
Abstract
Abstract
Piergiuseppe Agostoni. Considerations on safety and treatment of patients with chronic heart failure at high altitude. High Alt Med Biol 14:96–100, 2013.—Prognosis and quality of life of chronic heart failure (HF) patients have greatly improved over the last decade. Consequently, many patients are willing to spend leisure time at altitude, usually <3500 m, but their safety in doing so is undefined. HF is a syndrome that often has relevant co-morbidities, such as pulmonary hypertension, COPD, unstable cardiac ischemia, and anemia. HF co-morbidities may per se impede a safe stay at altitude. Exercise at simulated altitude is associated with a reduction in performance, which is greater in HF patients than in normal subjects and greater in patients with most severe HF. In normal subjects, the reduction in performance is ∼2% every 1000 m altitude increase, whereas it is 4% and 10% in HF patients with normal or slightly diminished exercise capacity and in HF patients with markedly diminished exercise capacity. On-field experience with HF patients at altitude is limited to subjects driven to altitude (3454 m) for a few hours. The data showed a reduction in exercise capacity similar to that reported at simulated altitude. “Optimal” HF treatment in patients spending time at altitude is likely different from optimal treatment at sea level, particularly as regards β-blockers. Carvedilol, a β1–β2-α-blocker, reduces the hypoxic ventilatory response through a reduction of the chemoreflex response, and it reduces alveolar-capillary gas diffusion, which is under control by β2-receptors. These actions are not shared by selective β1-blockers such as bisoprolol and nebivolol, which should be preferred for treatment of HF patients willing to spend time at altitude. In conclusion, spending time at altitude (<3500 m) is safe for HF patients, provided that subjects are free of co-morbidities that may directly interfere with the adaptation to altitude. However, HF patients experience a reduction of exercise capacity in proportion to HF severity and altitude. Finally, HF patients should undergo a specific “altitude-tailored treatment” to avoid pharmacological interference with altitude adaptation mechanisms.

Introduction
Chronic HF is a syndrome which is characterized by the impairment of several body parts, such as lungs, kidney, muscles, pulmonary circulation, red blood cells, and sympathetic nervous system, all of which imply a specific adaptation to altitude or may be further impaired at altitude. Moreover, HF patients frequently have co-morbidities, such as—just to mention some—lung diseases, systemic hypertension, metabolic syndrome, peripheral and coronary vascular diseases, all of which may have a detrimental role in altitude adaptation, particularly when combined with HF. Therefore, patients with HF and lung disease, pulmonary hypertension—including out-of-proportion pulmonary hypertension due to HF (Simonneau et al., 2009)—anemia, severe renal insufficiency, angina, or primitive cardiac valvular or pericardial diseases, who are willing to ascend to altitude, should be evaluated for HF and also for the specific HF co-morbidities they are affected by. For instance, in a patient with HF and COPD, the latter is the factor that actually limits altitude exposure due to a greater arterial P
Several physiological adaptations to or consequences of high altitude exposure may, in principle, negatively influence the physical condition of HF patients, which includes the increase of sympathetic activity, pulmonary and systemic blood pressure, heart rate, lung fluid content, or the reduction of stroke volume (Agostoni et al., 2009; Cogo and Miserocchi, 2011; Rimoldi et al., 2010; Swenson, 2011). Some of these effects are limited in time but, because they are possibly associated with a deterioration of HF, they should be cautiously considered when evaluating whether a HF patient can go to high altitude. Therefore, at first glance, HF patients should be advised to not go to altitude, albeit it has been very recently suggested that repeated, short-lasting (3–4 hours) exposures to a simulated altitude up to 2700 m may be beneficial for HF patients in terms of quality of life, muscular strength, and exercise performance (Saeed et al., 2012). However, a 3–4-hour exposure may be different from a 24-hour or longer exposure, because the negative effects of some adaptations to high altitude may need more time to develop completely.
Very few non-laboratory, real-life experiences are presently available for HF patients at altitude. Indeed, albeit laboratory studies are able to mimic hypoxic conditions, this is not the case for other variables encountered at altitude, such as a cold and dry environment, as well as poor weather conditions in general. Exercising in a cold and dry environment does imply a greater energy consumption if compared to exercise performed in a comfortable setting. However, it is now appreciated that patients with coronary artery disease and preserved left ventricular function can safely reach altitude and exercise there, and that adverse cardiac events, such as unstable angina or coronary syndrome, do not occur more frequently than at sea level if subjects unaccustomed to exercise are excluded (Dehnert and Bartsch, 2010; Schmid et al., 2006; de Vries et al., 2010). Indeed, Schmid et al. (2006) showed that coronary patients who have been completely revascularized can safely go and exercise at the Jungfraujoch (3454 m), and de Vries et al. (2010) showed that patients with a history of myocardial infarction and preserved left ventricular function presented a decrease in exercise capacity similar to that of healthy controls at 4200 m in the Aconcagua region after a 10-day acclimatization (de Vries et al., 2010). No data are available for HF patients, except for another study of the Schmid group (Nobel et al., 2010), which showed that HF patients in stable clinical condition, class NYHA II, and with peak V
Several HF patients have implanted defibrillators (ICD) for arrhythmia treatment, and several have pacemaker-mediated resynchronization therapy (CRT) for HF treatment. At present, little information exists regarding function of ICD and CRT at altitude. Weilenmaen et al. (2000) studied 13 patients with single chamber pacemakers and found no changes in ventricular stimulation thresholds at a simulated altitude of 4000 m, although the duration of exposure was only 30 min and may not accurately reflect what would happen with longer stays in hypobaric hypoxia. Moreover, in a recent survey study in Swiss patients living at altitude, it has been reported that ICD shock was rare (4%) and it has been suggested that ICD patients living at moderate altitude may safely perform moderate physical activity (Kobza et al., 2008).
More precise information is available regarding exercise performance in HF patients during exposure to acute hypoxia as obtainable in a laboratory setting. Indeed, exercise performance was progressively reduced in HF patients if they exercised at a simulated altitude of 1000, 1500, 2000, and 3000 m (Fig. 1). Notably, this reduction was greater in HF patients than in normal subjects, and it was greater in the more severe HF patients (Agostoni et al., 2000), where the severity of the disease was defined by peak V
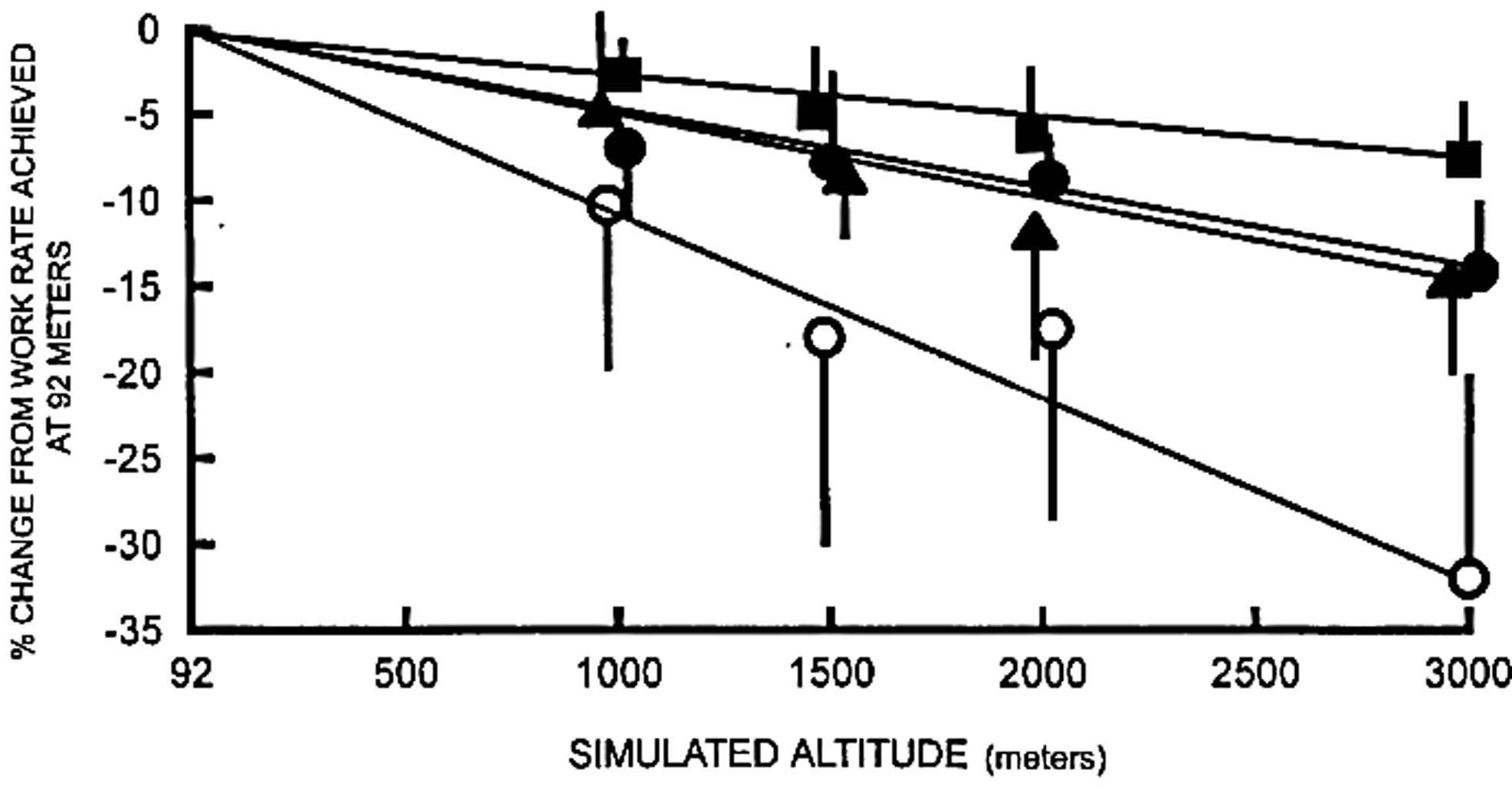
Mean (±95% confidence intervals) reduction in maximum work rate with simulated altitude, as a percentage decrease from maximum work rate at 92 m. Slopes differed (p<0.05) in healthy subjects (-2%±1% per 1,000 m; filled squares) compared with patients, and between patients with normal (-4±2%; filled circles), or slightly diminished workload (-4±2%; filled triangles) compared with patients with markedly diminished workload (-10±3%; open circles). From Agostoni et al., 2000.
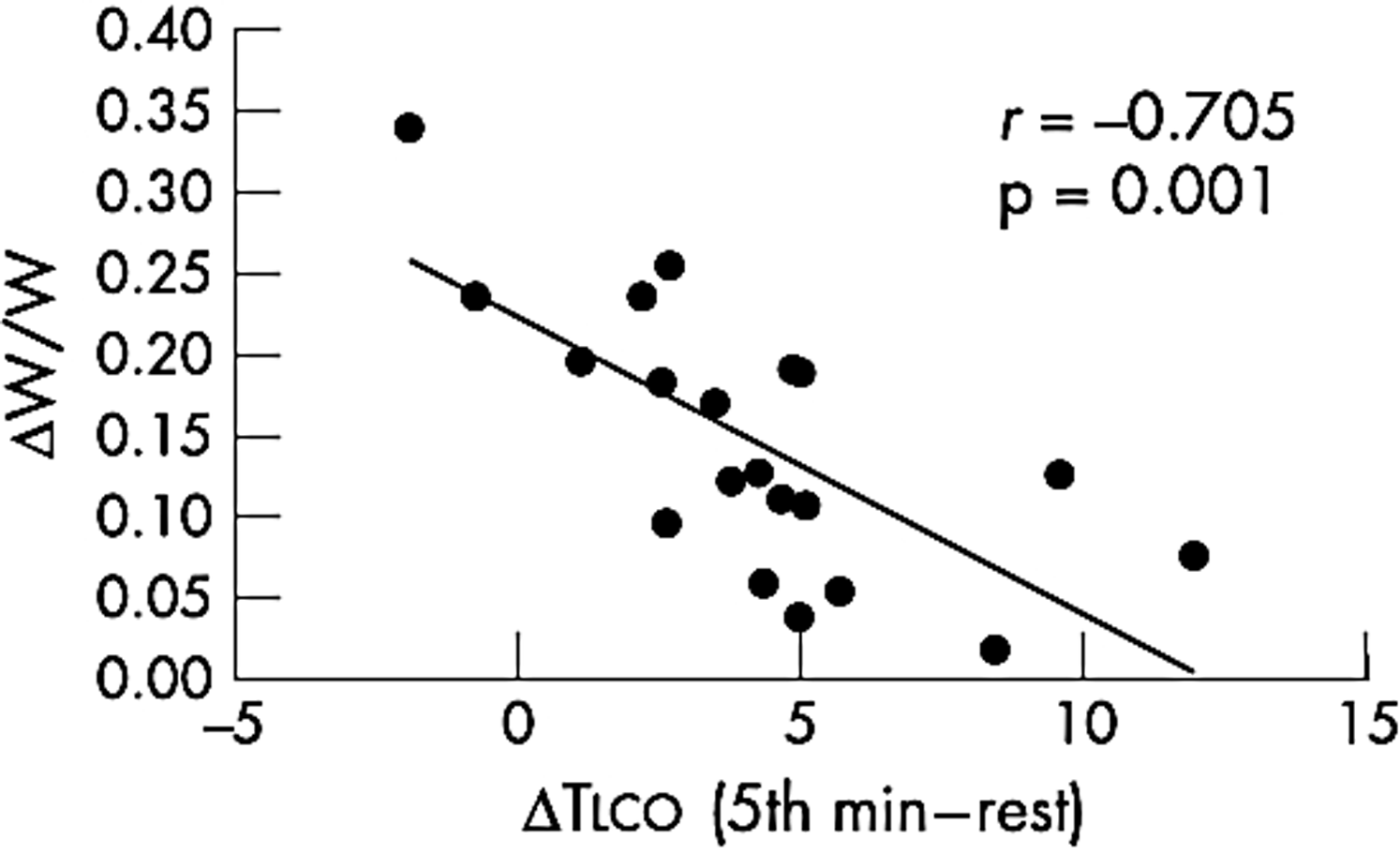
Reduction of exercise capacity in hypoxia. ΔW/W=[maximum workload achieved in normoxia - maximum workload achieved in hypoxia]/maximum workload achieved in normoxia. ΔTLCO=differences in lung diffusing capacity for carbon monoxide between the fifth minute of exercise and rest in heart failure patients. Patients with the greatest capability to increase TLCO during exercise are those who show the smallest reduction in exercise capacity in hypoxia. From Agostoni et al., 2002b.
It should also be noticed that we have no data on the effects of prolonged altitude sojourns for HF patients. Indeed, altitude adaptation includes, in healthy subjects, among others, improvement of ventilation, alveolar capillary diffusion, and oxygen carrying capacity in the blood. All these should increase exercise performance of HF patients. Similarly we have no data to answer the frequently asked question on how fast a HF patient can safely travel to altitude, including rate of ascent and staging at intermediate altitude. Consequently, cautious advice should be given to HF patiens willing to spend prolonged time at altitude.
All the above-reported data, either at simulated or at real altitude, have been obtained in HF patients in stable clinical conditions and on so-called optimal medical treatment. The latter is defined at sea level, but the optimal medical treatment for a given HF patient may be different at altitude. Two factors among several others that influence exercise performance at altitude, and precisely the alveolar capillary gas diffusion and the chemoreflex-mediated ventilatory response to hypoxia, are impaired in HF and, most importantly, they can be directly influenced by drugs used for HF treatment. Indeed, ion transport and the accompanying fluid movement across the alveolar capillary membrane are active phenomena under the control of β2 receptors located on the airway surface of type I and II alveolar cells, and chemoreflex is regulated by angiotensine, nitric oxide, β1, β2 and α receptors. Angiotensine 1 (AT1) receptor blockers and β-blockers are among the drugs used for the treatment of HF. The high-altitude adaptation of a normal subject on AT1 receptor blockers (telmisartan) is the main topic of an extensive research project, the HIGHCARE project, which was recently conducted at the Mount Everest South Base Camp (5400 m). No result on the effect of telmisartan on ventilatory and blood pressure control at high altitude has been released yet. Differently, it is now appreciated that the exercise performance of healthy subjects at high altitude is influenced by the type of β-blocker used. In a recent report, Valentini et al. (2011) showed that at Capanna Regina Margherita (4560 m) peak V
Some studies have been carried out by our group in Milan to assess the effects of HF treatment on exercise performance of patients at a simulated altitude of 2000 m (Agostoni et al., 2002a; 2002b; 2007). This altitude was chosen because it is likely to be reached by HF patients during leisure time in the mountains. Two issues were analyzed: the effects of different β-blockers on alveolar capillary gas diffusion and those on the regulation of ventilation during exercise. As regards their effects on alveolar capillary gas diffusion, chronic carvedilol treatment is associated to a reduction of total alveolar capillary diffusion, as inferable from DLCO measurement (Agostoni et al., 2002a). By splitting DLCO into its two components, membrane diffusion and capillary volume, we showed that carvedilol reduced the former. We then showed that DLCO was reduced in HF patients on carvedilol, but not in those on bisoprolol (Agostoni et al., 2006b), and that this reduction directly correlated with a reduction of exercise performance in HF patients with DLCO <80% of its predicted value (Agostoni et al., 2007). We very recently (Contini et al., 2012) confirmed this observation in a cross-over study comparing HF patients on carvedilol, bisoprolol, and nebivolol, the CARNEBI trial, and we showed that the reduction in DLCO was only observed during treatment with carvedilol. Interestingly, the reduction in DLCO was associated to an increase of the alveolar capillary p
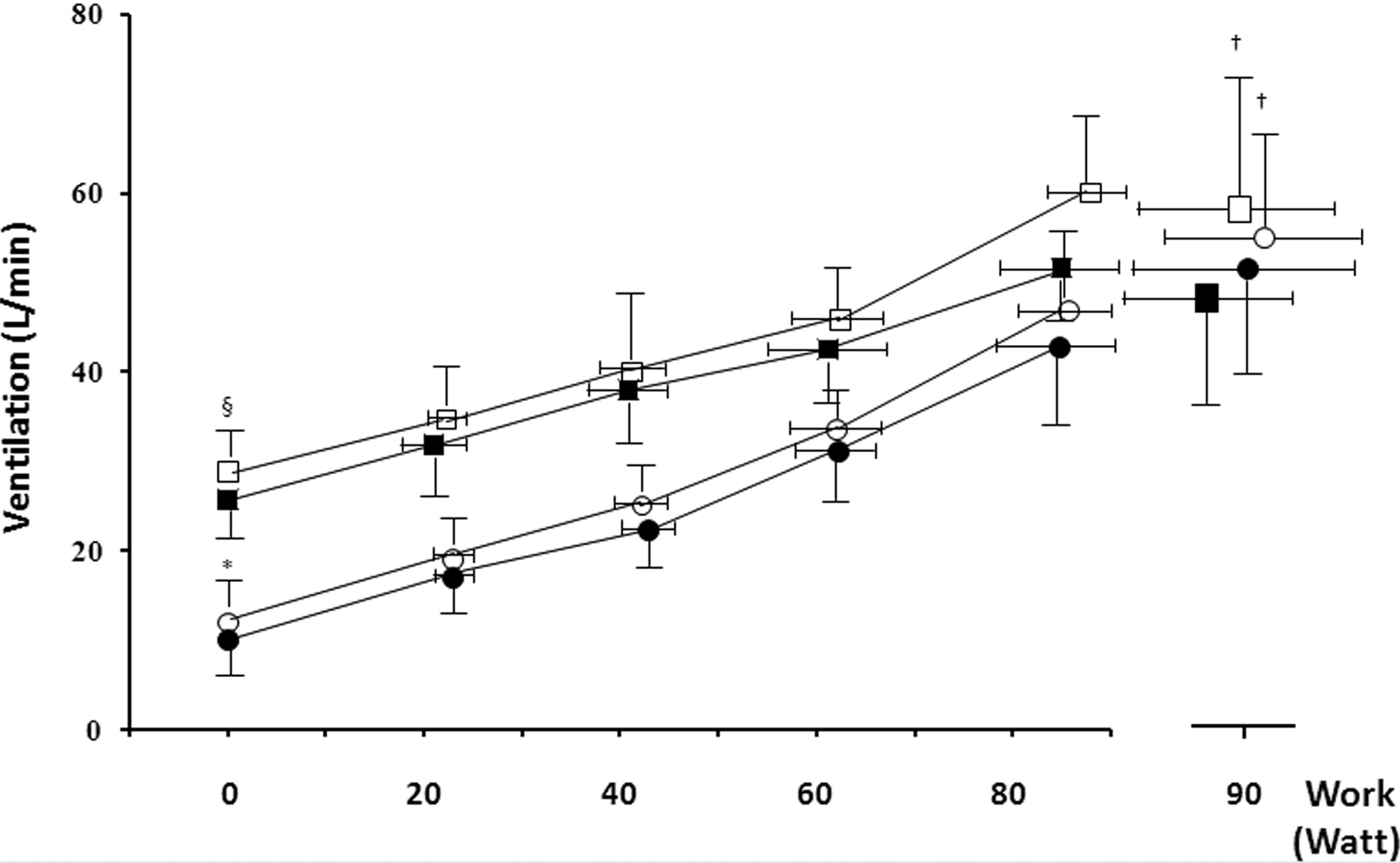
Effect of carvedilol (filled symbols) versus placebo (empty symbols) on ventilation at different work rates, both in normoxic (circles) and in hypoxic (squares) conditions. Data from Agostoni et al., 2006b.
In conclusion, HF patients can safely spend leisure time at altitude up to 3500 m, provided that they are on optimal, “altitude-tailored” HF treatment. HF patients, however, should expect a reduction of physical performance in relationship to the severity of the disease and to the altitude they will reach. Patients with HF co-morbidities should be evaluated with care, because the co-morbidities may definitively preclude HF patients from safely staying at altitude.
Footnotes
Author Disclosure Statement
No competing financial interests exist.