
Abstract
Abstract
Ginosar, Yehuda, Atul Malhotra, and Eli Schwartz. High altitude, continuous positive airway pressure, and obstructive sleep apnea: Subjective observations and objective data. High Alt Med Biol 14:186–189, 2013.—We report observations made by one of the authors who ascended to the Thorang La pass (5416 m) in the Nepal Himalaya in October 2010, despite moderate-severe obstructive sleep apnea. We report the first recorded use of nasal CPAP to treat high altitude pulmonary edema (progressively severe dyspnea at rest and severe orthopnea, with tachycardia and tachypnea) that occurred at 4400 meters, when snow and darkness made safe evacuation difficult. We also present objective longitudinal data of the effects of altitude on auto-adjusting CPAP delivered via a portable nasal CPAP device, and on the apnea hypopnea index measured during sleep while using the device. OSA may be a risk factor for the development of high altitude pulmonary edema and we suggest that a nasal CPAP device located in high altitude trekking stations may provide an additional or alternative treatment option for managing high altitude pulmonary edema until evacuation is possible.
Introduction
Subjective Observations (YG)
I am a healthy male anesthesiologist; at the time of the trek I was 48 years of age, height 179 cm, weight 76 kg, BMI 23.7 kg/m2, nonsmoker, taking regular exercise. Fifteen months prior to the trek, I was diagnosed with moderate-severe obstructive sleep apnea (OSA) based on a long-standing history of snoring, poor sleep quality, daytime somnolence, and positive polysomnograph findings (98% oxygen saturation on room air, snoring volume 68 decibels; apnea-hypopnea index (AHI) 28.4/h, apneic episodes lasting up to 40 sec with desaturation to 85%). Sleep quality improved with auto-adjusting nasal CPAP (auto-adjusting CPAP device: AutoSet Spirit II; nasal mask: Mirage Swift II; both from Resmed Ltd, Bella Vista, NSW, Australia).
There is now electricity in every village on the popular Annapurna trail (Table 1), although there are typically no electricity points in rooms in roadside lodges. Having failed to find a battery pack for my CPAP device, I connected it either to the central power supply or rewired it from a light socket in the bedroom. There were two nights when no electricity was available (Chame 2670 m and Yak Kharka 4050 m); on those occasions I was extremely symptomatic from what I assumed to be OSA (repeated reawakening with a sensation of gasping, despite attempting to sleep sitting upright). The latter of these two nights without CPAP was followed by the development of symptoms attributed to high altitude pulmonary edema (HAPE) the next day (see below). The last night was spent at Thorung Pedi at 4400 m. Ascent rate was below 300 m/day to allow acclimatization and included three continuous nights at Bhraga (3450 m) with daytime treks to higher elevations. Up to this stage, I was asymptomatic, apart from diuresis and mild tachypnea, which are normal physiological adaptations to altitude. Four hours after arrival at Thorung Pedi, I became mildly dyspneic on moderate exercise and took a first dose of 250 mg acetazolamide and rested. Dyspnea worsened progressively over the next 4 hours, to severe dyspnea at rest, severe orthopnea that made lying flat impossible, and eventually marked dyspnea sitting up. There was a marked subjective sensation of tightness in the chest, with tachycardia and tachypnea. Although I was able to speak clearly, it made me breathless. I did not have a pulse oximeter, and the light was too poor to determine my color. My fellow travelers were not medically trained but they attested to the fact that I was calm and rational and was apparently not having an anxiety-hyperventilation attack. Although I had no cough, gurgling breathing, or pink frothy sputum, it was clear that this met diagnostic criteria for HAPE.
1
There is broad consensus that the most important treatment for HAPE is to descend at least 300 m urgently, day or night.
2
By this time however, it was pitch black and snowing. In light of my breathlessness, we felt that evacuation by foot was impossible, and that evacuation by horse or helicopter was dangerous in the poor visibility. I took a second dose of 250 mg acetazolamide and applied CPAP sitting upright in bed. By 1 h, breathing became easier and eventually I was able to sleep sitting up for about 3 h. In the morning (3:30
Villages with no electricity during the trek; **Site of HAPE described in the text.
Objective Data
On return home we analyzed the data from the CPAP device. We present the average and 95th percentile auto-adjusting CPAP levels (Fig. 1) and the average measured AHI (Fig. 2) obtained for each calendar day of the trek, including baseline days in Pokhara before and after the trek. The longitudinal data present a clear picture of progressive effects of altitude on both of these parameters, and when compared with baseline (827 m), high altitude (4400 m) was associated with an almost two-fold increase in the measured auto-adjusting CPAP level and an almost five-fold increase in the AHI.
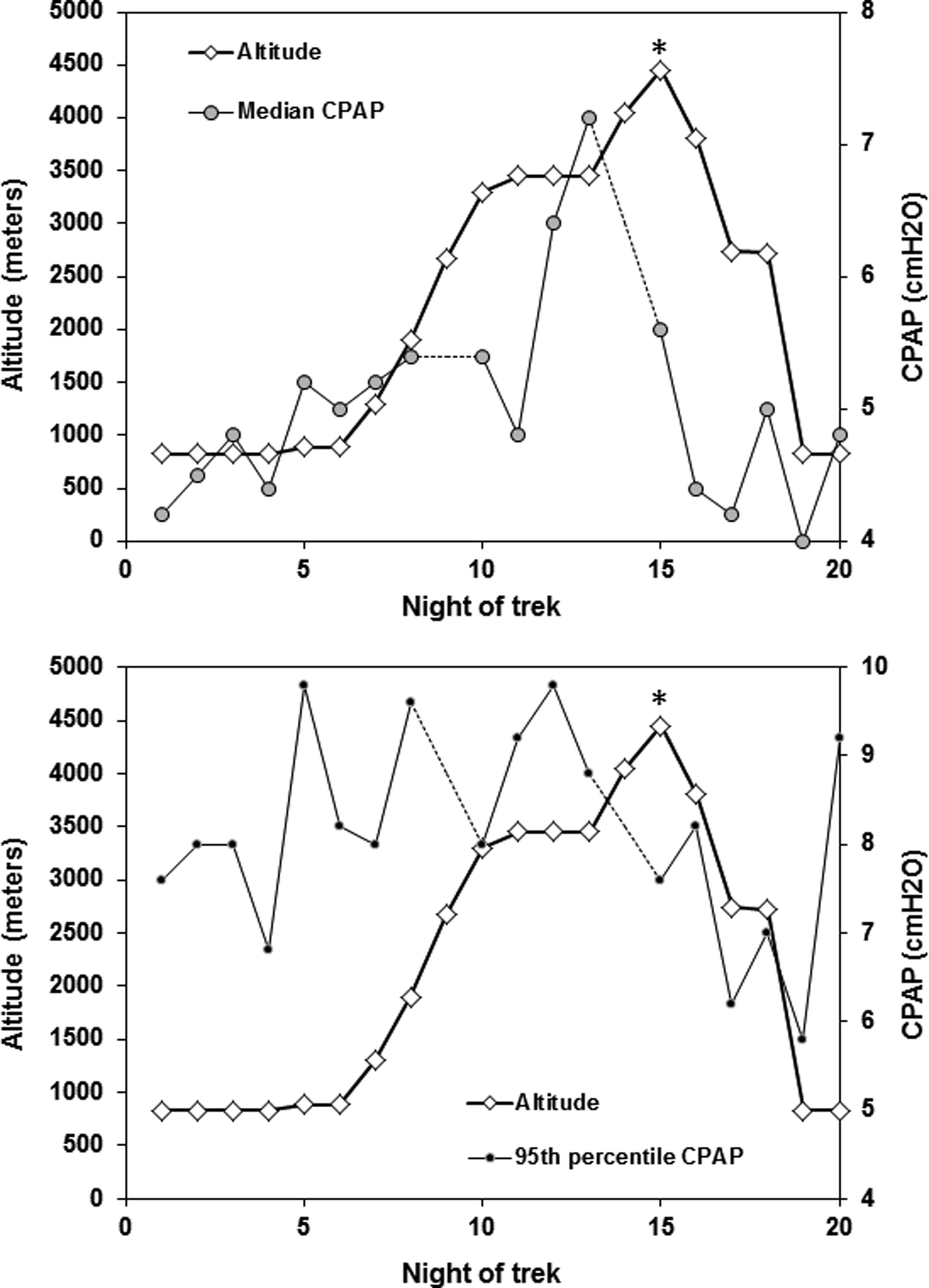
The effect of change in altitude on (
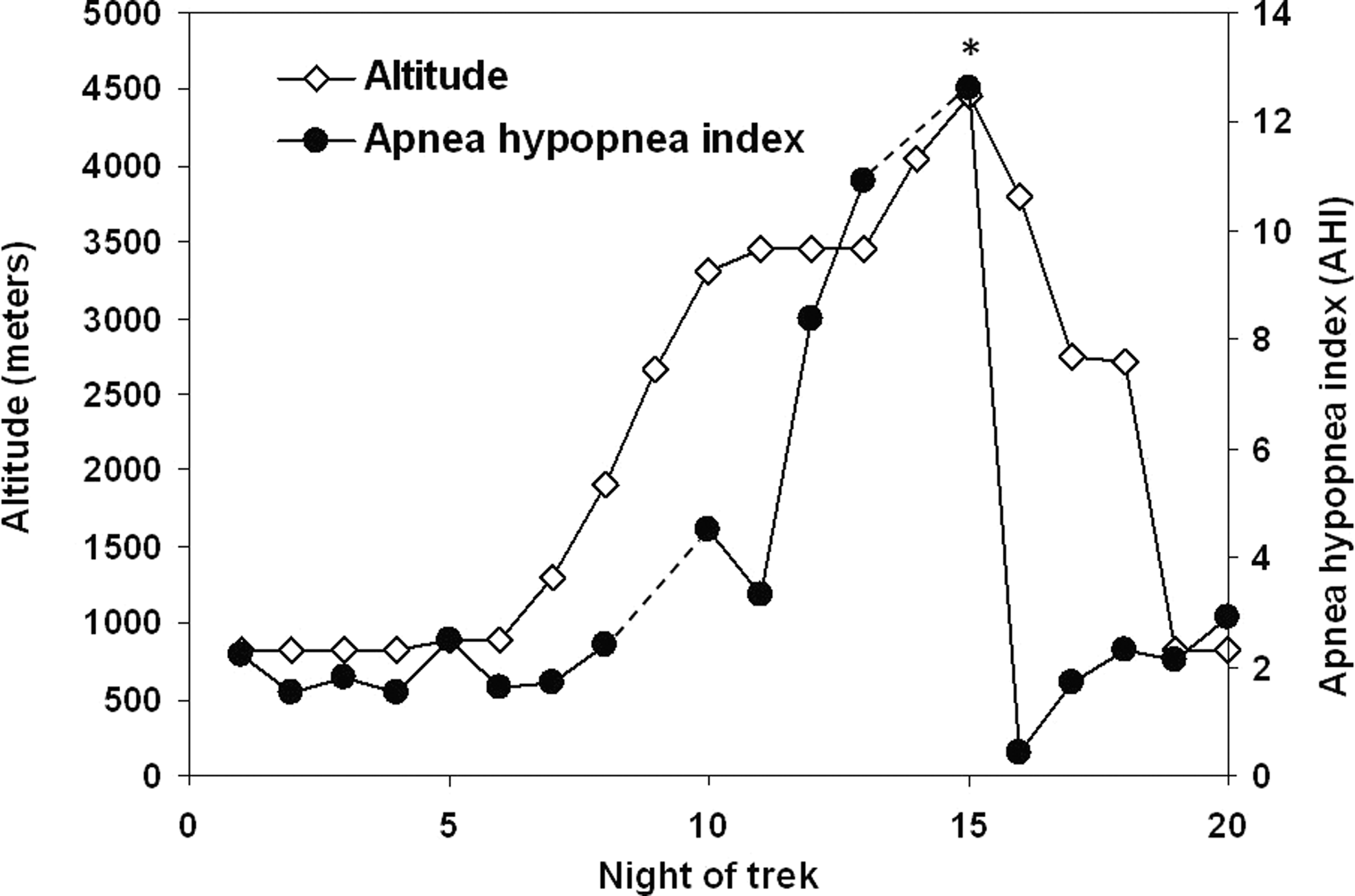
The effect of change in altitude on the apnea-hypopnea index (AHI). See text for details; see Table 1 for details of villages. Breaks in lines represent nights with no electricity; *represents night of HAPE symptoms. Note: The CPAP device used in this study was not able to distinguish between central and obstructive apneic episodes.
Discussion
Increasing altitude causes a progressive reduction in the barometric pressure and partial pressure of oxygen, with well-described ventilatory responses that are modified by acclimatization. 3
Acute mountain sickness (AMS) is associated with rapid ascent above 2500 m that does not provide sufficient time for acclimatization (typically in excess of 300 m per day); 2 it usually occurs progressively and includes a wide spectrum of neurological and respiratory complaints.1,2 The described case meets diagnostic criteria for HAPE that is based on any two of the following symptoms: dyspnea at rest, cough, weakness/decreased exercise performance, chest tightness or congestion; and any two of the following signs: rales or wheezing, central cyanosis, tachypnea, tachycardia. 1
The cause of HAPE is less clearly understood than other causes of pulmonary edema 4 . It is likely related to a nonuniform response to hypoxia; in some lung regions, hypoxic pulmonary vasoconstriction predominates with reduced pulmonary flow (dead space), while in neighboring less vasoconstricted regions, increased pulmonary hydrostatic pressure predominates, with pulmonary edema (right-to-left shunt); this may explain the exacerbation of HAPE after exercise. 4 Chronic untreated OSA is associated with mild to moderate pulmonary hypertension due to the effects of chronic intermittent hypoxemia 5 and an increased susceptibility to hypoxic pulmonary vasoconstriction; both may contribute further to HAPE in OSA.
Although a recent study found no effect of a change in altitude on the CPAP levels required in auto-adjusting CPAP devices, 6 that study only assessed the effects of decreasing altitude as high altitude dwellers traveled to sea-level. Another recent study 7 assessed the effects of increased altitude from baseline 490 m, with 2 nights each at 1860 m and 2590 m. Although there was a reduction in nocturnal oxygen saturation (94%, 90%, 86–87%, respectively), all patients ascended to altitude without CPAP, despite being CPAP dependant at baseline. In our report we assessed the longitudinal effects of acute changes in altitude from 820 m to 4400 m on CPAP levels and apneic/hypopneic episodes, while continuing to use CPAP. Although our report is based on one subject, objective longitudinal data over multiple data points appears to suggest a deleterious effect of acute increases in altitude on severity of sleep disordered breathing in this subject. The mean auto-adjusted CPAP level increased two-fold (although the 95th percentile CPAP did not change consistently during the most symptomatic period), the apnea/hypopnea index increased five-fold and the trek was complicated by HAPE.
The CPAP device used in this study was not able to distinguish between central and obstructive apneic episodes, and it is possible that the median CPAP level may be more sensitive to central apnea than the 95th percentile CPAP level. Furthermore, this device adjusts CPAP in response to apnea, snoring, and flow limitation. HAPE is likely to affect these factors that determine CPAP further, both due to reduced lung compliance and perhaps due to flow turbulence caused by rapid, shallow breathing. Unstable ventilatory control is known to be a factor underlying the pathogenesis of OSA, such that alveolar hypoxia would be predicted to induce periodic breathing in predisposed individuals.8–10
Previous reports would suggest that the increased apneic episodes were more likely attributable to central than obstructive apnea. In a study of 14 trekkers hiking from 1400 m to 5000 m, the central respiratory disturbance index increased progressively from 0/h to 56/h, while obstructive apneic/hypopneic index reduced over the same period from 11/h to 2/h. 11 Similar observations were made by the same investigators in a group of five patients with moderate OSA at simulated altitude. The AHI due to obstructive apnea at 60 m, 610 m, and 2750 m was 25.5, 17.3, and 0.5, respectively; the AHI from central apnea was 0.38, 8.1, and 78.8, respectively at the same altitudes. 12
In this report we describe a presumptive diagnosis of HAPE and its successful treatment with nasal CPAP. Additionally, we present longitudinal data to suggest that increasing altitude was associated with 1) a progressive increase in auto-adjusted CPAP, and 2) a progressive marked increase in the number of apneic and hypopneic episodes occurring during nasal CPAP use. In recent guidelines for prevention and treatment of acute mountain sickness, CPAP was suggested as a possible adjunct to supplemental oxygen in the hospital setting,
3
but its use has rarely been described in treating HAPE in the field. A blow-bottle positive pressure system was proposed to provide variable PEEP for high altitude, but was not tested on clinical HAPE patients.
13
A tight fitting face mask with spring-loaded expiratory resistors (5 cmH2O and 10 cmH2O) were used to treat patients with HAPE under controlled conditions in the Mt McKinley research facility (4400 m).14,15 Oxygen saturation14,15 and tidal volume
15
progressively increased, respiratory rate progressively decreased, and minute ventilation was unchanged.
15
Finally, a CPAP helmet providing 15 cmH20 CPAP improved Sp
Footnotes
Acknowledgments
YG made the trek, recorded the subjective observations and objective data and wrote the manuscript. AM and ES gave pre-trek consultations and made substantive changes to the manuscript and approved the final version. The authors gratefully acknowledge the assistance of Mr. David Gazi from Cleanetica (Israel) for downloading data from the Resmed CPAP device. YG gratefully acknowledges the assistance at Thorang Phedi of Nurit, Hillel, Bracha, and (last but not least) the horse.
Author Disclosure Statement
No competing financial interests exist.