
Abstract
Abstract
Bosch, Martina M., Daniel Barthelmes, and Klara Landau. High altitude retinal hemorrhages: an update. High Alt Med Biol. 13:240–244, 2012. —Retinal hemorrhages represent a common phenomenon in eyes of high altitude climbers. In this review, we present an update about this entity, with focus on its pathophysiology and practical implications. Due to their delayed appearance in the course of an expedition, retinal hemorrhages are not predictive when assessing the risk for life-threatening complications related to hypobaric hypoxia. Consequences for ocular health depend greatly on the extent and localization of retinal bleedings, but are generally mild and reversible in healthy eyes.
Introduction
Depending on size and location, hemorrhages may go unnoticed if located peripherally of the macula or result in noticeable scotomas when located close to the fovea centralis of the retina. Small intraretinal hemorrhages may cause only slight visual disturbances, whereas a spillover of blood into the vitreous cavity may cause severe visual impairments—down to an acuity of counting fingers or less.
Treatment of hemorrhages, especially when not intense, is not required, as hemorrhages are resorbed within days or weeks—depending on the size—and usually do not result in permanent damage to the neural tissue ( Regnault 1970; Maar et al., 2000).
High Altitude-Associated Retinal Hemorrhages
The retinal hemorrhages described above also occur at high altitude—initially reported by Houston in 1968 on Mount Logan. They have been closely associated with high altitude sickness, as first described by Singh et al. (1969) in 24 of of 1925 subjects staying between 11,000 ft (3353 m) and 18,000 ft (5486 m), and Frayser et al. (1970) in nine of 25 mountaineers at an altitude of 17,500 ft (5334 m).
Changes at the posterior segment of the eye can be found in unacclimatized individuals exposed to hypobaric hypoxia at high altitudes and have been linked to the complex of altitude-related illness (AI), which also includes acute mountain sickness (AMS), high altitude cerebral edema (HACE), and high altitude pulmonary edema (HAPE) (Houston, 1976; Meehan and Zavala, 1982; Hackett and Roach, 2001). Independent risk factors for the development of AI are maximum altitude climbed to, individual susceptibility, and ascent rate (Schneider et al. 2002; Bloch et al., 2009).
Signs of high altitude retinopathy (HAR) include retinal hemorrhages (HARH), engorgement and tortuosity of retinal vessels, optic disc hyperemia and swelling, cotton wool spots, and even vitreous hemorrhage (Frayser et al., 1970; Rennie and Morrissey 1975; Shults and Swan 1975; Wiedman 1975; McFadden et al., 1981). Butler et al. (1992) reported central retinal vein occlusion in association with altitude retinopathy. A cotton wool spot is an area where nerve fiber layer infarction has taken place, which is surrounded by swollen nerve axons. This is caused by the combination of hypoxia and hypoperfusion, including further mechanisms such as probable micro-embolization due to platelet aggregates that develop during hypoxia or hypobaria (Gray et al., 1975; McFadden et al., 1981). A current study on retinal changes in various altitude diseases found patients with branch retinal vein occlusions with macular edema (Arora et al., 2011), possibly caused by increased hematocrit and hemoglobin concentrations. A classification for HAR has been established by Wiedman and Tabin (1999). They described four stages of increasing severity of high altitude retinopathy where the area of retinal bleeding parallels the occurrence of optic disc edema.
Possible Causes and Characteristics of High Altitude Retinal Hemorrhages
High altitude retinal hemorrhages (HARH, Fig. 1) are most likely induced by systemic hypoxic effects on the eye, despite regulatory adjustments by both retinal and choroidal circulation. According to data from the Muztagh Ata study in 2005, increased hematocrit, possibly representing higher blood viscosity, correlated positively with the number of hemorrhages (Barthelmes et al., 2011). Elevated blood viscosity may increase shear stress to the pre-damaged retinal vascular endothelial cells.
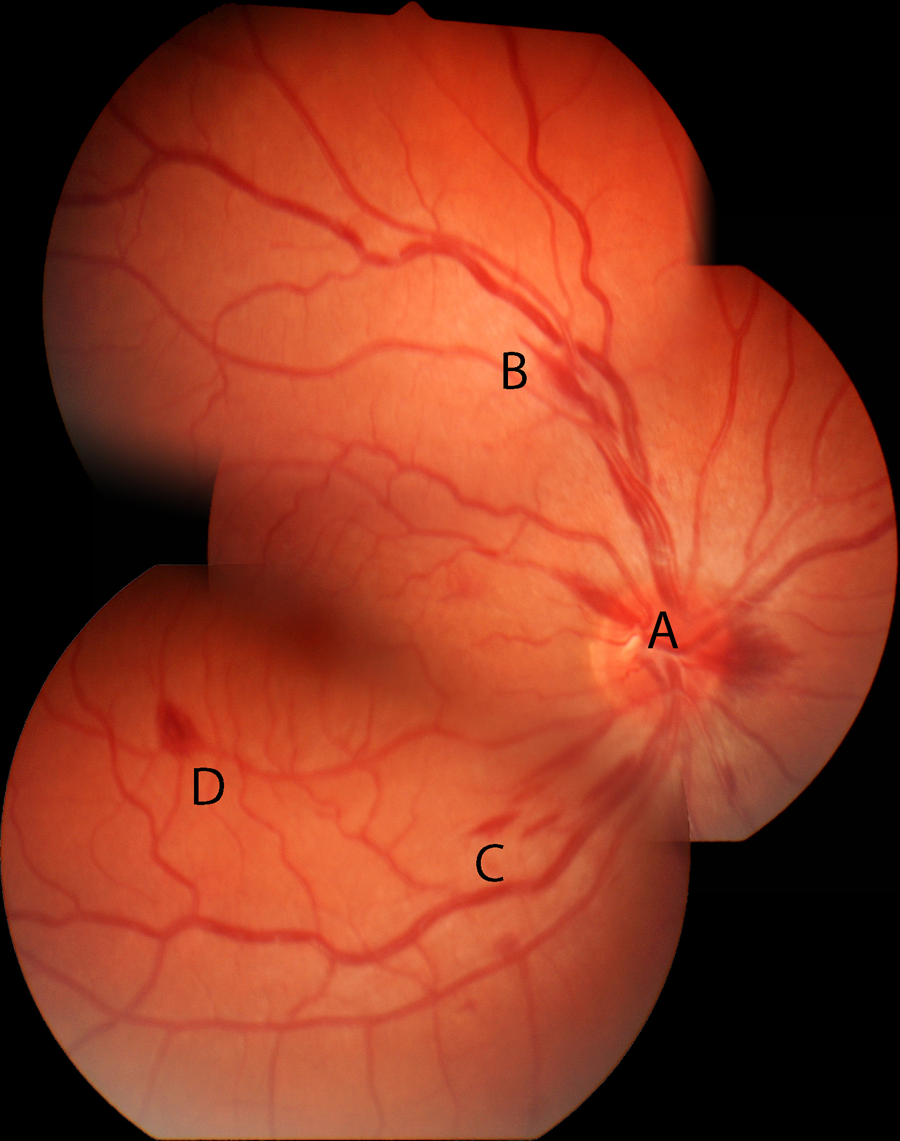
This fundus photograph shows the retina of a high altitude climber at 6870 m, who participated in the Muztagh Ata study in 2005. To be seen are
A subset of climbers show white-centered hemorrhages, also known as Roth spots (Roth, 1872). This specific type of bleeding observed at sea-level occurs in patients with capillary fragility due to systemic infections, hypertension, leukemia, diabetes (Rodriguez-Adrian et al., 2003), anemia, and leukemia, (Wechsler et al., 2004)—all of which may eventually result in capillary rupture (Ling and James, 1998). The white center of a Roth spot has been shown to represent a fibrin-platelet thrombus. Duane et al. (1980) described this white thrombus located at the site of a vessel rupture. Duane et al. (1980) and McFadden et al.(1981) reported Roth spots in climbers after exposure to high altitudes. High altitude climbers with Roth spots often present with larger retinal hemorrhages compared to climbers without white-centered hemorrhages (Barthelmes et al., 2011). This may be explained by distinct pathophysiological processes where climbers with Roth spots have undergone longer episodes of lower oxygen saturation during the climb (Barthelmes et al., 2011). This supports the hypothesis that hypoxic damage to retinal vessels at high altitudes can cause wall rupture after a certain time lag and then induce retinal bleeding, which is also an explanation for the above-mentioned white-centered hemorrhages (Ling and James, 1998).
Which Residual Problems Have Been Documented after HARH?
Similar to retinal hemorrhages occurring at sea level for various reasons, high altitude retinal hemorrhages usually disappear within days or a few weeks without sequelae. The large scale Muztagh Ata study found no persistent retinal pathologies 4.5 months after descent (Barthelmes et al., 2011). Other reports on HARH however mentioned residual problems as persistent scotomas (Shults and Swan, 1975; McFadden et al., 1981), vision loss after ischemic central retinal vein occlusion (Butler et al., 1992), and visual field shrinkage (Wiedman, 1975). It seems that in these cases, other pathologies (i.e., vessel occlusions) caused permanent damage rather than the hemorrhages themselves.
Incidence, Timing and Location of HARH
High altitude retinal hemorrhages can usually be seen ca. 3500 m above sea level (Hackett and Rennie, 1979; Honigman et al., 2001). Yet, to date, the exact incidence of high altitude retinal hemorrhages remains uncertain. The estimated incidence of HARH is reported to vary from 0% (Wiedman, 1975) to 79% (Barthelmes et al., 2011). Since many climbers with HARH do not experience visual disturbances, small hemorrhages, which appear and clear up during the course of the sojourn at high altitudes, may go unnoticed. Moreover, due to a time lag between reaching a certain altitude and occurrence of bleeding, diagnosis of HARH and identification of time of occurrence may only be established by systematic field examinations at different heights. It is of note that independent of the amount of hypoxia, a large number of retinal hemorrhages were detected shortly after descent from higher altitude, not during the ascent. That is, high altitude retinal hemorrhages mostly occur after the body has been subjected to the highest lack of oxygen to the tissue during the climb and not in a timely manner during or directly afterwards. Most entities of altitude-related illness occur at the highest reached altitude and regress after having reached lower altitudes. The vast majority of HARH were reported to be either near the optic disc or outside of the temporal retinal arteries (i.e., the macula remained unaffected). This explains the lack of symptoms during a climb in most mountaineers (Barthelmes et al., 2011).
Climbers, who sustain longer and more extensive systemic hypoxia during the expedition, present with more HARH (McFadden et al., 1981; Barthelmes et al., 2011). Also, the higher the ascent and the longer the duration at high altitudes, the higher the occurrence of retinal hemorrhages. Further studies have implicated that HARH may be seen more often in young and physically well-trained mountaineers—especially in those who undergo strenuous exercise at high altitudes (Brinchmann-Hansen et al., 1989; Arora et al., 2011)—such as in the report by Willmann et al. (2011) where mountaineers rapidly ascended to an altitude of 4559 m.
To date, there are no correlations between the incidence of high altitude retinal hemorrhages and medication such as diuretics or steroids shown in any of the very few high altitude studies considering this issue.
Which Signs and Symptoms of Altitude Illness Correlate with HAR or Only HARH?
Mountaineers affected by acute mountain sickness (AMS) suffer from a variety of nonspecific symptoms such as headache, nausea, insomnia, dizziness, lassitude, or fatigue (Roach et al., 1993). Some show a progression of symptoms eventually leading to high altitude cerebral edema (HACE), the end-stage of AMS. Hypoxia-induced increase in cerebral blood flow coupled with decreased integrity of the blood-brain barrier and cytotoxic edema are at the center of pathophysiological processes (Wilson et al., 2009). Signs of HACE are ataxia, altered consciousness, or both in a person with AMS. This condition is fatal if left untreated promptly and properly.
The cerebral signs of altitude illness are of interest from an ophthalmological point of view, since the eye is considered to be “the window to the brain”. Regulation of circulation of the brain has been reported to behave similarly to that of retinal vessels under hyper- and hypoxic conditions (Delaey and Van De Voorde 2000; Patton et al., 2005). It is hence possible that the pathophysiology of AMS, HACE, and retinal changes at high altitudes possess a common denominator. Studies on altered autoregulation of the cerebral blood flow (Jansen et al., 2002) and vasogenic cerebral edema (Hackett et al., 1998), possibly causing AMS and HACE, support this hypothesis.
Whether high altitude retinopathy shows a clear correlation with cerebral dysfunction at high altitude and thus may be utilized as a predicting sign, is still a matter of debate (Clarke and Duff, 1976; Wiedman and Tabin, 1999; Barthelmes et al., 2011; Willmann et al., 2011). Hence, we suggest to discuss HARH separately from optic disc swelling, which has been included in the current classification of high altitude retinopathy (Wiedman and Tabin, 1999).
Optic disc swelling has been reported to occur in up to 79% at altitudes of 4560 m (Willmann et al., 2011) and up to at least 59% of mountaineers at altitudes of 6800 m above sea level, increasing in incidence with ascent to higher altitudes and regressing quickly upon descent (Bosch et al., 2008). A correlation between optic disc swelling, peripheral oxygen saturation, and symptoms of acute mountain sickness has been reported in 27 climbers, concluding that optic disc swelling is most likely the result of hypoxia-induced brain volume increase (Bosch et al., 2008). On the other hand, Willman et al. (2011) did not find a correlation between optic disc swelling and symptoms of acute mountain sickness in 18 mountaineers. A possible explanation for this discrepancy is the different ascent profiles (rapid vs. slow) and the different heights reached in the two studies.
Both optic disc swelling and HARH are signs of overall susceptibility to hypoxia. But, the dynamics of HARH, as opposed to those of optic disc swelling, differ as there is a delay in appearance and a slower regression of changes in the posterior segment. Clarke and Duff (1976) questioned whether the appearance of isolated retinal hemorrhages should be considered a warning sign of impending cerebral edema. Another study also could not find a correlation between HARH and cerebral symptoms (Barthelmes et al., 2011). Wiedman and Tabin (1999), on the other hand, indicated a possible association between HAR and HACE in their work.
Recommendations
What to do on a trip to high altitude if someone has symptoms/findings suggestive of HAR?
Symptomatic bleeding in the eye suggests either the occurrence of hemorrhages within the macula or a spillover into the vitreous, both of which may impair vision markedly. If the climber is unfortunate enough to have bilateral hemorrhages close to the foveolar region, he or she will have to descend (with help) since resorption of the blood will take days to weeks, depending on the hemorrhage. If visual disturbances do not resolve within a week, the climber should seek consultation by an ophthalmologist within maximally another week. Since there is no clear evidence that retinal hemorrhages are warning signs of impending severe acute mountain sickness or even high altitude cerebral edema, continuation of the expedition can be ventured—under the premise that the climber is never alone during the further sojourn at high altitudes—and only in case visual disturbances due to retinal bleeding are minimal and do not impede the safety of the climb. As soon as scotomas occur in both eyes, it is prudent to descend immediately and accompanied.
Can people with prior symptomatic retinal hemorrhages go back to high altitude? Which guidelines should be followed?
Since HARH are of transient nature, we would not go as far as to discourage climbers who have experienced prior symptomatic retinal hemorrhages from going back to high altitude.
To date there is no medication that has been reported to prevent retinal hemorrhages. However, studies on high altitude related diseases are often performed in healthy mountaineers who are not on regular medication. Medication such as nonsteroidal anti-inflammatory drugs, corticosteroids, and acetazolamide, were shown to have no impact on retinal bleeding in the Muztagh Ata study (Barthelmes et al., 2011).
Future Directions
Further studies with large cohorts and similar ascent profiles should be pursued in the future in order to find answers to current discrepancies in hypotheses concerning the pathophysiology of HARH and their association to signs and symptoms of altitude sickness. More data on the development of retinal hemorrhages, also in context with optic disc swelling, is needed. Grading of high altitude retinopathy could be extended to include the fact that changes to the optic disc due to hypoxia occur more quickly than retinal hemorrhages during the same hypoxic event. Severity of HAR during a climb might be defined by emphasizing the appearance of the optic disc, whereas overall severity after the climb could include the extent of HARH.
The lack of data regarding how many climbers with preexisting medical problems develop high altitude retinal hemorrhages or whether certain drugs can induce HARH makes it difficult to develop concise management guidelines. Further data should be collected on healthy mountaineers taking medication at high altitudes. Thus, the above-mentioned recommendations should be considered with caution.
Footnotes
Author Disclosure Statement
The authors have no competing interests or financial ties to disclose.