
Abstract
Abstract
Naeije, Robert, and Rebecca Vanderpool. Pulmonary hypertension and chronic mountain sickness. High Alt Med Biol 14:117–125, 2013.—Chronic mountain sickness is a syndrome of severe symptomatic polycythemia and hypoxemia occurring in natives or long-term high altitude sojourners. The condition may be complicated by pulmonary hypertension in proportion to decreased oxygenation, indicating hypoxic vasoconstriction and remodeling. Exercise in these patients is associated with a steep slope of pulmonary artery pressure-flow relationships and decreased vascular distensibility. Correction of pulmonary vascular resistance for increased hematocrit decreases the severity of pulmonary hypertension. Exercise-induced pulmonary hypertension in chronic mountain sickness does not affect exercise capacity, in relation to high oxygen content of the blood and increased lung diffusing capacity. Right ventricular failure seems to be an uncommon complication of chronic mountain sickness, but the exact prevalence of the condition is not known. Acetazolamide given for 6 months to patients with chronic mountain sickness improves oxygenation, polycythemia, and pulmonary artery pressure.
Introduction
The proposed cut-off values for hemoglobin and Ppam for the diagnosis of CMS and pulmonary hypertension derive from previously reported upper limits of normal for healthy South American permanent high altitude residents. However, this may introduce semantic difficulties when comparing the physiology of high altitude residents to sea level controls. It has been better realized in recent years that altitude limits of normal may be exposed to a large ethnic variability (West, 2012). Tibetans compared to Andeans present with lower hematocrits and higher arterial oxygen saturations (Beall, 2000) and no or only mild pulmonary hypertension (Groves et al., 1993, Hoit et al., 2005). Another potential source of confusion is about the purpose of the measurements. The diagnosis of hypoxic pulmonary vascular remodeling by an increased Ppam or pulmonary vascular resistance (PVR) obviously needs a correction for increased polycythemia-related viscosity, even though this is not commonly done. But a diagnosis of right ventricular failure on increased afterload requires a measurement of uncorrected Ppa, as the right ventricle “sees” pressure, not viscosity, and symptomatology of pulmonary hypertension is essentially caused by right ventricular failure (Champion et al., 2009). It may therefore be preferable to refer high altitude measurements of the pulmonary circulation to the universal definition of pulmonary hypertension as a Ppam≥25 mmHg with a PVR≥3 Wood units (Galiè et al., 2009; McLaughlin et al., 2009).
Hypoxic Pulmonary Vasoconstriction and Remodeling
Altitude is associated with a hyperbolic decrease in atmospheric pressure and inspired P
Pulmonary Hypertension at High Altitudes With or Without Chronic Mountain Sickness
After the report of HPV in cats, in 1946 (Von Euler and Lijestrand, 1946) and one year later in man (Motley et al., 1947), the first report in English of direct measurements of Ppa in humans living at high altitudes was published a decade later (Rotta et al., 1956). The authors catheterized the right heart of seven young adult healthy volunteers at sea level, six healthy lowlanders after 1 year of continuous residence in Morococha (4540 m), and seven native residents and two patients with CMS living permanently at >4000 m. Mean Ppa was 12 (range 9–15) mmHg in lowlanders at sea level, 18 (range 16–20) mmHg in lowlanders after 1 year in Morococha, 25 (range 18–29) mmHg in highlanders living in Morococha, and 34 and 35 mmHg in the two CMS patients (some of the Ppam calculated from systolic right ventricular pressure). There was a striking inverse correlation between oxygen saturation and Ppa or PVR. The authors suspected this to be related to HPV, but thought persistent vasoconstriction to be unlikely. They noted that supplemental oxygen did not affect PVR. Furthermore, pathological data available to them from accidentally deceased highlanders pointed at a “marked dilatation of the vascular bed of the lungs,” with no mention of structural changes. They excluded cardiac output, which was increased only in the CMS patients. Hyperventilation was most unlikely, as Ppa was the highest in the highlanders with the lowest levels of ventilation. They concluded that their results had to be explained by an increased blood volume essentially related to an increased red blood cell mass.
A few years later, pathologists showed that men born and living at high altitudes have remodeled pulmonary arterioles with medial hypertrophy and narrowed lumen resembling a fetal pattern (Naeye, 1962, Arias-Stella and Saldana, 1963). Penaloza et al. reported in 1963 on right heart catheterization in 38 healthy young men born in villages at altitudes>4000 m and having lived for at least 8 years>4500 m, and in 25 healthy young adults at sea level. Mean Ppa in highlanders amounted to 28±10 (mean±2 SD) mmHg compared to 12±2 mmHg in the controls. Wedged Ppa (Ppw) and right atrial pressures were low–normal, cardiac output was not different from sea level controls, and PVR was increased to 332±213 dynes x sec x cm−5. The authors concluded that increased PVR in high altitude dweller was explained by anatomical changes in the small pulmonary arteries and arterioles. They dismissed polycythemia and hypervolemia on the basis of different time courses of decreases in hematocrit and Ppa when high altitude natives are taken to sea level, and the observation that sea level patients with polycythemia do not present with pulmonary hypertension (Penaloza et al, 1963). It is of interest that the hemoglobin levels in their highlanders were at 19.5±1.97 g/dL, indicating a range from 15.5 to 23.5 g/dL, thus a proportion of subjects with hemoglobin levels corresponding to the definition of CMS.
In a review article written half a century after their initial pioneer observations, Penaloza and Arias-Stella plotted Ppam reported in life-long high altitude residents as a function of arterial oxygen saturation (Sa

Hyperbolic relationship between mean pulmonary artery pressure (PPA) and altitude of locations. Extremes are observed in Lhasa and in Leadville. From Reference 43, with permission.
The contrasting levels of Ppa reported in the inhabitants of Leadville and in Lhasa have been thought to be genetically determined (Penaloza and Arias-Stella, 2007). According to this reasoning, several ten-thousands of years of living at high altitudes in Tibet would have selected fitter individuals with lower HPV allowing for better survival and reproduction, while no such selection pressure would have acted on residents of Colorado, which was more recently populated with higher turn-over of communities. However, whether such a Darwinian evolution could have really occurred over a time period of only a few thousand years of colonization of high altitude plateaus remains currently debated (West, 2012).
Pulmonary Circulation During Hypoxic Exercise
While in most high altitude dwellers with and without CMS, Ppam is only mildly elevated at rest, exercise is associated with a sharp increase, which occurs with unchanged or slightly increased PVR, in contrast with the decrease in PVR normally observed at exercise at sea level (Penaloza and Arias-Stella, 2007). Banchero et al. (1966) catheterized the right hearts of 35 healthy men aged 17 to 34 years born and resident at altitudes higher than 4000 m, and living in Morococha (4540 m), and of 22 healthy men aged 17 to 23 years born and residing permanently in Lima, at sea level altitude. The measurements were obtained at rest and after 5 minutes of supine cycling at a workload of 300 kg-m/min/m2, corresponding to a V
Less severe exercise pulmonary hypertension was reported in a right heart catheterization study in 16 healthy highlanders born and living in La Paz “alto” (4000 m), but investigated in La Paz (3750 m). The subjects presented with a resting Ppam of 20±3, increasing to 32±8 mmHg at exercise (Lockhart et al., 1976). In six of the subjects with a Ppam at rest of 23±1, increasing to 34±6 mmHg at exercise, supplemental oxygen had no effect on Ppam at rest, but decreased Ppam to 28±3 mmHg at the same cardiac output at exercise, suggesting inhibition of exercise-induced vasoconstriction (Lockhart et al., 1976). The suggestion of exercise-induced pulmonary vasoconstriction in that study was supported by less steep single lung Ppam–Q in unilateral pulmonary artery balloon occlusion experiments. Vogel et al. (1962) reported invasive measurements of resting Ppam of 25 mmHg increasing to 54 mmHg at moderate exercise with workloads ranging from 25 to 100 W in subjects living in Leadville, at the altitude of 3100 m. In contrast, Groves and colleagues (1993) measured a Ppam of 15 mmHg, increasing to 35 mmHg at workloads ranging from 60 to 180 W in subjects living in Lhasa at 3658 m, allowing for the recalculation of slopes of Ppam–Q relationships at the upper limit of sea level normal (Groepenhoff et al., 2012). The highest Ppam and slopes of Ppam–Q plots have been reported by Penaloza and Sime (1971) in CMS patients with Ppam of 37 mmHg at rest and 82 mmHg at exercise.
With development of technology and investigator skills (Bossone et al., 2012), field echocardiographic studies of the pulmonary circulation have become possible. Stuber et al. (2010) reported on such measurements at rest and at a 50 W workload in subjects born and living in La Paz, at altitudes of 3600–4000 m. The results showed a Ppam of 20 mmHg at rest and 29 mmHg at mild exercise (slope of Ppam–Q 3 mmHg/L.min−1) in healthy highlanders, and 23 mmHg increasing to 39 mmHg (slope of Ppam–Q 5 mmHg/L/min−1) in highlanders with CMS. Groepenhoff et al. (2012) reported on Ppam–Q plots in 13 patients with CMS, 15 healthy highlanders, and 15 matched lowlander controls confirming these results. Slopes of Ppam–Q were on average 4.8 mmHg/L/min in CMS patients, 2.8 mmHg/L/min in healthy highlanders, and 1.7 mmHg/L/min in recently acclimatized lowlanders.
These studies, altogether summarized in Figure 2, show that pulmonary hypertension in patients with CMS is at the high extreme of a spectrum of responses depending of individual and ethnic variability in pulmonary vascular reactivity to hypoxia.
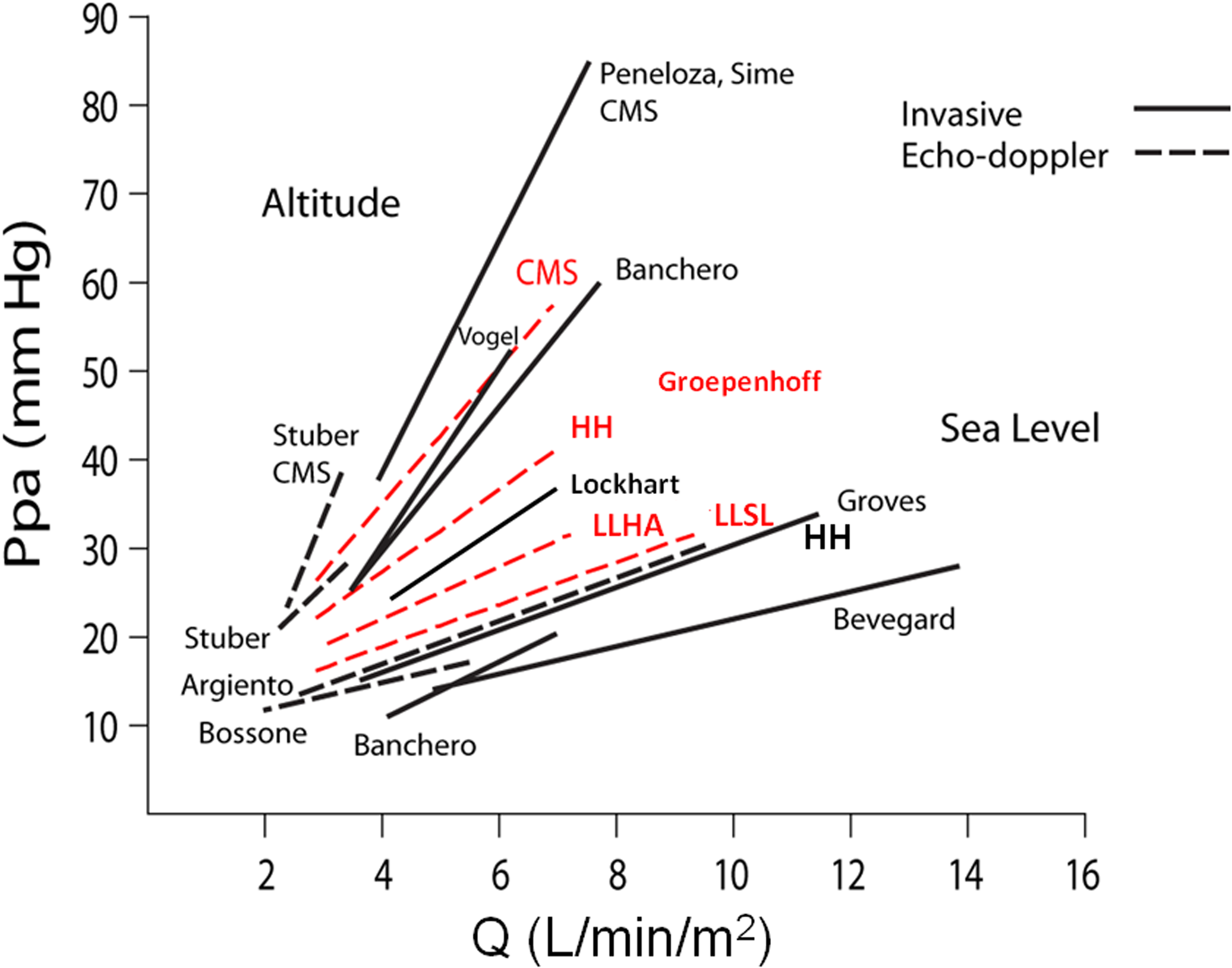
Range of mean pulmonary artery pressures (Ppa) expressed as a function of cardiac index (Q) at exercise in high altitude (HA) and sea level (SL), high altitude (HH), and sea level (SL) inhabitants. Source studies are indicated by names of first authors. Highlanders present with higher resting Ppa and increased slopes of Ppa–Q. Adapted from Ref. 13, with permission.
Effects of Pulmonary Vascular Distensibility
Multipoint Ppam–Q coordinates measured at several levels of workload can usually be described by a linear approximation. The slope of linearized Ppam–Q is always less than predicted by the resting PVR equation. This is explained by the distensibility of pulmonary resistive vessels (Naeije and Chesler, 2012). Attentive examination of the shape of multipoint Ppam–Q relationships actually discloses a slight curvilinearity (Linehan et al, 1992, Reeves et al., 2005). The resistive vessel distensibility accounting for it can be calculated using a mathematical model of the pulmonary circulation integrating realistic changes in pulmonary vascular resistance and compliance (Linehan et al., 1992). The derived PVR equation expresses Ppam as a function of Q, total PVR (Ro), left atrial pressure (Pla) and distensibility coefficient (α):

This approach was applied to invasive measurements obtained on normal volunteers in hypobaric chamber experiments that simulated an ascent on Mount Everest. Hypoxic exposure during several weeks in these subjects increased PVR from 2.3±0.2 to 3.9±0.2 Wood units and decreased α from 2±0.2 to 0.8±0.1 % diameter change per mmHg pressure. The same calculations on the individual data of acute hypobaric exposure experiments reported in another group of healthy volunteers did not show any difference in α, but in that study, PVR remained unchanged and hypoxic exposure was short (Wagner et al., 1986).
Pulmonary vascular pressure flow relationships have been recently reported in 110 healthy volunteers studied by exercise stress echocardiography at sea level (Argiento et al., 2012). The results show an averaged linear slope of Ppam–Q of 1.51±0.54 mmHg/L/min and α of 1.3±1.0 %/mmHg in keeping with previous invasive studies. The distensibility coefficient α was on average lower in men than in pre-menopausal women and decreased with age. A recent preliminary study suggested that α might be decreased in asymptomatic carriers of the BMPR-2 mutation, known to carry a 20% risk to develop pulmonary arterial hypertension, possibly reflecting early vascular disease (Pavelescu et al., 2012).
Groepenhoff et al. (2012) found an unchanged α in recently acclimatized lowlanders, in keeping with minimal increase in PVR in that particular group and short term 24–48 h hypoxic exposure. In that study, along with increased slope of Ppam–Q, α decreased from a sea level 1.7 %/mmHg to an altitude value of 1.4 %/mmHg in the lowlanders. It was at 0.7 %/mmHg in healthy highlanders and was very low at 0.3 %/mmHg in patients with CMS. The averaged Ppam–Q relationships recovered in that study are shown in Figure 3, illustrating higher Ppam at any level of cardiac output in patients with CMS compared to healthy highlanders, while the recently acclimatized lowlanders had almost no hypoxic vasoconstriction. These results were likely explained by the authors by more pronounced pulmonary vascular remodeling in CMS patients than in healthy highlanders, with possibly an added component of exercise-induced vasoconstriction.

Average mean pulmonary artery pressure (Ppa) versus cardiac output (Q) plots in 15 healthy lowlanders (LL), 15 highlanders (HH), and 13 patients with chronic mountain sickness investigated at Cerro de Pasco (4350 m), without (full lines) and with (dashed lines, arrows) a correction for hematocrit with an equation reported by Linehan et al, 1992. Limits of normal at sea level are shown by the shaded area.
Viscosity
One wonders why relatively little attention has been paid until now on the effects of increased red blood cell mass in studies on the pulmonary circulation at high altitudes. Increased red blood cell mass increases Ppa at any given level of flow and resistance because of increased viscosity of the blood. In Poiseuille's equation relating pressure drop and flow through rigid glass tubes, resistance is linearly related to viscosity as

where l is tube length, r is the radius, and η a viscosity coefficient. This is transposed to the pulmonary circulation by dividing by a factor of k to account for the number of parallel vessels, assuming l is constant for the pulmonary circulation, r is the internal radius of the resistive vessels, the pressure drop is Ppam minus Ppw, and flow is cardiac output (Q)

Red blood cell mass is usually assessed in clinical practice by a measurement of hematocrit. Several equations have been used to describe the relationship between hematocrit and viscosity. Because viscosity is proportional to resistance and a function of hematocrit, a relative resistance at a hematocrit of 45% can be calculated from a measured resistance using

We re-examined the contribution of blood viscosity to previously reported Ppam–Q relationships (Groepenhoff et al., 2012) by calculating a relative total PVR at a hematocrit of 45% (R0(45%)) for each group from the measured R0 at rest (R0(HCT)) using either an exponential relationship used by Linehan et al. (1992) to explain the effect of hematocrit on Ppam–Q relationships in isolated dog lung experiments,

where ϕ is the hematocrit. We repeated the analysis with the more classically cited relationship between blood viscosity and hematocrit derived from hindlimb vessel studies by Whittaker and Winton (1933):

These relative R0(45%) values (Table 1) were then introduced in Linehan's distensible model. The results are shown in Figure 3 for Ro(45%) calculated with Linehan exponential relationship. Increased hematocrit largely explained the upward shift of Ppam–Q relationships in healthy highlanders, and even more so in CMS patients. The proportionally more important contribution of increased hematocrit to slope of Ppam–Q in CMS patients is explained by their less distensible pulmonary circulation. These results were similar with Ro(45%) recalculated with the Whittaker and Winton's relationship.
Values as measured and after correction for relative increase in hematocrit (HCT) using either an exponential equation (Linehan, 1991) or a linear equation (Whittaker and Winton, 1933).
It is remarkable that corrections for hematocrit brought average resting values for Ppam at the upper limit of the normal range. This observation, together with recent report of mild pulmonary hypertension in Tibetans (Hoit et al., 2005) introduces doubt as to whether phenotypic differences between Tibetans and Andeans include intrinsic differences in pulmonary vascular reactivity and remodeling.
The effects of increased hematocrit on the pulmonary circulation was investigated by Manier et al. (1988) in a study on the effects of isovolemic hemodilution on pulmonary gas exchange in eight Bolivian subjects born and living at altitudes between 3600 and 4200 m and investigated in La Paz (3650 m). The hematocrits were above 3 SD's of normal residents in that city, and five of the subjects had a hemoglobin higher than 21 g/dL. Isovolemic hemodilution decreased hemoglobin from 21.5±1.6 g/dL to 18.2±2.0 g/dL, hematocrit from 66±7 to 56±7 % and PVR from 3.9±1.6 to 3.1±1.2 Wood units. The individual PVR responses to decreased hematocrit were predicted by Linehan's equations (Fig. 4).
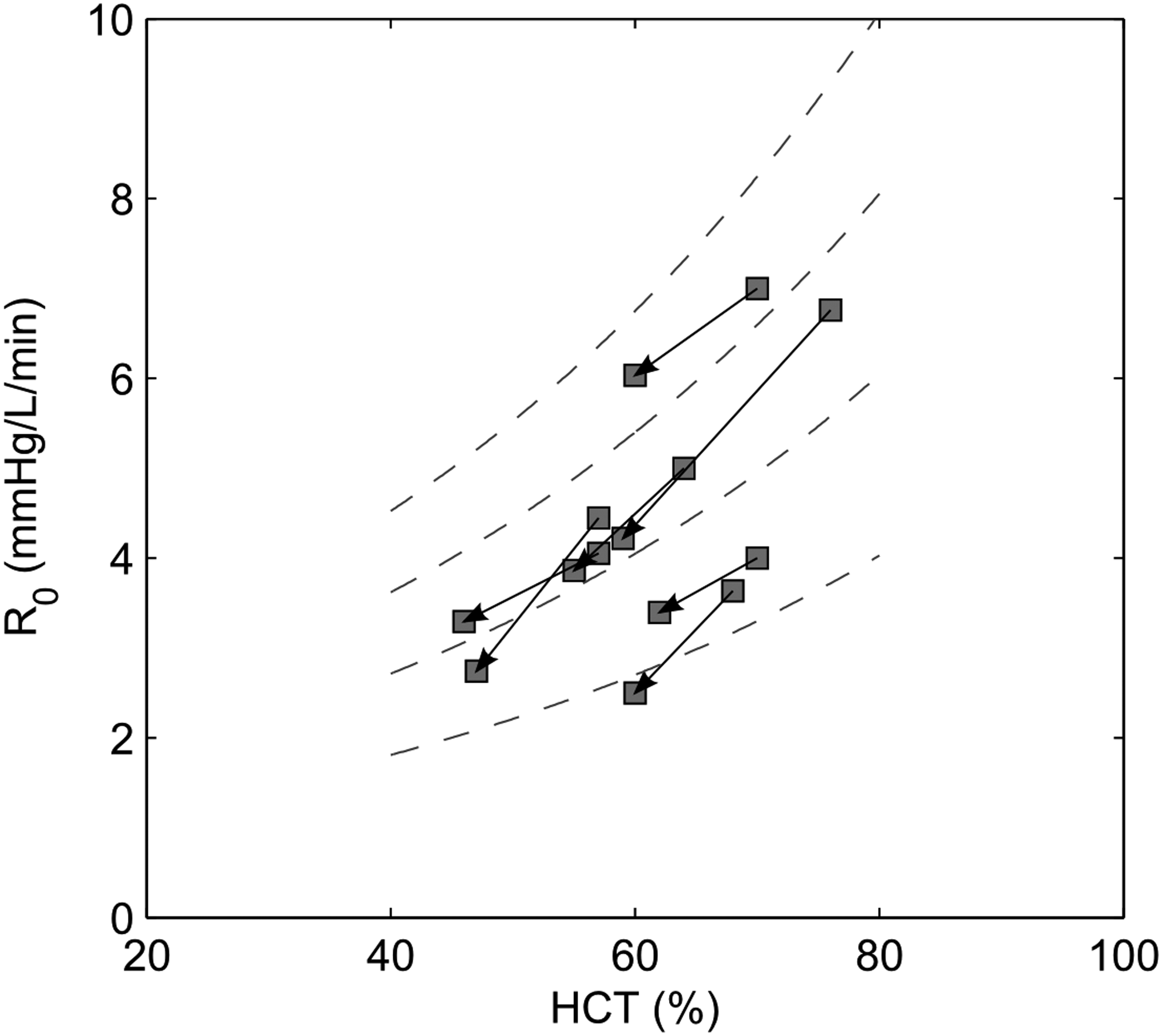
Prediction of changes in total pulmonary vascular resistance (Ro) as a function of changes in hematocrit (HCT) in 8 subjects with increased hematocrit before and after isovolemic hemodilution (arrows). Stippled lines show model predictions from a Ro of 2 Wood units at a hematocrit of 45%. Changes in Ro were predicted by a distensibility model of the pulmonary circulation incorporating the effects of hematocrit on viscosity of the blood reported by Linehan et al, 1992.
Winslow et al. (1985) reported on the effects of isovolemic hemodilution in one CMS patient living in Cerro de Pasco (4350 m). A decrease in hematocrit from 62 to 42% and hemoglobin from 22.4 to 16 g/dL, decreased Ppa from 42/34 to 22/9 mmHg with an increase in cardiac output from 4.1 to 5.4 L × min−1, thus allowing for an estimated similar change in PVR. Thus, model predictions of PVR changes as a function of hematocrit are in keeping with reported effects of isovolemic hemodilution.
The contribution of increased hematocrit to PVR in highlanders with or without CMS has been usually dismissed on the basis of circumstantial arguments (Penaloza et al., 1963) or previous experimental studies showing little impact of increased hematocrits in the range reported at high altitudes (Lockhart et al., 1976). Maggiorini and Leon-Velarde (2003) mentioned a relationship between increased hemoglobin and Ppam in Himalayan and Andean studies on high altitude residents. Their analysis suggested an “out of proportion” pulmonary hypertension in CMS. The present recalculations rather suggest that much of the pulmonary hypertension in CMS may be explained by an increased viscosity of the blood. How common a real “out of proportion” pulmonary hypertension occurs in high altitude dwellers with or without CMS remains to be determined. The expert consensus advice on the diagnosis of pulmonary hypertension at high altitudes might have to go a step further than a mention about “excessive polycythemia” (Leon-Velarde et al., 2005) and consider a more systematic correction factor for hematocrit.
Relevance to Exercise Capacity
Recent studies have introduced a new notion of “pulmonary vascular reserve” as a limiting factor to exercise capacity. This is a combination of low PVR, shallow slope of Ppam-Q, high pulmonary vascular distensibility and diffusing capacity, and early exercise pulmonary transit of agitated contrast (La Gerche et al., 2011, Lalande et al., 2012). There is evidence that pulmonary vascular reserve also contributes to limit exercise capacity at high altitudes (Naeije, 2011, Pavelescu et al., 2013). It is thus surprising that CMS patients appear to have a preserved aerobic exercise capacity compared to healthy highlander or lowlander controls studied at the same altitude, in spite of important differences in pulmonary vascular responses (Groepenhoff et al., 2012). This is to be explained by compensatory lung diffusing capacity and increased arterial O2 content. The finding that maximum workload and V
Right Ventricular Failure
High altitude exposure has been reported to be associated with right heart failure. This complication of increased Ppa occurs in cattle brought to high altitude pastures (Hecht et al., 1962), in Indian soldiers transported from sea level to high altitude borders with China (Anand, 1990), and in Han Chinese immigrants to Tibet (Sui et al., 1988, Pei et al., 1989). A case of echocardiographic acute right heart failure has been reported in a lowlander with known strong HPV within the first days of arrival at the altitude of 4000 m (Huez et al., 2007). In this patient, the clinical examination was unremarkable. The expanding use of echocardiographic devices will probably allow for more frequent diagnosis of clinically silent cases of “high altitude right heart failure.” Patients with end-stage CMS may present with clinical signs of heart failure, but very few measurements have been reported to substantiate this diagnosis. Chronic hypoxia and relative hypercapnia could be a cause of salt and water retention in otherwise mildly afterloaded right heart, thereby causing congestion, but this also deserves more investigation.
Echocardiographic measurements of the heart have been reported in one study on high altitude Peruvian dwellers with a diagnosis of Monge's disease (Maignan et al., 2009). The patients presented with trans-tricuspid gradients at an average of 34 mmHg, but also relatively low arterial P
Animal Models
Transgenic mice that constitutively overexpress the human erythropoietin gene as a model of CMS have marked pulmonary hypertension in vivo, but not in blood-free perfused lungs, decreased pulmonary vascular smooth muscle mass and decreased vasoreactivity, along with an increase prostacyclin and nitric oxide production (Hasegawa et al., 2004). In hypoxic conditions, these mice do not develop right ventricular hypertrophy despite hematocrits increased to an average of 86%, have less pulmonary vascular remodeling than wild-type controls, and their pulmonary vasoreactivity to thromboxane analogs or hypoxia is reduced (Weissmann et al., 2005). There are data suggesting that blood viscosity in transgenic mice overexpressing erythropoietin is less than predicted from the increased hematocrit, in relation to increased elongation of erythrocytes at physiologic shear rates (Vogel et al., 2003). Thus, experimental animal data suggest endothelial function and erythrocyte mechanics adaptations limiting the increase in PVR caused by polycythemia. Whether this is relevant to polycythemic patients with CMS is uncertain. Our modeling predictions of the effects of increased hematocrit and the previous isovolemic hemodilution experiments rather suggest a limited or even insignificant functional component to polycythemia-associated increase in PVR.
An interesting consequence of polycythemia is decreased ventilation, in relation to the increased CO2 content of the blood, allowing for more CO2 output at any given level of P
Treatment of Pulmonary Hypertension in Chronic Mountain Sickness
A variety of treatments have been previously proposed for pulmonary hypertension in CMS patients, but with very few controlled trials (Rivera-Ch et al., 2007). The most obvious nonpharmacological treatment of CMS is to move the patients to lower altitudes, which has been shown to be associated with a complete reversal of excessive polycythemia and pulmonary hypertension (Sime et al., 1971). However, this is often impossible for social and economical reasons. Another option is blood-letting, with or without isovolemic hemodilution, which has been reported in observational studies to produce symptomatic improvement along with transient decreases in hematocrit lasting for several days to several weeks (Rivera-Ch et al., 2007). Repetitive blood-letting carries a serious risk of iron depletion, which is associated with an enhanced hypoxic pulmonary vasoconstriction (Smith et al., 2008) and worsening of pulmonary hypertension in CMS patients (Smith et al., 2009). Thus, the practice of blood-letting in CMS requires re-evaluation. On the pharmacological side, there has been a small randomized study showing a decreased packed cell volume and hemoglobin after 2 years of treatment with the angiotensin converting enzyme inhibitor enalapril 5 mg/day in 26 subjects living in La Paz (Plata et al., 2002). The study has not been repeated on a larger scale in patients with current definition of CMS. There is need of more extensive evaluation of possible clinical effects, and measurements of the pulmonary circulation, of angiotensin converting enzyme inhibitors in CMS. Experimental and some anecdotal clinical evidence suggest that methylxanthines might improve polycythemia, but this has not been tested in a controlled clinical trial (Rivera-Ch et al., 2007).
There has been interest in acetazolamide as a potential pharmacological treatment of CMS. Acetazolamide decreases the renal reabsorption of bicarbonate and thereby induces a metabolic acidosis with increased ventilation and improved oxygenation (Swenson, 1998). The drug has been reported to inhibit HPV acutely in experimental animals (Deem et al., 2000, Hohne et al., 2007) and also in a human study (Teppema, 2007), but does not appear to prevent more chronic hypoxic pulmonary vascular remodeling (Faoro et al., 2007). Acetazolamide decreases erythropoietin production essentially through an improved oxygenation of the blood. Richalet et al. (2005) reported a 3-week randomized controlled trial of acetazolamide in 30 CMS patients living in Cerro de Pasco (4350 m). Acetazolamide decreased hematocrit and serum erythropoietin, increased ventilation, and improved oxygenation (Richalet et al., 2005). These results were confirmed in a longer 3-month randomized controlled trial, followed by a 3-month extension in 55 patients (Richalet et al., 2008). The patients treated with acetazolamide had a significant decrease in the acceleration time of Doppler pulmonary flow-velocity, indicating pulmonary vasodilation. Echocardiographically-determined PVR did not significantly change in this CMS group with near-normal baseline PVR at an average of 1.75 Wood units (Richalet et al., 2008). It would be interesting to repeat the study in CMS patients with severe pulmonary hypertension.
There has been no randomized controlled trial of drugs shown effective in pulmonary arterial hypertension, such as prostacyclins, endothelin receptor antagonists, or phosphodiesterase-5 inhibitors (Galiè et al., 2009; McLaughlin et al., 2009). In addition to obvious logistic difficulties in organising such trials, there would be a problem in selecting the most relevant end-points. This will be a challenge to address in future expert consensus conferences on high altitude diseases.
Conclusions
Patients with CMS present with pulmonary hypertension at rest and more so at exercise. This is explained by increased pulmonary vasoconstriction and remodeling, but also by increased hematocrit. Whether pulmonary hypertension has to be added to hypoxic ventilatory response, oxygen saturation, and hemoglobin concentration as phenotypic differences between Andean and Tibetan populations is not yet entirely clear. Further studies are needed to define the possible contribution of hypoxic pulmonary vascular disease to heart failure reported in advanced CMS. The definition of pulmonary hypertension at high altitude may have to align on international guidelines, with a cut-off value of 25 mmHg for mean pulmonary artery pressure, but also with a correction factor for hematocrit.
Footnotes
Acknowledgment
We are grateful for the critical review of the manuscript by Dante Penaloza.
Author Disclosure Statement
No competing financial interests exist.