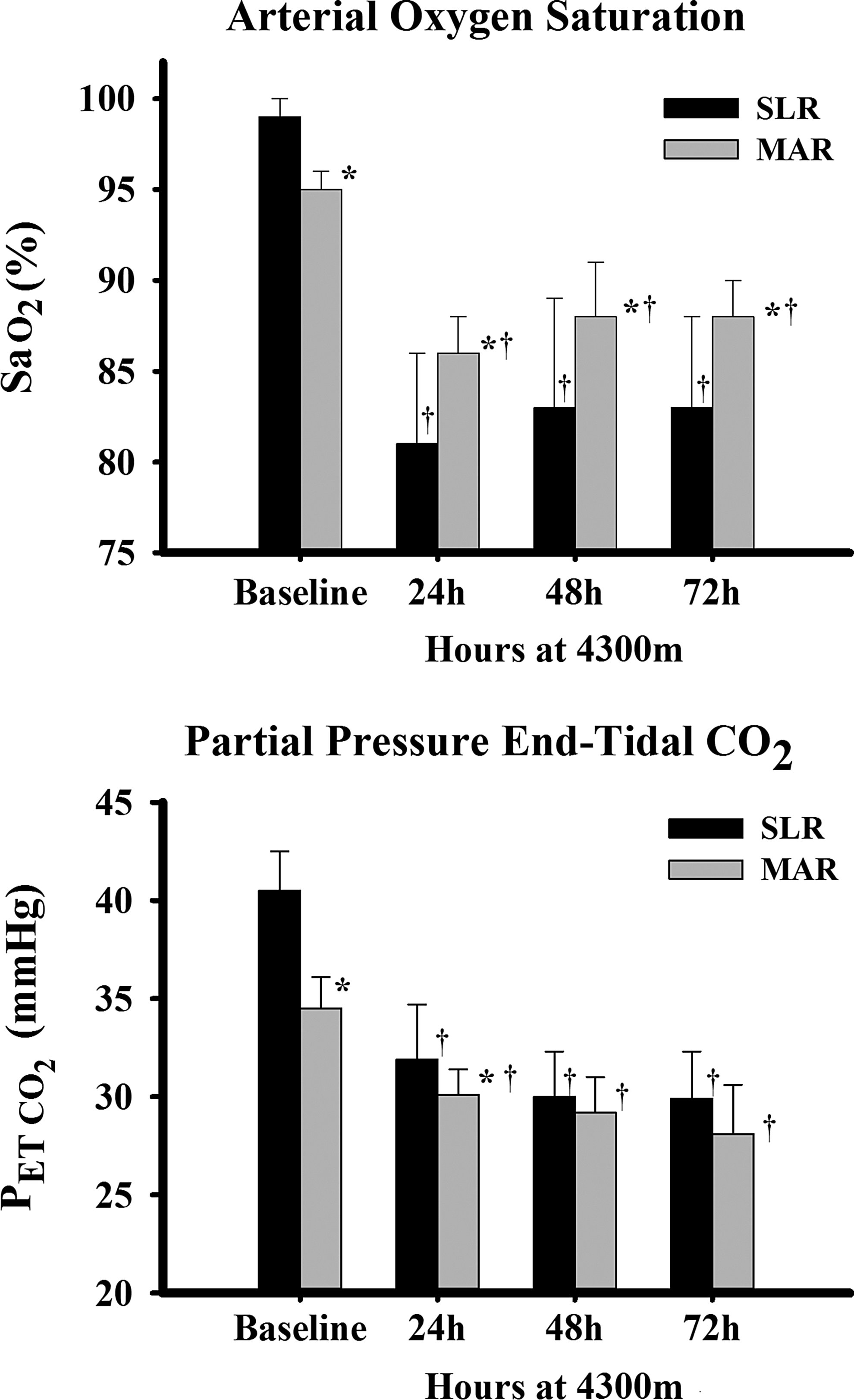
Arterial oxygen saturation (Sa
HR, heart rate; MAP, mean arterial pressure; PETCO2, partial pressure of end-tidal carbon dioxide; PETO2, partial pressure of end-tidal oxygen; RER, respiratory exchange ratio; SaO2, arterial oxygen saturation;
Exercise and sleep arterial oxygen saturation
In the first few hours at 4300 m during exercise, Sa
Resting hematologic measures of acclimatization
The [Hb] (g/dl) and Hct (%) were higher at baseline in the MAR (16.1±0.8 and 47.1±1.9) compared to the SLR (15.0±1.0 and 45.1±2.9). [Hb] and Hct increased from baseline to 72 h for the SLR (15.8±1.0 and 47.1±2.7) but not the MAR (15.7±0.5 and 46.1±1.4), resulting in an estimated PV reduction for the SLR (−8.1±10.4%) but not the MAR (4.5±6.7%). The change in PV at 72 h at 4300 m was significantly different between groups (p=0.002).
Discussion
Retrospective analysis of data from our two previous studies conducted using similar experimental procedures showed that the ventilatory and hematologic adaptations acquired while living at moderate altitude were associated with reduced AMS prevalence and symptom scores compared to low altitude residents following a rapid ascent to 4300 m. Symptoms scores were reduced by ∼70% to 90% in MAR compared to SLR, and AMS was completely absent in the MAR group after 24 h at 4300 m. This effect is more than the 46% reduction in AMS symptom scores observed in another study following a 6-day residence at the same moderate altitude prior to ascent to 4300 m (Beidleman et al., 2009). The ventilatory and hematologic adjustments induced by long-term moderate-altitude residence, as evidenced by a higher resting ventilation and [Hb] at the baseline residence and the subsequent higher resting, exercise, and sleep Sa
The ventilatory changes induced by moderate-altitude residence in this study are similar to those reported by others for men and women residing at similar altitudes (Maresh et al., 1988; Muza et al., 2004; Reeves et al., 1993). At baseline, we observed a ∼15% higher resting alveolar ventilation, as reflected by a lower PET
During the first 72 h of exposure to 4300 m, the MAR in the present study maintained a ∼5% lower level of resting PET
The MAR also had a 7% higher [Hb] than the SLR when measured at baseline. This finding is consistent with the results of others that have reported that MAR living at 1800 to 2600 m have a 6%–13% higher [Hb] than SLR measured at their respective residence or shortly after arriving at moderate altitude (Boning et al., 2001; Brothers et al., 2007; Brothers et al., 2010; Maresh et al., 1985; Schmidt et al., 2002). The MAR in the present study did not maintain the ∼ 7% elevated [Hb] compared to the SLR when measured at 72 h of exposure to 4300 m. In fact, both groups reached the same [Hb] and Hct values at 72 h of exposure because only the SLR lost PV. Some reports have suggested that AMS is related to acute impairments in fluid balance regulation during exposure to high altitude (Loeppky et al., 2005a; Loeppky et al., 2005b; Westerterp et al., 1996). The observation that MAR have already achieved body fluid homeostasis prior to exposure to a higher altitude may put them at less risk for developing AMS.
The conclusions resulting from this study may be limited due to the following conditions: 1) this was a retrospective analysis of two studies that were not originally designed with the present purpose in mind; 2) the analysis was conducted only on men; and 3) although physical fitness has not been shown to impact AMS, the
Conclusions
In conclusion, long-term moderate-altitude residence is associated with ventilatory and hematologic acclimatization that decreases the severity and prevalence of AMS in men following rapid ascent to 4300 m. These AMS results in combination with the previously reported improvements in physical performance indicate that residence at moderate altitude is very effective in sustaining health and performance upon rapid ascent to high altitude.
Footnotes
Acknowledgments
The dedicated and professional efforts of LTC Michael Zupan, Ph.D., Ann Friedlander, Ph.D., Kevin Jacobs, Ph.D., Andrew Subudhi, Ph.D., Todd Hagobian, Ph.D., Ken Kambis, Ph.D., Ellen Glickman, Ph.D, Margaret Ardelt, Ph.D., SGT Dave Degroot, SGT Mike Tapia, and SGT Dennis Rufolo supporting the collection and analysis of the data are acknowledged and greatly appreciated. The dedication and efforts of the test volunteers in completing these studies are also acknowledged and appreciated.
Author Disclosure Statement
The authors have no conflicts of interest or financial ties to report. Approved for public release; distribution is unlimited. The views, opinions, and/or findings contained in this publication are those of the authors and should not be construed as an official Department of the Army position, policy or decision unless so designated by other documentation. Any citations of commercial organizations and trade names in this report do not constitute an official Department of the Army endorsement of approval of the products or services of the organizations.