
Abstract
Abstract
Davis, John E., Dale R. Wagner, Jesssica Thorington, and Cory Schall. Orthostatic responses at 4860 m in low, moderate, and high altitude residents. High Alt Med Biol 14:251–255, 2013—This study evaluated the influence of altitude of residence on orthostatic responses when exposed to high altitude. Data collection took place at the Carrel hut (4860 m) on Chimborazo in Ecuador. After being transported to the hut by vehicle, 69 people volunteered for the study. A 3-min stand test (rapid change from supine to standing) provided an orthostatic challenge while resting heart rate (RHR), systolic (SBP) and diastolic (DBP) blood pressures, and arterial oxygen saturation (SpO2) were measured. Participants were separated into four groups based on altitude of residence and ethnicity: LOW (<1500 m; n=15), MOD (1500–3000 m, n=30), and HIGH (>3000 m, n=11) Ecuadorians, and non-Ecuadorian lowlanders (NE-LOW, n=13). Supine and standing RHRs were lower (p<0.05) for HIGH compared to other groups. Furthermore, standing increased RHR in LOW, MOD, and NE-LOW by 11.9±5.3, 9.5±4.1, and 11.6±7.4 bpm, respectively, while HIGH stayed the same (0.6 bpm increase±3.3). Additionally, mean arterial pressure decreased slightly but not significantly upon standing in all groups except HIGH. The difference in Sp
Introduction
Any additional physiological stressor, such as altitude-induced hypoxia, may have a detrimental effect on orthostatic tolerance. As altitude increases, the partial pressure of oxygen decreases, further diminishing the oxygen supply to the brain and exacerbating the symptoms of presyncope. In fact, it has been shown in numerous studies that orthostatic tolerance is diminished at altitude (Blaber et al., 2003; Claydon et al., 2005; Malhotra and Murthy, 1977; Mytton et al., 2008; Rickards and Newman, 2002; Sagawa et al., 1993). Blaber et al. (2003) reported that the increased prevalence and severity of presyncope at high altitude is due to ineffective peripheral vasoconstriction and insufficient cerebral perfusion due to cerebral vasoconstriction as a result of hypoxic hyperventilation-induced hypocapnia.
Given the many physiological adaptations that occur to aid in wellbeing at high altitude, it is logical to assume that high-altitude natives might respond better than lowlanders to orthostatic stress at high altitude. Indeed, Claydon et al. (2004) found that Peruvian highlanders, regardless of whether they were healthy or had chronic mountain sickness, had exceptional orthostatic tolerance when tested at 4338 m. They hypothesized that high hematocrit and large packed cell and blood volumes contributed to their ability to withstand orthostatic stress. However, this same research team later reported that Ethiopian highlanders had orthostatic tolerances similar to that of lowlanders from the United Kingdom, both less tolerant of orthostasis than the Peruvian highlanders (Gulli et al., 2007). This raises the question as to whether orthostatic tolerance is a result of adaptation to high altitude or an ethnic-specific difference. To address this question, Gulli et al. (2007) suggested that comparisons should be made between ethnically similar highlanders and lowlanders. Thus, the purpose of our study was to evaluate the influence of altitude of residence on orthostatic responses of Ecuadorians when exposed to high altitude. We hypothesized that high altitude residents would have an improved cardiovascular response to an orthostatic challenge when exposed to high altitude because of long-term physiological adaptations.
Materials and Methods
Setting and participants
This study took place inside the Carrel hut (4860 m), a refugio which can be reached by vehicle on Chimborazo (6310 m). The summit of Chimborazo is the highest point in Ecuador; as such, tourists and Ecuadorians from various altitudes of residence often travel to the Carrel hut to view the mountain. Those who arrived at the hut during the data collection period were invited to participate in the study. Only those participants who had come directly to the mountain from their altitude of residence were asked to participate. Volunteers were informed about the purpose and procedures of the study. They signed a written informed consent, which was available in both English and Spanish. The study was approved by the Institutional Review Board of Alma College and Equitorialis University of Quito, Ecuador. Sixty-nine participants (47 men, 22 women; age=37.2±10.4 years) completed the study.
Procedures
Cardiovascular measurements included resting heart rate (RHR), oxygen saturation (Sp
Statistical analyses
Data were separated into four groups based on the altitude of residence of the study participants: low altitude Ecuadorians (LOW;<1500 m, n=15), moderate altitude Ecuadorians (MOD; 1500–3000 m, n=30), high altitude Ecuadorians (HIGH;>3000 m, n=11), and non-Ecuadorian tourists who resided at low altitude (NE-LOW, n=13). Analysis of variance (ANOVA) with Tukey's Post-Hoc test was done to determine significant mean differences among the groups. Statistical significance was accepted with a p value<0.05. All statistical analyses were done using SPSS (version 19, IBM, Armonk, NY).
Results
Resting heart rate (RHR) increased in response to standing in all of the groups except the HIGH group (Fig. 1). Additionally, the HIGH group had lower RHRs at every position compared to the other three groups. SBP decreased immediately upon standing in all groups except the HIGH group. SBP was significantly lower in the HIGH group relative to the other three groups at each time point, and DBP was highest in the LOW group. This resulted in a significantly lower mean arterial pressure (MAP) for the HIGH group relative to the other groups (Fig. 2). Furthermore, MAP was maintained upon standing for the HIGH group, but dropped slightly for the other subjects (Fig. 2). Symptoms of orthostatic intolerance (lightheadedness, dizziness) were noted in 26% (4/15) of the LOW group, 43% of the MOD group (13/30), 9% of the HIGH group (1/11), and 23% of the NE-LOW group (3/13). The LOW group had the lowest Sp
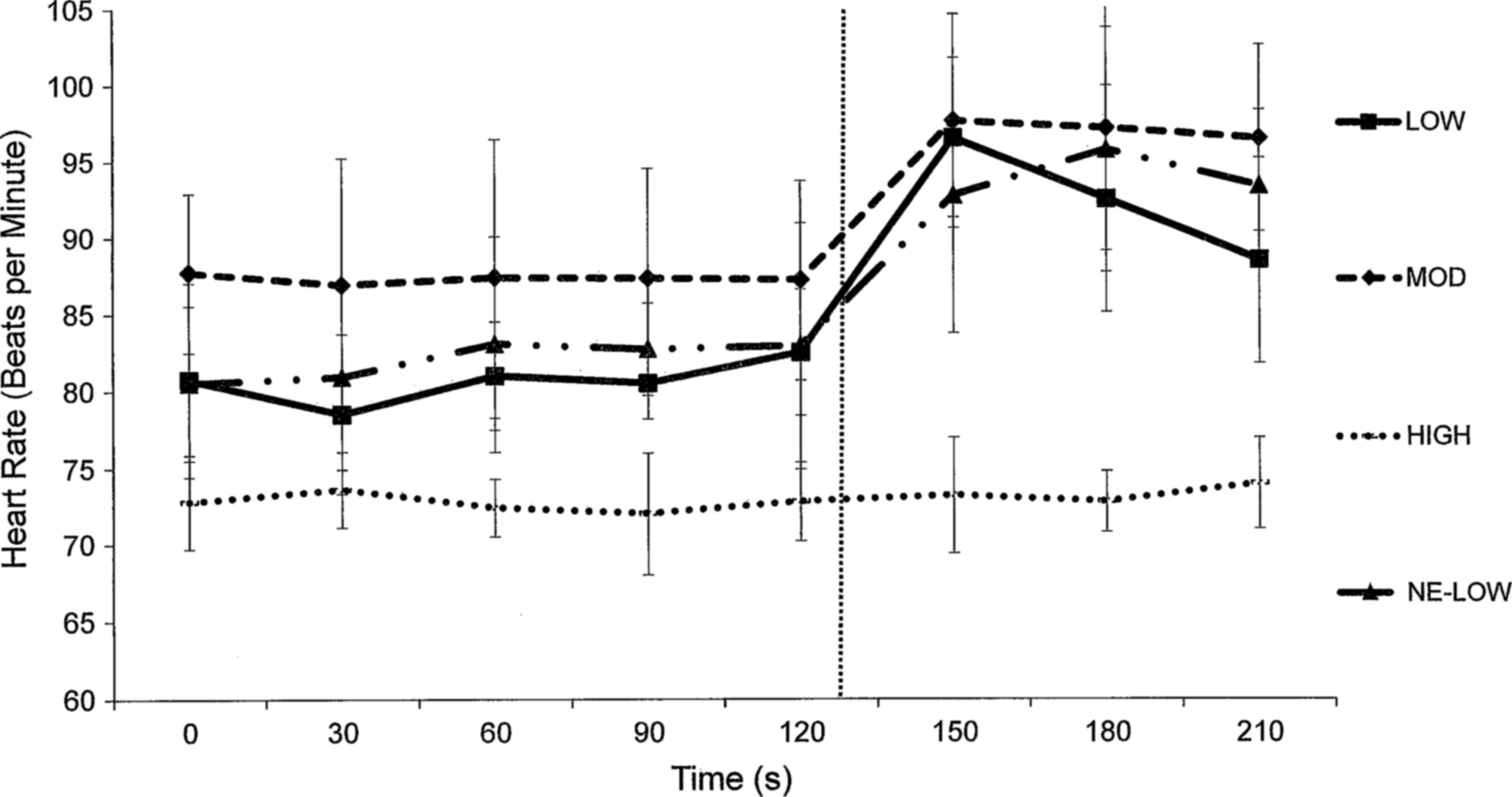
Resting heart rates during supine and standing postures. The vertical dashed line indicates standing. Means±1 SD are displayed.
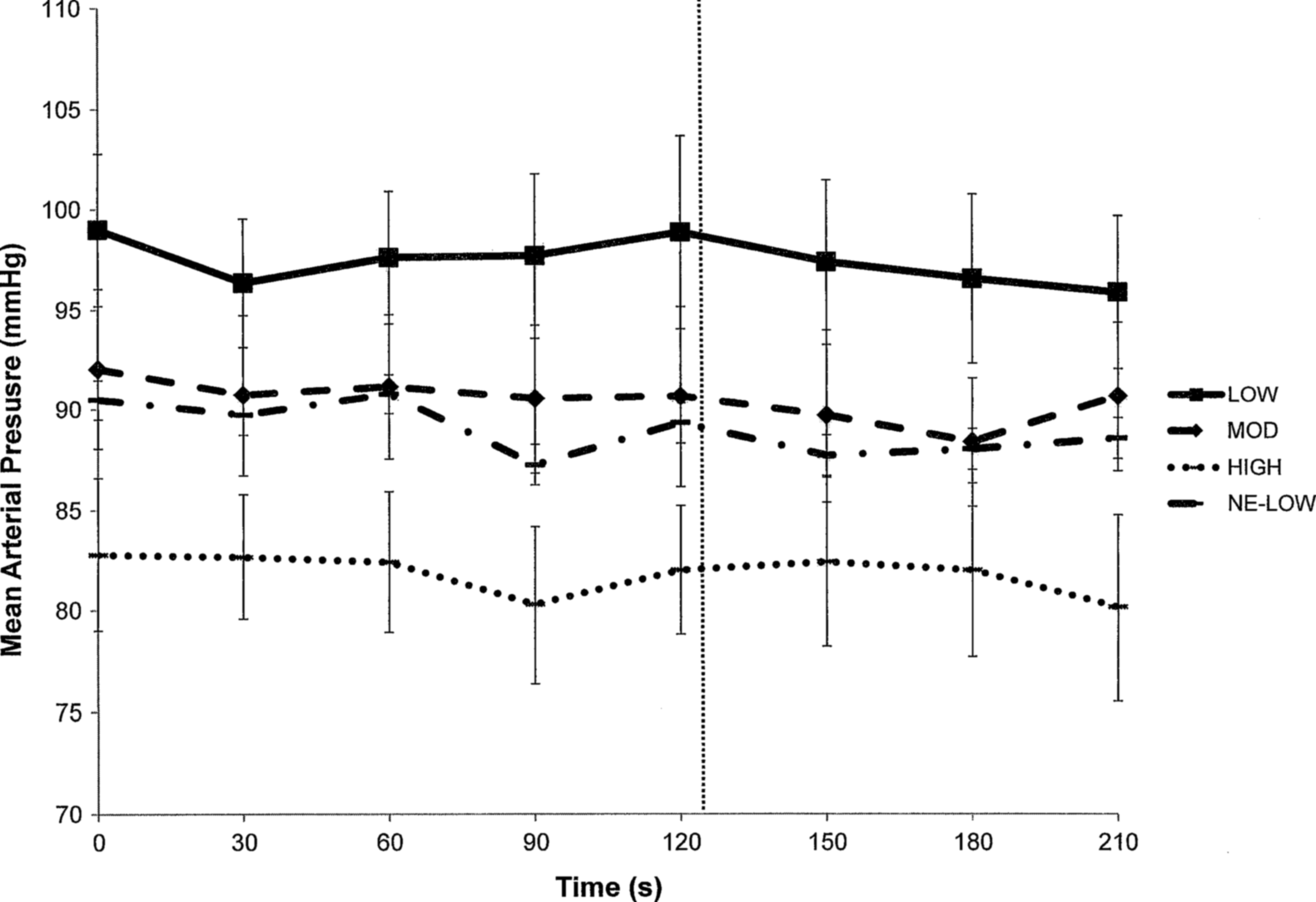
Mean arterial pressure during supine and standing postures. The vertical dashed line indicates standing. Means±1 SD are displayed.
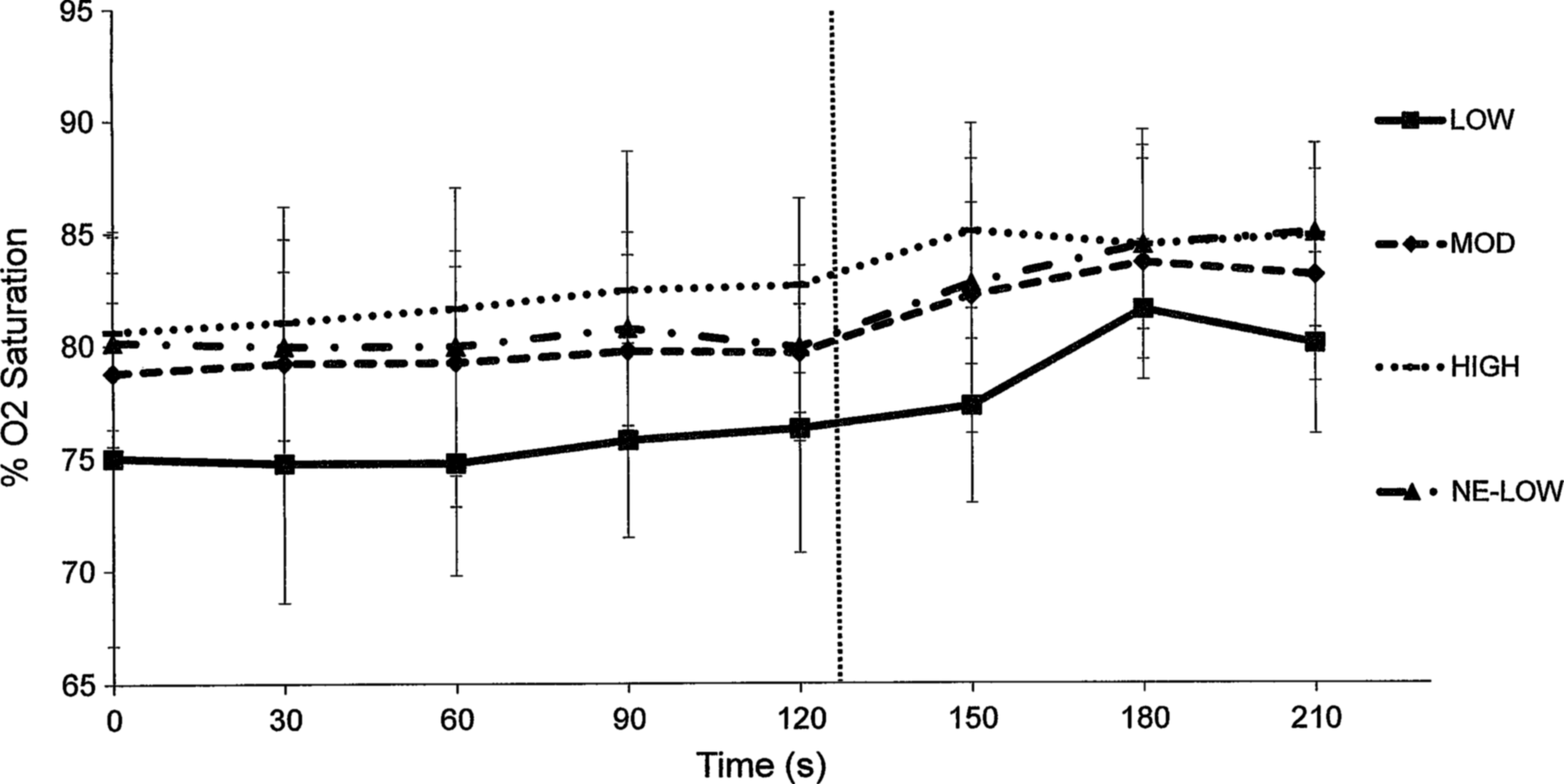
Arterial oxygen saturation during supine and standing postures. The vertical dashed line indicates standing. Means±1 SD are displayed.
Discussion
Previous researchers have tested the orthostatic tolerance of their study participants at both low and high altitudes (Blaber et al., 2003; Claydon et al., 2005; Malhotra and Murthy, 1977; Mytton et al., 2008; Rickards and Newman, 2002; Sagawa et al., 1993; Thomas et al., 2010), and Gulli et al. (2007) examined orthostasis in three different ethnicities at their respective altitudes of residence. However, to our knowledge, this is the first published study to use a single ethnic group to evaluate the influence of altitude of residence on orthostatic responses to acute exposure to high altitude. The key finding from this investigation was that Ecuadorians living at the highest altitudes (>3000 m) have minimal heart rate and blood pressure responses to orthostatic changes when tested at 4860 m.
Gulli et al. (2007) reported that both Peruvian and Ethiopian highlanders had blunted baroreflex function, yet only the Peruvians expressed exceptional orthostatic tolerance compared to sea-level Caucasians. This led these researchers to question whether exceptional orthostatic tolerance is attributed to ethnicity or altitude adaptation. Our data suggest that altitude of residence, more than ethnicity, influenced the cardiovascular responses to orthostatic stress. Only the Ecuadorians who lived at the highest altitudes showed blunted heart rate and blood pressure responses to the stand test; the LOW and MOD Ecuadorians had responses similar to those of NE-LOW. Additionally, research suggests that the cardiovascular responses to orthostatic stress in fully acclimatized individuals is not substantially different than what would be observed at sea level (Thomas et al., 2010) or compared to high altitude natives (Malhotra and Murthy, 1977), giving further credence to the idea that altitude adaptation is able to affect orthostatic tolerance. Although we did not measure blood volume, we hypothesize that the HIGH group had greater blood volume, which may have contributed to their ability to maintain stroke volume and blood pressure in spite of the orthostatic challenge. Claydon et al. (2004) reported exceptional orthostatic tolerance in Peruvian highlanders and surmised that it might be due to their great blood volume. Given that both Ecuadorian and Peruvian highlanders are Andean natives, it is logical that they might share this adaptation. High hematocrit, packed cell volume, and blood volume appear to be important for orthostatic tolerance (Claydon et al., 2004; Gulli et al., 2007).
Another possible explanation for the HIGH group's orthostatic ability is greater cerebral perfusion because of long-term acclimatization to high altitude. Blaber et al. (2003) reported that hypocapnia as a result of hyperventilation can lead to cerebral vasoconstriction and presyncope at altitude. Due to their pre-acclimatized condition from living at high altitude, the HIGH group likely experienced much less hyperventilation at 4860 m than the LOW and MOD groups, and thus greater cerebral perfusion and less symptoms of orthostatic intolerance. Furthermore, Wolff (2000) speculated that during acclimatization to high altitude cerebral blood flow would increase and compensate for the reduced arterial oxygen content and therefore maintain oxygen delivery to the brain. It is possible that our HIGH group had higher cerebral blood flows and oxygen delivery resulting in an improved orthostatic tolerance. Again, this is speculation, as we did not measure cerebral artery mean blood flow velocities, end-tidal P
An alternative explanation is peripheral chemoreflex involvement in the reduced heart rate response and improved orthostatic tolerance observed in the HIGH group. Several previous studies have reported interactions between the carotid chemoreceptors and baroreceptors (Braga et al., 2006; Stewart et al., 2011; Zoccal et al., 2008). One of these studies (Stewart et al., 2011) demonstrated that arterial baroreflexes and chemoreflexes interact in controlling ventilation. The influence of chemoreflexes on the baroreceptor control of heart rate is not as well established. Halliwell and Minson (2002) did find that acute exposure to hypoxia reset baroreflex control of both heart rate and sympathetic activity to a higher pressure without altering baroreflex sensitivity. The role of long-term acclimatization on the interaction between baroreflex and chemoreflex control of heart rate and blood pressure has not been extensively studied. However, it is possible that the findings in our HIGH subjects were due to an alteration in chemoreflex function and a diminished sympathetic response, resulting in a lower heart rate during our orthostatic challenge.
We used a supine-to-stand test to create an orthostatic stress. Cooke et al. (2009) claimed stand testing for orthostatic hypotension had low diagnostic accuracy, and a combined head-up tilt test with lower body suction (El-Bedawi and Hainsworth, 1994) has been recommended for the assessment of orthostatic tolerance. However, all three tests—stand, head-up tilt, and lower body negative pressure—have been deemed capable of measuring orthostatic responses (Hyatt et al., 1975). We chose the stand test because of its relevance to normal activity and its practicality. Mytton et al. (2008) noted that the head-up tilt test eliminates the action of the calf muscles which promote venous return, making the stand test more relevant to normal activities. Thomas et al. (2010) also cited the relevance of the stand test in selecting it for their study. From a practical standpoint, the stand test was easier than the others to administer in a refugio at 4860 m, and we surmised that Andean natives would be more comfortable and willing to participate in a study that required standing from a supine position than one that involved a tilt table or suction on their lower body.
A limitation of this study is that blood pressure measurements were obtained manually via auscultation. Beat-to-beat blood pressure measured by finger photoplethysmography would have allowed for a more rapid and complete assessment of blood pressure changes during the transition from supine to standing. Nevertheless, the same trained technician took all of the blood pressure readings to avoid inter-rator error. Additional measurements such as blood flow velocity and end-tidal P
In summary, the heart rate and blood pressure responses to an orthostatic stress of standing rapidly from a supine position at 4860 m were minimal in Ecuadorians who live above 3000 m. In contrast, Ecuadorians living at low and moderate altitudes had cardiovascular responses similar to those of non-Ecuadorian tourists, such as a significant increase in heart rate and a slight drop in systolic blood pressure upon standing. Our findings suggest that altitude of residence influences the cardiovascular responses to orthostatic stress.
Footnotes
Acknowledgments
We thank the participants who volunteered for the data collection and all of the faculty and staff at Equitorialis University for their help in making this study a success.
Author Disclosure Statement
The authors have no conflict of interest to report.