
Abstract
Abstract
Patz, David S., Michael D. Patz, and Peter H. Hackett. Dead space mask eliminates central apnea at altitude. High Alt Med Biol 14:168–174, 2013.—Travelers to high altitude may have disturbed sleep due to periodic breathing with frequent central apneas. We tested whether a mask with added dead space could reduce the central apneas of altitude. 16 subjects were recruited, age 18–35, residing at 4600 ft (1400 m). They each slept one night with full polysomnographic monitoring, including end tidal CO2, in a normobaric hypoxia tent simulating 12,000 ft. (3658 m) altitude. Those who had a central apnea index (CAI) >20/h returned for a night in the tent for dead space titration, during which they slept with increasing amounts of dead space, aiming for a CAI <5/h or <10% of baseline. Then each subject slept another night with the titrated amount of dead space. Of the 16 subjects, 5 had a central apnea index >20/h mean 49.1, range 21.4–131.5/hr. In each of the 5, the dead space mask reduced the CAI by at least 88% to a mean of 3.1, range 0.9–7.1/h, (p=0.04). Hypopnea index was unchanged. Three subjects required 500 cc of dead space or less. One subject required 860 cc, and one required 2.1 L. Morning symptoms and arousal index were not significantly affected by the dead space mask. Dead space did not appear to increase the CO2 reserve. At 12,000 ft., central apneas can be effectively reduced with a dead space mask, but clinical utility will require further evaluation.
Introduction
Another strategy to reduce CSA is to add carbon dioxide (CO2) to inspired air. Pembrey and Allen (1905) first showed that breathing air with a mixture of CO2 stabilized periodic breathing in Cheyne-Stokes respirations at low altitude. Many decades later, Bersenbrugge et al. (1983) found that CO2 by nasal cannula suppressed the central apnea of hypoxia/altitude. Xie et al (1997) subsequently used a dead space mask that allowed some rebreathing of exhaled air to treat patients with idiopathic central sleep apnea. Khayat et al. (2003) similarly used an adapted CPAP nasal-oral mask with added dead space to reduce central sleep apnea in patients with heart failure. Knowing that nasal CO2 suppresses CSA at altitude, and that a dead space mask suppresses CSA in other settings, we evaluated whether a mask with added dead space (no CPAP machinery) suppresses central apnea of high altitude, and attempted to record its impact on symptoms and mechanism of effect.
Methods
Recruitment
Sixteen healthy volunteer subjects without symptoms of obstructive sleep apnea or prior mountain sickness, living at 4600 ft (1400 m), ages 18–35 years, were recruited by newspaper advertisement to participate in the study. They signed informed consent overseen by the St. Mary's Hospital investigational review board (protocol #2010-004).
Protocol
Each of the 16 subjects had a full night attended polysomnogram in Grand Junction, Colorado (4600 ft, 1400 m) inside a normobaric hypoxia tent, with FiO2 kept at 15.6±0.3% to simulate 12,000 feet (3658 m). Subjects with a central apnea index (CAI) greater than 20/h were invited back for further studies with dead space intervention. At least 1 week elapsed between studies for each subject in order to minimize effects of acclimatization. Each returning subject had one night of “dead space titration,” sleeping 1–2 h with increasing amounts of dead space: 110 cc, 360 cc, 440 cc, or 610 cc. Two of the five returning subjects required an additional night of titration, needing more than 610 cc of dead space. The subjects were then observed a full night, or, in one subject, 4 h, with the dead space volume determined sufficient to drop their CAI below five events per hour, or to less than 10% of their baseline CAI. The purpose of this third night was to assess the effect of the dead space mask on symptoms. One subject repeated his titration process an extra night with a pneumotachometer (Braebon 0551 Ultima flow sensor with 0310 pneumotach, Kanata, Canada) in line between the mask and the dead space to assess the increased minute ventilation required by various amounts of dead space. Minute ventilation at each dead space amount was measured for 5 min when periodic breathing was absent.
Polysomnography
Polysomnography was performed and scored according to American Academy of Sleep Medicine standards (Iber et al., 2007) with Alice 5 Sleepware (Philips Respironics, Murray, PA). End-tidal CO2 (ETCO2) was monitored with a Nonin RespSense (Plymouth, MN). The scoring sleep technologist used definition 4A for hypopnea, requiring 4% O2 desaturation, and was blinded regarding mask vs. no mask. Thermistry, nasal ETC02, and flow monitoring continued under the mask when dead space was added.
CO2 measures
Average eupneic end-tidal CO2 was obtained by picking a 5-min period approximately hourly when breathing was not cyclic with apneas or hypopneas. The lowest and highest digital end-tidal CO2 reading each minute through this 5 min period was recorded for six to eight 5-min periods through the night. These 60 to 80 numbers were averaged for the eupneic end-tidal CO2.
Apnea threshold (AT) is the P
CO2 reserve was defined as the difference between the average eupneic end tidal CO2 and the average apnea threshold (CO2 reserve=eupneic CO2 - AT) (Dempsey et al., 2004). All measures of apnea threshold and eupneic end-tidal CO2 were made in non-REM sleep.
Symptom measures
Each morning after a night in the altitude tent (Colorado Altitude Training, Boulder, CO), the subjects completed an Environmental Symptoms Questionnaire (ESQ) (Sampson et al., 1980) and a Lake Louise Symptom Score for acute mountain sickness (AMS) evaluation (Maggiorini et al., 1998).
Mask
We initially used a medium Quattro mask, with the safety flap removed and all leak holes taped shut, so that breathing was through the channel normally connecting to the CPAP hose. This provided 110 cc of dead space. Further dead space was added initially by using an Arrowhead water bottle whose top fit precisely over the exit of the Quattro mask. A 2-inch (5.1 cm) diameter hole was cut into the bottom of each water bottle, opening airflow to the environment. We used bottles 250 cc, 330 cc, and 500 cc in size.
Part way through the study, with subjects complaining of the resistance with breathing, the mask design was changed. We placed a 2-inch diameter hole in the front of the Quattro mask, with a short plastic 2-inch (5.1 cm) diameter cylinder running through the hole to allow plastic cups of various sizes (250 cc, 330 cc, 500 cc, and for one subject 750 cc.) to be attached (Fig. 1). One subject required more dead space, and a 1 L, then 1.5 L, then 2 L improvised plastic/cardboard arrangement was attached to the 2-inch plastic cylinder. One of the five subjects with a high frequency of central apnea, used the original style mask through his full night with dead space. The other four subjects with frequent central apneas used the second mask style, to evaluate their full night with the determined amount of dead space.

Initial and final mask styles. Initial mask design (left) required breathing through the narrow CPAP mask channel, 0.75 inches (1.9 cm). Final mask design (middle and right) eliminated airflow resistance with a minimum airflow channel diameter of 2 inches (5 cm).
Statistical analysis
An unpaired, two-tailed Student's t test was used to calculate p values comparing the group of 11 subjects who had few central apneas to the group of 5 subjects with frequent central apneas. A paired, two-tailed Student's t test was used to assess the 5 subjects who used the dead space mask, comparing respiratory values and symptom values without the mask to values of the full night with the mask. A paired, single-tailed Student's t test compared the central apnea index without and with dead space, since this value was intentionally titrated in one direction, downward. Values in the text and tables are average±1 standard deviation. In Figure 4 they are displayed as averages with bars indicating 1 standard error from the mean.
Results
Sixteen subjects were recruited, including 5 women, with ages ranging from 18–35, average 23.1 years. Average body mass index was 23.1±4.9, range 16.9 to 36.1. Average values for all variables are listed in Table 1.
Columns 1 and 3 compare averaged data from the 11 subjects with few central apneas, to the 5 subjects with over 20 central apneas per hour at altitude. P values between these columns relate to this comparison. Columns 3 and 5 compare averaged data in the 5 subjects with frequent CAs without dead space to their data with the optimal dead space added; the P values between these columns relate to this comparison. AHI, apnea hypopnea index; AM, morning; AMS, acute mountain sickness; BMI, body mass index; CA, central apnea; ESQ, environmental symptom questionnaire; Thresh, threshold.
Baseline altitude studies
Hypopneas and central apneas were the two predominant respiratory events in this group of healthy subjects at simulated altitude. Of 16 subjects, 5 had central apnea indices greater than 20 events per hour, range 21.4 to 131.5/h. The other 11 had central apnea indices less than 20 per hour, range 0.3 to 10.6/h. The hypopnea index (HI) was similar in both groups. Obstructive apnea index was less than 1/h and respiratory effort-related arousal index was less than or equal to 4/h in all 16 subjects in all studies. Comparing the group of 5 with high-frequency central apnea to the 11 with low-frequency central apnea, the average Sa
Dead space titrations
In the 5 subjects with frequent central apnea at altitude, the dead space volume required to reduce CAI below 5/h or below 10% of baseline varied significantly. 440 cc of dead space was adequate for 3 of the 5. One subject required 860 cc of dead space. The subject with the highest central apnea index, 131.5/h, required 2110 cc of dead space to significantly reduce central apnea at altitude. Figure 2 shows the hypnogram of an example titration.
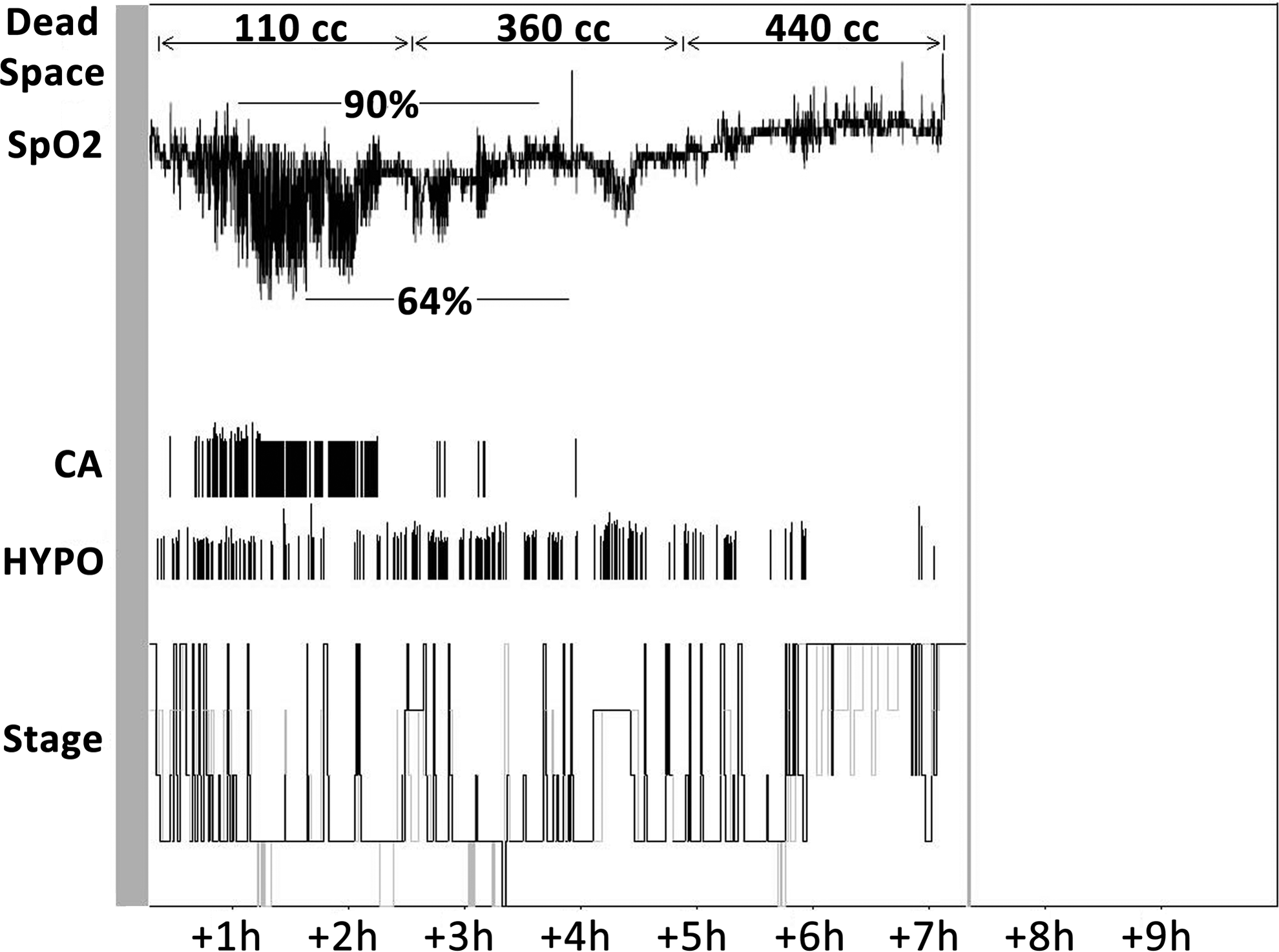
Hypnogram from one subject's dead space titration night at altitude. Note central apneas decreasing with increased dead space.
Baseline study vs. night with final dead space amount
Table 1 lists the average values comparing the untreated night at altitude to the night at altitude with the determined dead space amount in the 5 subjects with frequent central apnea. The apnea hypopnea index (AHI) and the central apnea index markedly decreased, while the hypopnea index was unchanged by the addition of dead space (Figs. 3 and 4). Average non-REM Sa
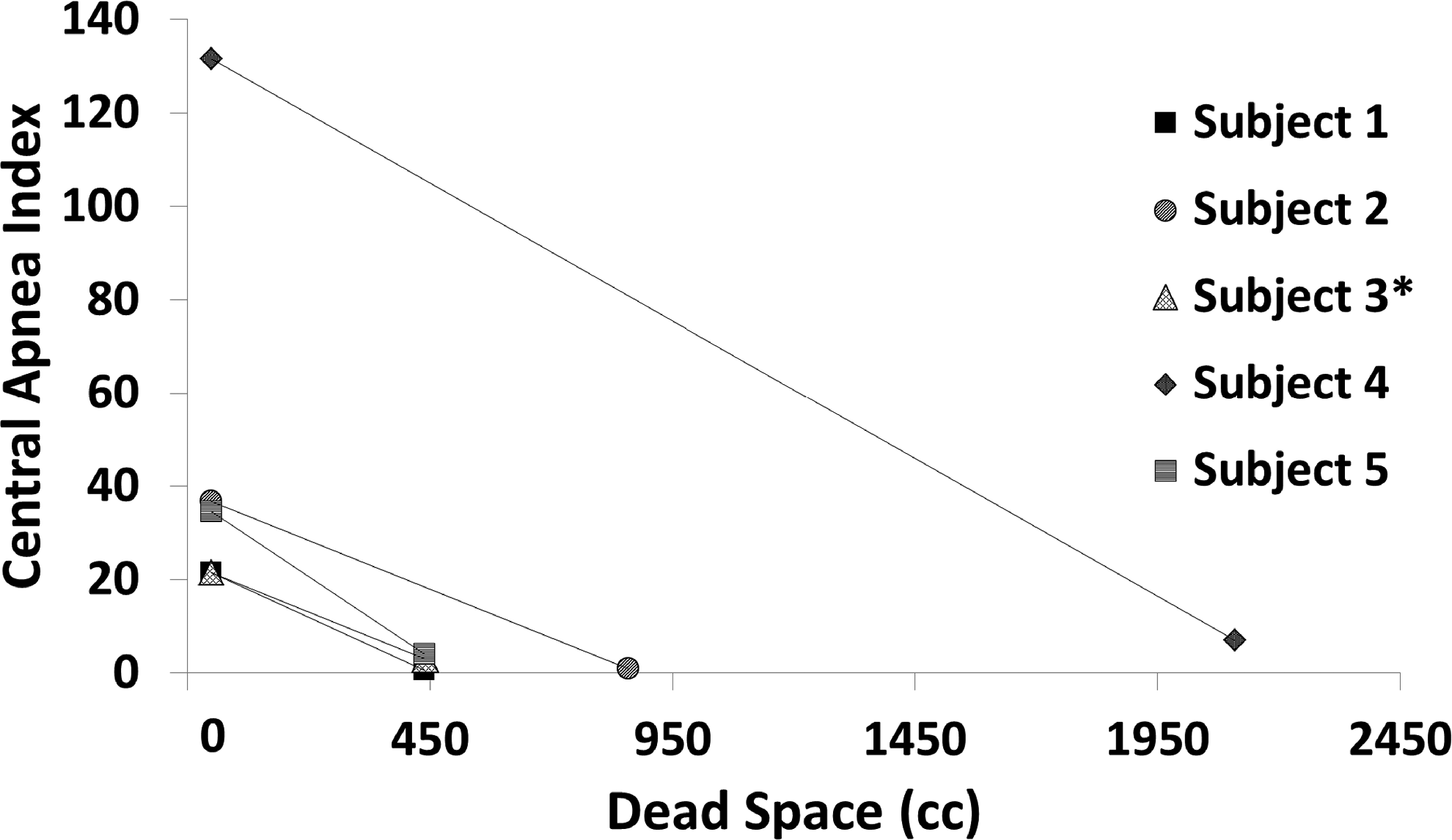
Central apnea index at 12,000 ft (3658 m) without and with dead space in 5 subjects: central apnea index at altitude dropped by 88% or more in each of 5 individuals when sufficient dead space was added. Amount of dead space required is reflected by X-axis location of lower point. *Subject 3 used the initial mask style.
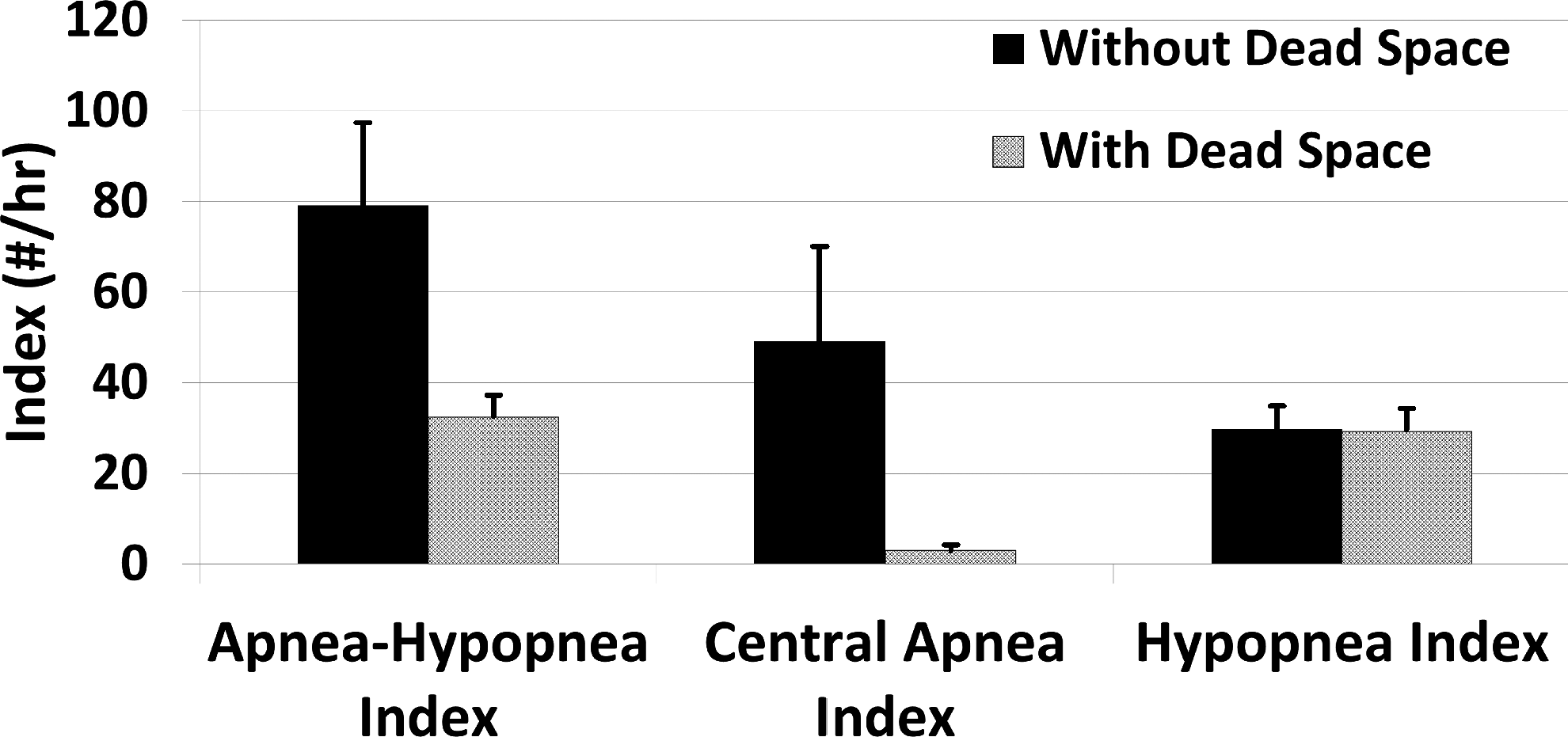
Respiratory event indices in 5 subjects at 12,000 ft (3658 m) without and with dead space mask. Apnea hypopnea index dropped significantly with dead space mask, due to significant reduction in central apnea index. Hypopnea index remained unchanged.
The subject with a central apnea index of 131/h had no periods of eupneic non-REM sleep, so eupneic end-tidal CO2 and CO2 reserve values were unavailable from his initial night without dead space. Regarding CO2 measures without vs. with dead space in the other four with frequent central apnea, end tidal CO2 increased with dead space. Since the apnea threshold also increased with dead space, the average CO2 reserve remained unchanged (Table 1).
Regarding symptoms, these five subjects scored slightly worse with the addition of dead space at altitude, with both the Lake Louise AMS score and the ESQ score. However, in the five subjects, symptoms were minimal and the only headache to develop overnight was on a night without the mask. Arousal index was not significantly affected by the mask (Table 1).
One subject slept with the pneumotachometer in line between the 110 cc mask and the dead space, with increasing volume of added dead space beyond the mask of 0 cc, 250 cc, 330 cc, and 500 cc. To fit the pneumotachometer in line, the initial unaltered Quattro narrow channel mask was used, along with the Arrowhead water bottles. The following trends were noted with increasing dead space: increased minute ventilation, end-tidal CO2, and apnea threshold, and decreased central apnea index. CO2 reserve did not increase (Table 2 and Fig. 5).
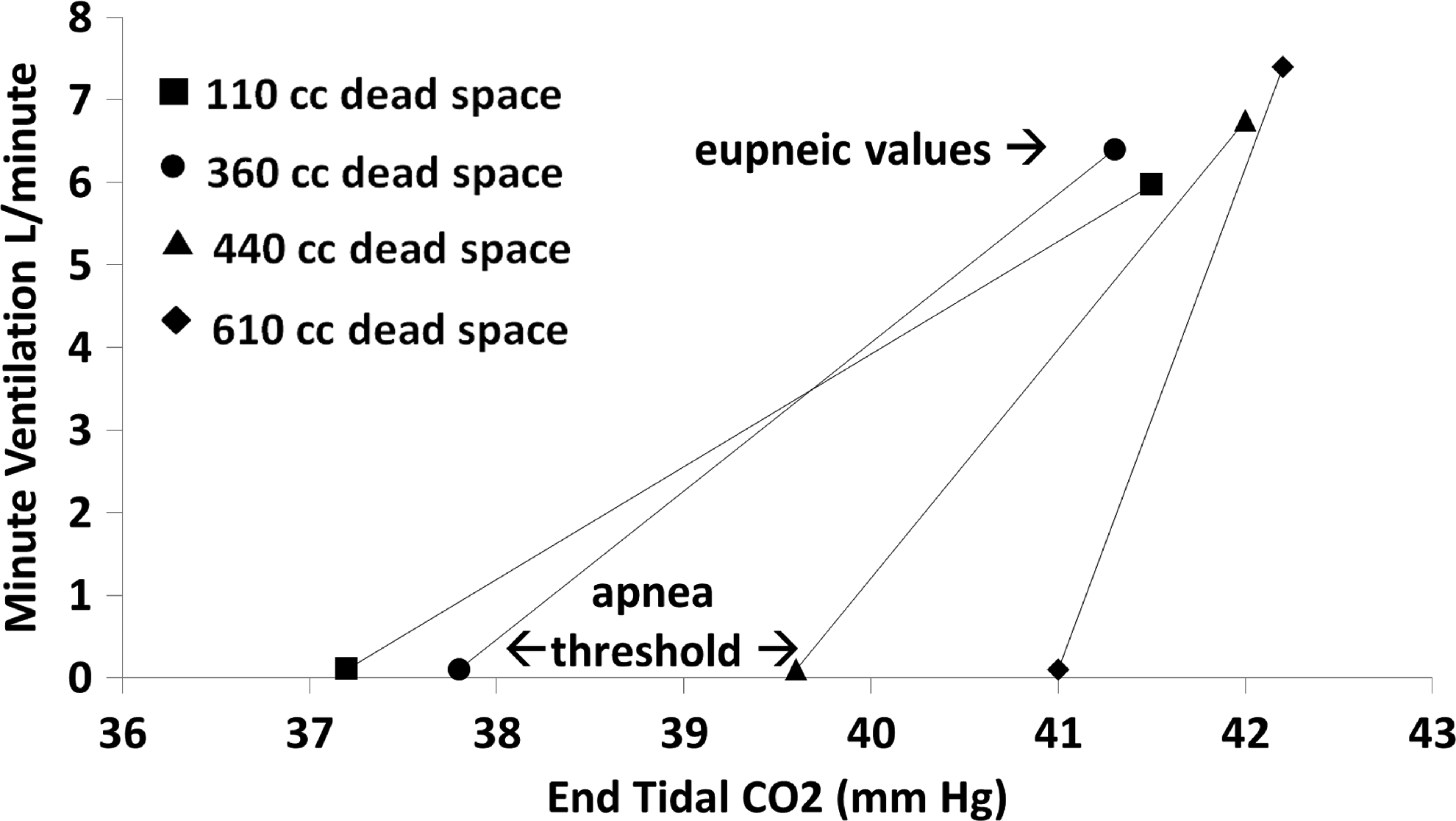
Eupneic end-tidal CO2 and eupneic minute ventilation and apnea threshold in one subject at 12,000 ft (3658 m) with 4 different amounts of dead space. Note that apnea threshold and eupneic end-tidal CO2 both increase with increasing dead space. Table 2 includes the same data numerically.
This subject was monitored with the pnuemotachometer. CO2 data are displayed in Figure 5.
Discussion
We found that in each of five subjects with significant central apnea at simulated altitude, a mask with added dead space reduced central apnea index by 88% or more.
The addition of dead space did not aggravate hypoxemia, likely due to increased minute ventilation, as observed in the one subject whose minute ventilation was monitored through a dead space titration.
The finding of reduced AHI is consistent with Lovis, who also recently studied the use of dead space at altitude. His five subjects with AHI >30 all had significant reduction in AHI (Lovis et al., 2012). Our suspicion, similar to Lovis, was that dead space would stabilize periodic breathing by raising P
There is disagreement in the literature regarding whether periodic breathing plays a role in acute mountains sickness. Nussbaumer-Oschner recently studied the course of central apnea at 4559 m, and over the first three nights central apnea continued at the same frequency, while symptoms of acute mountain sickness improved (Nussbaumer-Oschner et al., 2012). Their findings suggest a lack of relationship of central sleep apnea to symptoms of acute mountain sickness. Erba et al. (2004) found that subjects at 4559 m who remained well and those who subsequently developed acute mountain sickness had similar apnea hypopnea indices. These studies provide less optimism that reducing central apnea at altitude could reduce AMS symptoms.
It is not clear that eliminating periodic breathing at altitude is an advantage. One of the consequences of periodic breathing at altitude is accentuating intermittent hypoxemia at night. Intermittent hypoxemia leads to increased reactive oxygen species and production of prostaglandins in the carotid body, perhaps further increasing the hypoxic ventilatory response (HVR) (Iturriaga et al., 2005). Increasing HVR is an important part of acclimatizing to altitude and maximizing Sa
On the other hand, there may be benefits reducing the oscillating intermittent hypoxemia (IH) during sleep at altitude. While perhaps slightly reducing the hypoxic ventilatory response of the carotid body, reduction in IH may also reduce detrimental high sympathetic output. And, since hypoxemia is the main cause of AMS and high altitude pulmonary and cerebral edema, blunting the lowest Sa
To determine whether a dead space mask could be useful for decreasing insomnia, fatigue, AMS, or mood and cognition changes at altitude (Lemos et al., 2012) would, as Lovis concluded, require a large cohort and longer duration of successive nights at altitude (Lovis et al., 2012). Perhaps some of the arousals and complaints of poor sleep using the mask were discomfort related and would be expected to decrease with successive nights. Whether to pursue this possible nonpharmacologic alternative to acetazolamide is unclear. Some of our subjects in the morning, when asked, stated they would rather take a pill than wear the mask at night. The dead space mask may prove to have a role as an alternative for the subjects with known periodic breathing at altitude, unwilling to take acetazolamide, or unable to, due to allergy or side effects (Kayser et al., 2012). However, importantly, average Sa
Limitations
1. The ability to determine “apnea threshold” in the midst of periodic breathing may be less accurate than during controlled ventilation, where it is gradually approached, as in the first studies by Dempsey et al. (2004). During periodic breathing, Sa

Oscillations in arousal state and SaO2 may affect apnea threshold. A 30-second epoch from a subject during repetitive central apneas. Note the arousal during the three breaths in between the apneas.
In addition, circulatory delay from the pulmonary capillaries to the peripheral and central chemoreceptors adds a conceptual problem with the validity of our measurement of apnea threshold. The decision not to take the next breath is probably being made 6 to 15 seconds before blood with P
2. The different mask styles. In the first style, breathing through the narrow CPAP mask outlet may have added a resistive load to breathing, which could have an effect both of increasing P
Conclusions
A mask with dead space added can effectively reduce central sleep apnea at simulated altitude. The mechanism of effect is not clearly determined, and may be multifactorial. However, in this small group of subjects, using the mask for a single night did not ameliorate symptoms. The dead space mask may be a promising way to reduce periodic breathing at altitude and possibly improve symptoms due to periodic breathing, but in view of potentially delaying acclimatization, use of this device for travelers and climbers should await further studies.
Footnotes
Acknowledgments
Special thanks are given to Mark Spoon and Gary Steiner, the sleep technologists acquiring and scoring the data, and to the 16 subjects.
Author Disclosure Statement
All three authors have no financial or nonfinancial conflicts of interest to declare.
Role of the sponsors: The Institute for Altitude Medicine fund had no interest or participation in study design or outcome.
Funding source: Institute for Altitude Medicine.
Guarantor statement: David S. Patz takes responsibility for the content of the manuscript including the data and analysis.
Author contributions: David S. Patz is the principal investigator providing initial conception and contributing importantly to study design, data acquisition and analysis. He contributed to drafting the article and approved the submitted version. Michael D. Patz contributed importantly to data analysis, and critically evaluated the submitted article, and approved the submitted version. Peter H. Hackett is co-investigator, contributing importantly to initial study design and data analysis. He contributed to drafting the article and approved the submitted version.