
Abstract
Abstract
Spliethoff, Kerstin, Daniela Meier, Isabelle Aeberli, Max Gassmann, Wolfgang Langhans, Marco Maggiorini, Thomas A. Lutz, and Oliver Goetze. Reduced insulin sensitivity as a marker for acute mountain sickness? High Alt Med Biol 14:240–250, 2013—Reduced insulin sensitivity might increase the susceptibility to acute mountain sickness (AMS). The diabetogenic side effects of dexamethasone should therefore be considered for AMS treatment. To examine whether reduced insulin sensitivity is predictive of AMS and how it is affected by dexamethasone at high altitude, we analyzed endocrine and metabolic parameters obtained from healthy mountaineers in Zurich (LA; 490 m), and 2 and 4 days after fast ascent to the Capanna Regina Margherita (HA2, HA4; 4559 m). 14 of 25 participants developed AMS and were treated with dexamethasone starting in the evening of HA2. Before and after ingestion of an 1800 kJ meal, plasma was analyzed for erythropoietin (EPO) and cholecystokinin (CCK). Insulin sensitivity (HOMA-S) and beta cell activity were calculated. HOMA-S (p<0.01) and EPO levels (p<0.05) were lower in Zurich in the group developing AMS and given dexamethasone, i.e., before treatment and exposure to hypoxia. CCK was lower (p<0.01) and glucose and insulin were higher on HA4 in the dexamethasone group compared to the untreated group. Individuals with low baseline insulin sensitivity and low baseline EPO levels were more susceptible to AMS. Reduced CCK may contribute to the beneficial effect of dexamethasone on high altitude anorexia. However, reduced insulin sensitivity questions the widespread use of dexamethasone to prevent/treat AMS.
Introduction
AMS has an incidence of 15%–80% depending on individual susceptibility, acclimatization, speed of ascent, and maximum height reached above 2500 m (Hackett et al, 1976; Jackson et al, 2010; Maggiorini et al, 1990; Mairer et al, 2010). Most common symptoms of AMS are headache, insomnia, fatigue, dizziness, breathlessness, anorexia, and nausea (Hackett et al, 1976; Imray et al, 2010; Silber et al, 2003; Wu et al, 2010).
The underlying molecular mechanisms for dexamethasone-mediated improvement of mountaineers suffering from AMS are complex and only partly understood. This is due to the fact that the primary cause of AMS is still not well known. Because hypoxia-induced systemic inflammation, as well as an exaggerated sympathic tone play a role in the development of AMS (Hartmann et al, 2000; Julian et al, 2011; Klausen et al, 1997; Scherrer et al, 1993), the anti-inflammatory, immunosuppressant and sympatholytic action of dexamethasone could at least partly be responsible for dexamethasone's beneficial effects in AMS. Further, dexamethasone may modulate the release and action of gastrointestinal hormones that control food intake. Cholecystokinin (CCK), an important satiation hormone associated with generation of dyspeptic symptoms (Fried and Feinle, 2002; Pilichiewicz et al, 2008), has been shown to be increased in plasma at high altitude, and may play a role in the development of AMS-caused anorexia (Bailey et al 2000). Dyspeptic symptoms have also been observed in our study (Goetze et al, 2010) and CCK is known to decrease by dexamethasone in cultured cells, as well as in rats in vivo (Ratineau et al, 1996).
Dexamethasone, however, has a wide range of undesired side effects. In addition to its immunosuppressant impact that potentially increases the risk of infections and impaired wound healing, glucocorticoids have catabolic and diabetogenic effects on fat and carbohydrate metabolism (Lee et al, 2011; Sood and Ismail-Beigi, 2010; Wajngot et al, 1992). Unfortunately for diabetics, the risk of side effects of dexamethasone treatment is even higher than for healthy subjects because high altitude hypoxia itself may lead to changes in glucose homeostasis (Henriksen et al, 1999; Larsen et al, 1997). This may result in changed insulin requirements and, eventually, in a deterioration of their metabolic disorders.
Therefore, as a primary endpoint we investigated potential metabolic differences in patients with AMS, in particular concerning insulin sensitivity, metabolites, glucose metabolism, and gastrointestinal hormones. All these data were analyzed retrospectively depending on whether individuals required dexamethasone when exposed to high altitude.
Methods
Subjects
Twenty-five healthy and experienced mountaineers (15 male; 22–60 years) were recruited by advertisements in mountain journals. As we were interested in AMS and therefore avoided acclimatization, volunteers were not allowed to stay more than 3 nights above 2500 m for at least 1 month prior to the fast ascent. Any prophylactic medication (e.g., with acetazolamide) that could have an impact on acclimatization and the development of AMS was excluded as well. None of the subjects was in need of any frequent or continuous medical treatment. Exclusion criteria were chronic diseases, regular medication, history of transplantation, clinically significant heart diseases, and congenital heart or lung disease. Most volunteers had a body mass index (BMI) between 18 and 25 kg/m2, but two persons with a BMI slightly above 25 and one with a BMI of 31 were also included. Participants had to show normal eating behavior and were not allowed to require special diets. Eight subjects were known to have experienced high altitude pulmonary edema (HAPE) in past ascents to altitude. Informed consent was taken of all subjects. The Ethics Committee of the Canton of Zurich approved the study (EK-1677) that conformed to the declaration of Helsinki.
Study procedure and power calculation
We performed a power calculation to assess the sample size for the endpoint detection of a significant effect of dexamethasone on postprandial glucose concentrations. These calculations were based on a recent study by Abdelmannan et al. (2010). Those authors tested different doses of dexamethasone on postprandial glucose concentrations in healthy volunteers after a 75 g oral glucose tolerance test (OGTT) and measured an increase of blood glucose concentrations from 127±7.1 mg/dL to 176±19 mg/dL after a single dose of 8 mg dexamethasone given 24 h before the following OGTT. The carbohydrate amount given in the present study and the single dose treatment with dexamethasone were comparable to the experimental settings in the previous study (carbohydrate content of the muffin 52.91 g) (Abdelmannan et al, 2010). Based on these data, we calculated a sample size of only 4 volunteers and decided that a sample of 25 healthy volunteers would be high enough to detect a significant difference for our endpoint (effect size dz=2.9467321, α error probability=0.05, power (1-β error probability)=0.95; noncentrality parameter δ=5.8934642, critical t=3.1824463, df=3, analysis done by G*Power Version 3.1.3).
Subjects underwent baseline physical examinations to ensure they met the inclusion criteria. First blood samplings were done in Zurich (LA), 490 m above sea level, P

Scheme of study travel itinerary.
AMS assessment and medication
Occurrence of AMS was assessed using the Lake Louise Score (LLS>5) and through medical examination by experienced physicians. This study was not designed to assess the effects of dexamethasone on high altitude physiology in a randomized double-blind placebo controlled fashion. Therefore, for safety reasons, only subjects with high HAPE susceptibility, a LLS greater 5 in the morning or evening of HA2 or necessity identified by medical examination were treated with 2×8 mg/day dexamethasone (9-fluor-16a-methylprednisolone, Dexamethasone Galepharm, 4 mg, Galepharm AG, 8700 Kuesnacht, Switzerland) starting on the evening of HA2 (i.e., after the last blood sample had been taken on that day). One person had to be treated with dexamethasone already earlier on Day 2 so that this subject was excluded from the analysis. Due to the occurrence of AMS, 14 subjects had to be treated with dexamethasone (DEX) and 11 served as untreated controls (CON).
Study design and sample processing
Blood gas analysis was done in blood taken from the arteria radialis using an ABL 5 blood gas analyzer (Radiometer, Copenhagen). Blood samples were taken at ground level in Zurich (LA) and on Days 2 and 4 (HA2 and HA4) at the Capanna Regina Margherita. On the morning of each test day, a venous catheter was placed in the forearm to allow for blood sampling. Blood sampling was performed in the morning before an ad libitum breakfast at 07:00 AM (fasted hormone levels, Figs. 2 and 3), just before and 30, 60, 90, 120, 180, 240 min after a test meal of two muffins at 01:00 PM (1.76 g dietary fiber, 12.52 g protein, 18.06 g fat, 52.91 g carbohydrates, 1800 kJ), and between an additional muffin preload and ad libitum dinner at 07:00 PM of each test day. For dinner, subjects were offered pasta, bolognese sauce, grated parmesan cheese and two sorts of biscuits. They were free to choose quantity and kind of food. All food consumed was weighed on a kitchen scale to the nearest gram, and energy intake was calculated. EDTA-plasma samples were kept frozen in liquid nitrogen or stored in −80°C for later analysis.
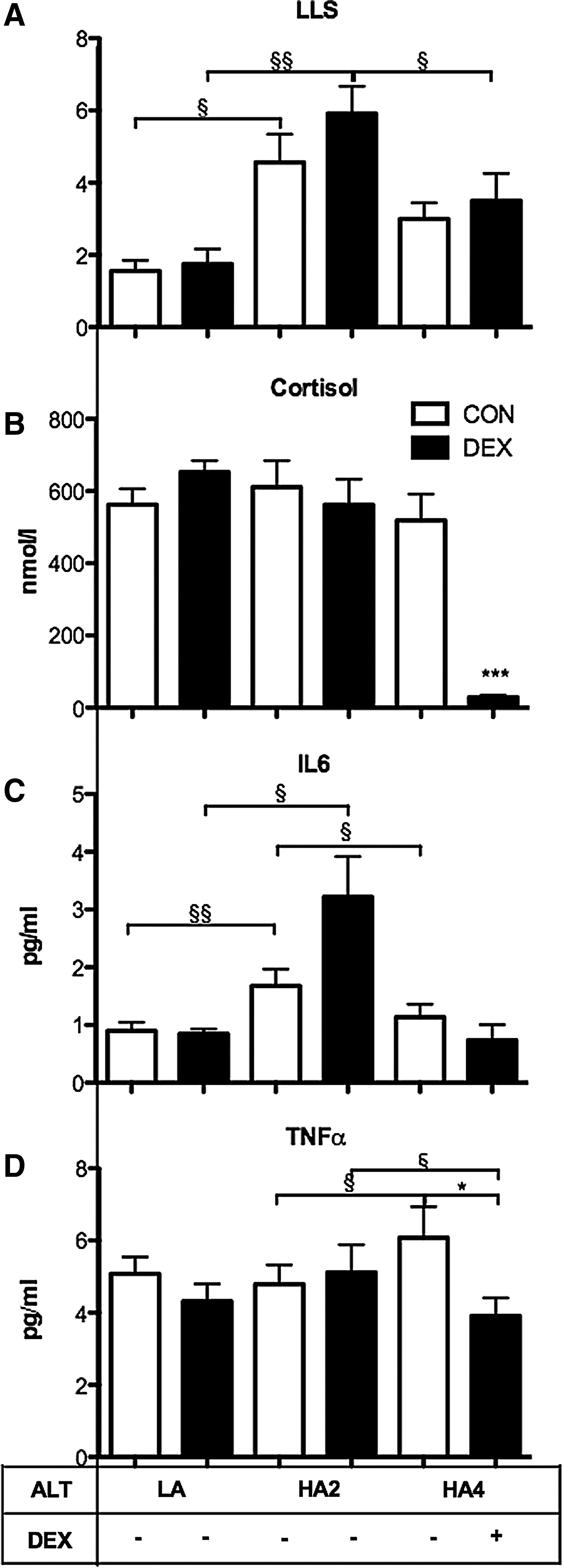
Inflammation and clinical AMS. Effects of hypoxia and dexamethasone on Lake Louise Score (LLS), (
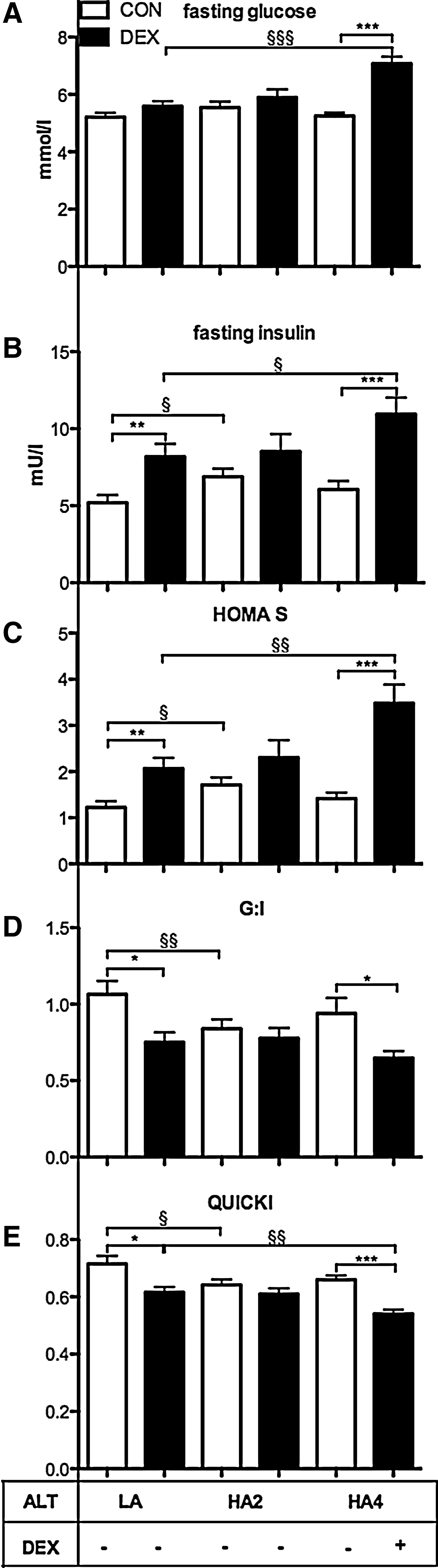
Glucose metabolism, fasted state. Effects of hypoxia and dexamethasone on fasting glucose and insulin. (
Plasma analysis
Inflammation markers
Cortisol was determined by electrochemiluminescence (Elecsys® Cortisol, Roche, Switzerland). Interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α) were measured using the Milliplex® MAP Human Cytokine/Chemokine Assay (Millipore). Erythropoietin (EPO) was determined with the Human Erythropoietin Immunoassay (Quantikine, IVD, R&D Systems, Minneapolis, MN,USA).
Gastrointestinal hormones
The Milliplex® MAP Kit Human Endocrine (Millipore, Billerica, MA, USA) was used for amylin. Cholecystokinin (CCK-8; active) was measured using Radioimmunoassay Kits (Eurodiagnostica, Burgdorf, Switzerland) by Prof. Christoph Beglinger, University Hospital Basel, Switzerland.
Glucose homeostasis
Glucose was measured by an enzymatic UV-Test with a Cobas Mira analyzer (Roche, Switzerland) and insulin by an ultra-sensitive Human Insulin RIA Kit (Millipore).
Calculations
Homeostasis model assessment (insulin sensitivity: HOMA S=(glucose*insulin)/22.5); beta cell activity: HOMA B=(20*insulin)/(glucose-3.5)), fasting glucose to insulin ratio (G:I), and quantitative insulin sensitivity check index (QUICKI=1/((LOG(insulin))+(LOG(glucose)) were calculated by using the measured values of fasting insulin (mU/L) and fasting glucose (mmol/L) (Hung et al, 2011; Matthews et al, 1985).
Statistics
Statistical analysis was performed with Graphpad Software (San Diego California, USA). Power Analysis was done using G*Power Version 3.1.3. Some data were skewed and had different variances. To compare two groups on one test day, significance was determined by unpaired Students t-test with Welch's correction. For comparison of different test days within groups the Wilcoxon matched-pairs signed rank test was used. Two-way ANOVA with Bonferroni post-hoc tests were used to compare hormone and metabolite levels over the course of the day. Area under the curve (AUC) was calculated for various time periods for hormones with the value of the plasma sample “before muffin” set as baseline. AUC therefore indicates the changes in plasma levels relative to individual baselines. Odds ratios with confidence interval and Fisher's exact test were calculated to define the risk to develop AMS in subjects with baseline EPO plasma levels l< 6 mU/ml and a HOMA S level ≥2 at baseline at LA. In the case of HOMA S, one value equaled zero; 0.5 was therefore added to all values to make the calculation of the odds ratio possible. Significance was assumed with a p value≤0.05.
Results
Baseline characteristics
No significant differences were found between the dexamethasone-treated (DEX) and untreated groups (CON) in BMI, body weight, age, gender and in systolic, diastolic blood pressure and peripheral oxygen saturation on any test day. Heart rate was significantly higher in DEX compared to CON already at low altitude (p<0.05) and increased in the Capanna Margherita CON on HA2 (p<0.05) (Table 1). Eight out of the 25 subjects were known to have suffered from HAPE before.
Subjects divided in dexamethasone treated group (DEX) and control group (CON); table includes age, body weight (BW; kg), body mass index (BMI; kg/m2), systolic (SBP; mmHg) and diastolic blood pressure (DBP; mmHg), heart rate (HR, beats per min), hematocrit (HC; %), erythropoietin (EPO; mU/mL), peripheral oxygen saturation (SPO2; kPa). LA, low altitude, Zurich, baseline; HA2: day 2 and HA4: day 4 at high altitude at the Capanna Regina Margherita.
Values are means±SD; * indicates a significant difference to control at the same day, § indicates a significant difference within the same group to baseline in ZH; §,*: p<0.05, §§,**: p<0.01, §§§,***: p<0.001.
Hypoxia and clinical high altitude illness
Both groups decreased their arterial P
Lake Louise Score (LLS) was increased in both groups on HA2 compared to LA (p<0.01) and tended to be higher in HA2DEX compared to HA2CON (p=0.07). On HA4 LLS decreased but the effect was only significant in the dexamethasone-treated group (p<0.05 for HA2DEX vs. HA4DEX; p=0.16 for HA2CON vs. HA4CON). In both groups LLS remained higher on HA4 compared to LA (p<0.05) (Fig. 2A).
As expected, plasma EPO levels were increased in all subjects on HA2; EPO then decreased somewhat from HA2 to HA4, but remained higher on HA4 compared to LA (HA2CON and HA4CON to LACON, p<0.01; HA2DEX and HA4DEX to LADEX, p<0.001). EPO levels decreased from HA2 to HA4 in both groups, but were lower in HA4DEX than in HA4CON (p<0.05) (Table 1). Unexpectedly, EPO levels were lower in the dexamethasone-treated group than in the untreated control group at baseline in LA (p<0.05) (i.e., before any dexamethasone treatment) (Table 1). The odds ratio for the risk of suffering from AMS for subjects with EPO levels<6 mU/mL at baseline in LA was 10.5 with a confidence interval (CI) of 1.36–81.09 and a p value of 0.03 in the Fisher's exact test.
Blood metabolites and insulin
Plasma glucose concentration was higher in HA4DEX than in HA4CON at most time points of the day (p<0.001 morning, before muffin, 60, 90 min after muffin; p<0.01 30 min; p<0.05 120, 180, 240 min) (Table 2). Fasting glucose levels were increased in HA4DEX compared to LADEX (p<0.001) and HA4CON (p<0.001) (Fig. 3A). Other metabolites including betahydroxybutyrate, triglycerides, free fatty acids, and lactate were also determined but did not differ significantly across groups (data not shown).
Plasma levels±standard deviation of glucose (mmol/L), insulin (pmol/L) and CCK (pmol/L) in Zurich (LA) and on Day 2 (HA2) and Day 4 (HA4) at high altitude, measured nine times each day and separated retrospectively into two groups (dexamethasone-treated (DEX) and control group (CON)).
Indicates significant differences between HA4CON and HA4DEX; § indicates significant differences between LACON and LADEX; §, *: p<0.05, §§,**: p<0.01, §§§, ***: p<0.001.
Retrospective analysis of baseline data at LA indicated that plasma insulin was higher in DEX compared to CON at 60 min (p<0.01). Comparison of the study throughout the days within groups showed no significant difference at any time point in CON, but insulin was higher in DEX on HA2 compared to LA 30 and 60 min postprandially (pp) (Table 2, p30<0.001, p60<0.01). We observed an overall effect of dexamethasone and altitude in HA4DEX compared to LADEX (p<0.001), but did not detect a significant difference between time points. HA4DEX had higher levels at 30 and 60 min than HA2DEX (p<0.001). Insulin levels were higher in HA4DEX than in HA4CON after the test meal and just before dinner (p<0.001 60, 90 min pp; p<0.01 30, 120 min pp; p<0.05, 180 min pp, before ad lib) (Table 2). Figure 3B represents fasting insulin levels taken before breakfast and demonstrates higher levels in LADEX compared to LACON (p<0.01) and in HA4DEX compared to HA4CON (p<0.001).
The AUC of insulin was smaller in HA2DEX than in LADEX at the time points 30, 60 and 90 min (p30<0.05, p60<0.01, p90<0.05), and greater in HA4DEX than in LADEX at the time points 120, 180 and 240 min (p120<0.05, p180<0.01, p240<0.001). At 180 min HA4CON was greater than LACON (p<0.05). At the time points 180 and 240 min, the AUC of insulin was greater in HA4DEX than in HA4CON (p<0.05) (data not shown).
Assessment of insulin sensitivity
Calculation of homeostasis model assessment (HOMA) levels indicated that HOMA S levels were high and therefore insulin sensitivity was lower in HA4DEX than in HA4CON (p<0.001). While this effect was expected considering the known effect of dexamethasone on glucose metabolism, it is remarkable that insulin sensitivity also was lower in LADEX compared to LACON (p<0.01) (i.e., already at baseline before any treatment). The odds ratio for the risk of developing AMS for subjects with HOMA S baseline levels in LA ≥2 was calculated as 22.5 with a confidence interval of 1.1–480.3 and p=0.014 in the Fisher's exact test. HOMA S increased in HA2CON compared to LA (p<0.05) and in HA4DEX compared to LA (p<0.01) (Fig. 3C). Eight of the DEX subjects had prior episodes of HAPE but HOMA S values did not differ between DEX subjects with or without prior HAPE episodes (results not shown). Beta cell activity (HOMA B) remained unchanged. Fasting glucose to insulin ratio (Fig. 3D) was lower in LADEX and HA2CON compared to LACON (p<0.05, p<0.01) and also lower in HA4DEX than in HA4CON (p<0.05). QUICKI values were significantly lower in LADEX and HA2CON than in LACON (p<0.05) and lower in HA4DEX compared to LADEX and HA4CON (p<0.01, p<0.001) (Fig. 3E).
Inflammation markers and cortisol
Endogenous cortisol was measured as an internal treatment control standard in all individuals before and after medication with dexamethasone (Fig. 2B). As expected, endogenous cortisol was markedly lower after treatment (HA4DEX vs. HA4CON, p<0.001). Retrospective analysis indicated, however, that endogenous cortisol did not differ between groups in LA or at HA2; in other words, endogenous cortisol was only suppressed in dexamethasone-treated participants. Based on similar cortisol levels on HA2 and LA in both groups, the ascent on Days 0 and 1 had no influence on HA2.
Plasma IL-6 concentrations increased in both groups on HA2 compared to LA (CON, p<0.05, DEX, p<0.01). IL-6 tended to be lower on HA4 than on HA2, but this difference was only significant in the control group (p<0.05) and not in the dexamethasone-treated group (HA2DEX vs. HA4DEX, p=0.07) (Fig. 2C). Plasma TNF-α levels were lower in HA4DEX than in HA4CON (p<0.05) (Fig. 2D).
CCK and amylin
Plasma levels of amylin did not differ at individual time points across groups (i.e., there was no effect of either hypoxia or dexamethasone treatment). Amylin and CCK increased as expected after the muffin test meal in both groups and on all days. (Table 2)
Interestingly, CCK levels were lower in HA4DEX compared to HA4CON 30 min (p<0.05) and 60 min (p<0.01) after the test meal (Table 2). The AUC of CCK was also smaller in DEX compared to CON on HAH2 30, 60, and 90 min after the test meal (p<0.05). The AUC was greater in HA4CON compared to LA 30, 60 and 90 min postprandially (p30<0.01, p60<0.01, p90<0.05); compared to HA4DEX, it remained higher over all time points after the muffin test meal (before breakfast p<0.05, all other time points p<0.01) (data not shown).
Amylin had a greater AUC at HA2 in CON 30 and 60 min after the muffin test meal (p<0.05). Ninety to 240 min after the muffin the AUC of amylin was greater in CON at HA2 than on LA(p<0.001) (data not shown). Similarly, we also measured PYY and gastrin over the course of the study but did not detect any differences among groups (data not shown).
Caloric intake ad libitum dinner
Energy intake (kcal) during the ad libitum dinner was lower in DEX on all three days (p<0.05) and was decreased in both groups on HA2 compared to LA (LACON vs. HA2CON p<0.01; LADEX vs. HA2DEX p<0.05). Energy intake returned to nearly baseline levels on HA4 (HA2CON vs. HA4CON, p<0.05; HA2DEX vs. HA4DEX, p<0.01) (Fig. 4).

Food intake at ad libitum dinner (CON=9, DEX=12). § indicates significant differences within the groups between different test days, tested with Wilcoxon matched-pairs signed rank test; * indicates significant differences between groups on the same test day, tested with unpaired Students t test with Welch's correction. §, *: p<0.05; §§, **: p<0.01; §§§,***: p<0.001. Error bars represent standard error of the mean. LA, Zurich, baseline; HA2, Day 2, and HA4: Day 4 at the Capanna Regina Margherita.
Taken together, our findings indicate that baseline insulin sensitivity and baseline EPO levels were lower in individuals at risk of AMS; these individuals required dexamethasone treatment in the evening of HA2 as they developed AMS.
Discussion
Our main goal was to study specifically the effects of AMS on pre- and postprandial metabolism of a caloric solid meal. We were also interested in side effects of dexamethasone treatment on metabolism in AMS-prone patients when exposed to high altitude-induced hypoxia. Our results did not only confirm the expected effect of dexamethasone on glucose homeostasis but also revealed differences between the dexamethasone and control groups in plasma EPO levels and insulin sensitivity already at baseline in Zurich (i.e., at low altitude and before treatment with dexamethasone).
The clinical appearance of AMS, as reflected by the Lake Louise Score (LLS), was induced by the fast ascent to high altitude with an increase on HA2 and a decrease due to acclimatization on HA4 in both groups as expected (Jackson et al, 2010; Leshem et al, 2008). The prevalence of 57% of AMS in our subjects lies within the upper range of the data reported by other groups that found a prevalence of 30%–60% at altitudes between 4243 m and 5671 m (Basnyat et al, 1999; Jackson et al, 2010; Maggiorini et al, 1990; Ziaee et al, 2003). This may be due to the fast ascent and to the inclusion of eight subjects with known HAPE susceptibility. The decrease in LLS on HA4 after dexamethasone clearly shows the effective improvement in well-being of the subjects who suffered from AMS but were successfully treated with dexamethasone, as it has been reported previously (Subudhi et al, 2011).
Endogenous cortisol was measured and analyzed to prove dexamethasone's efficacy. The suppressive effect of dexamethasone on endogenous cortisol production was as expected (Findling et al, 2004; Miller et al, 1992): the dexamethasone-treated group showed a marked decrease in the plasma levels of endogenous cortisol at HA4. Hence, the medication of the individuals suffering from AMS was considered effective.
Cytokines
Consistent with other studies, the plasma concentration of IL-6, but not of the other cytokines, increased due to exposure to high altitude hypoxia (Hartmann et al, 2000; Klausen et al, 1997). Plasma IL-6 and TNF-α decreased in the dexamethasone-treated group on HA4, an expected observation due to the anti-inflammatory effect of dexamethasone.
EPO
Erythropoietin expression is upregulated by hypoxia (Eckardt et al, 1989). As expected, plasma EPO levels therefore increased on HA2 after the fast ascent. Endogenous EPO has a relatively short plasma half-life of 6–9 hours (Eckardt et al, 1989). Our results therefore suggest that the EPO production was still higher on HA4 compared to LA but lower compared to HA2. The significantly lower EPO plasma level in the dexamethasone-treated group on HA4 can be explained by the effect of dexamethasone on gene transcription of cytokines via the glucocorticoid receptor (Amano et al, 1993; Newton et al, 2010; Smith et al, 2001). Hypoxia inducible factor (HIF) enhances EPO gene transcription in response to hypoxia (Wang and Semenza, 1995), and others showed in cultured cells that dexamethasone suppresses the expression of HIF (Gaber et al, 2011). Unfortunately this effect interferes with the acclimatization to high altitude hypoxia and, hence, contributes to the necessity to descend in case of AMS despite medication with dexamethasone. Further possible influences on plasma EPO levels such as EPO clearance from blood have not well been investigated yet.
In apparent contrast to our study, Pavlicek et al. (2000) reported no difference in baseline levels but a significantly higher EPO plasma level in HAPE susceptible subjects at high altitude. Of note, one of the inclusion criteria for our study was that the subjects were not allowed to spend more than 3 nights at 2500 m or higher one month prior to the study, but we did not completely exclude activities at altitude. Altitude activities prior to the study and a better general state of physical fitness may have lead to the slightly but significantly higher EPO levels at LA in the group that did not suffer from AMS (Frese and Friedmann-Bette, 2010). However, another study (Siebenmann et al, 2011), which also included some of the subjects who participated in our experiments, found that V
Glucose metabolism
Glucose metabolism was affected by dexamethasone on HA4 as expected. Dexamethasone has been shown to increase glucose levels in other studies (Marquet et al, 1999). We could not confirm, however, the increased glucose levels due to hypoxia or AMS itself reported by Larsen et al. (1997). Glucocorticoids affect glucose metabolism in several ways: they impair insulin-dependent glucose uptake in the periphery and enhance gluconeogenesis in the liver (Rizza et al, 1982; Rooney et al, 1993). Our data show that glucose and insulin levels increased and, hence, insulin sensitivity decreased after dexamethasone treatment on HA4, which was expected (Abdelmannan et al, 2010). No significant changes due to hypoxia could be seen on HA2. Surprisingly, however, we found a lower insulin sensitivity in Zurich at baseline—which has to be clearly differentiated from diagnosed diabetes—in the subjects that later suffered from AMS and had to be treated with dexamethasone. This may be an indication of higher susceptibility of those individuals for AMS. We did not evaluate the subjects with respect to any hereditary predisposition for diabetes. Of note Henriksen et al. (1999) showed that dexamethasone differentially alters muscle glucose metabolism of normoglycemic relatives of type 2 diabetic patients. It has to be considered that six volunteers who reported at least one incidence of HAPE in history were included in the dexamethasone-treated group. As it has been shown that HAPE susceptibles have an elevated baseline sympathetic tone (Duplain et al, 1999), this seems also to be the case for AMS-prone individuals (Lanfranchi et al, 2005; Loeppky et al, 2003). Because it is well known that autonomic nervous system activity has a strong impact on the control of glucose (Porte and Williams, 1966; Shimazu, 1967; Walter et al, 1974), we considered that these processes might have an impact on our studies, in particular as baseline heart rate at LA was increased in DEX compared to CON. The known effect of dexamethasone on glucose metabolism and the autonomic nervous system might partly explain the effect of dexamethasone on AMS (Scherrer et al, 1993). Note that we did not analyze parameters of the autonomic nervous system in this study, and thus we cannot evaluate our findings regarding those aspects. The lower plasma EPO levels in the dexamethasone-treated group already at baseline may also contribute to reduced insulin sensitivity because it has been shown that EPO improves glucose tolerance in mice by changing muscle metabolism (Foskett et al, 2011; Julian et al, 2011; Maggiorini et al, 1990), and because EPO treatment of anemia in uremic patients improved insulin resistance and alleviated hyperinsulinemia (Mak, 1996). HIF plays an important role in glucose metabolism under hypoxic conditions (Cheng et al 2010), but this effect may be impaired by dexamethasone treatment (Gaber et al 2011). It has been shown that HIF activation in heart muscle of diabetic patients is impaired (Heather and Clarke 2011), but our subjects were less insulin sensitive even though not as insulin resistant as when suffering from diabetes. So far, there is no evidence for an impaired HIG expression in subjects prone to AMS (Ding et al, 2011; Droma et al, 2008).
Insulin sensitivity is impaired in patients with metabolic syndrome, but other symptoms such as increased blood pressure or higher BMI did not appear to be prevalent in our subjects (Salazar et al, 2011). Although they did not yet show any obvious symptoms of diabetes or even overt changes in blood glucose levels, people predisposed for diabetes may have more difficulties to handle those side effects of dexamethasone because they aggravate their insulin resistance that might have been undetected before. Therefore, we analyzed insulin sensitivity by different models using fasting insulin and glucose levels, but all yielded consistent findings. We did not perform hyperinsulinemic-euglycemic clamps or oral glucose tolerance tests in our study. Another possible indicator for assessing the blood glucose concentration over a longer period of time is glycated hemoglobin (HbA1c) (Borges et al, 2011; Heianza et al, 2011). Nevertheless, we are convinced that the calculations of HOMA, QUICKI, glucose to insulin ratio combined with the values of fasting insulin are helpful and reliable indices to assess insulin resistance (Hung et al, 2011; Matthews et al, 1985; McAuley et al, 2001).
Hormones
Plasma CCK levels of HA4CON tended to be higher at one time point (30 min postprandially) compared to LA and HA2, but this difference did not reach statistical significance. We could therefore not confirm the increase in resting plasma CCK that Bailey et al. found at high altitude (Bailey et al, 2000). The AUC revealed a significantly higher increase of CCK in HA4CON compared to LA and HA4DEX, which may indicate that hypoxia could still have had some influence. This finding, combined with the significantly lower levels in HA4DEX compared to HA4CON, confirms an effect of dexamethasone on CCK levels similar to what had already been reported by Ratineau et al. in both cell culture and rat experiments (Ratineau et al, 1996). Therefore, the decrease in CCK may play a role in the improvement of AMS-associated anorexia after dexamethasone treatment.
Although we found no significant difference at single time points in amylin plasma levels that would implicate an effect of hypoxia or dexamethasone, we observed significant differences in the postprandial AUC. The AUC revealed that amylin increased more in HA2CON compared to HA2DEX at the time points 30 and 60 min and compared to LACON for the time points 90, 120, 180, and 240 min. Therefore, the food intake induced amylin response seems to be different in subjects at high altitude compared to sea level and compared to subjects suffering from AMS. This needs to be further investigated but at least our data suggest that dexamethasone has no effect on amylin plasma levels.
Caloric intake
The overall effect of hypoxia on eating, in particular the significant decrease of caloric intake during the ad libitum dinner in both groups on HA2 confirms the results of earlier studies (Lippl et al, 2010; Westerterp-Plantenga et al, 1999). The increase in caloric intake back to nearly baseline (LA) levels in both groups on HA4 was probably due to acclimatization and the dexamethasone treatment in the DEX group (Bruera et al, 2004). Subjects at risk for AMS (DEX) ate less than the control group on all three testing days. As we did not measure hormone levels and metabolites during and after the ad libitum dinner, potential mechanisms need to be tested in future studies. For detailed analysis of caloric intake in our test subjects, please see Aeberli et al. (2012).
Finally, some limitations of our study need to be mentioned. First, medication was not blinded and we had no placebo control group included due to the primary endpoint of this large-scale study. In other words, any individual who required dexamethasone treatment due to medical condition and development of AMS received the drug. The other individuals remained untreated. Nonetheless, we believe that the main conclusion of our study (i.e., that low insulin sensitivity may predispose for AMS when exposed to hypoxia), is interesting and remains valid; all the data were analyzed retrospectively so that there was no bias as to the data at baseline in patients who later required dexamethasone treatment. Second, due to the design of the study and the experimental conditions including the available infrastructure at high altitude, we did not carry out oral glucose tolerance tests or hyperinsulinemic-euglycemic clamps that would have permitted stronger conclusions concerning the state of glucose metabolism. Third, due to some technical difficulties in blood sampling under field conditions and analysis, the group size (n) for some parameters is rather small.
In summary, our results provide evidence indicating that dexamethasone in the treatment of AMS has not only positive effects on inflammation and altitude anorexia, but also carries the risk of a potentially dangerous influence on glucose metabolism, in particular as our data indicate that individuals with decreased insulin sensitivity may be more susceptible to AMS. Finally, this study emphasizes a clear need for further investigation and reminds the reader that dexamethasone is a potent drug but, due to the numerous possible side effects, also potentially dangerous, when taken at high altitude.
Footnotes
Acknowledgments
Special thanks go to the subjects who volunteered to participate in our study. We also want to thank Beat Grenacher, Institute of Veterinary Physiology, and Barbara Schneider, Institute of Animal Nutrition, University of Zurich, and Prof. Christoph Beglinger, University Hospital Basel, for their help with blood sample analysis.
Author Disclosure Statement
None of the authors has any conflict of interest with regard to this article.
This study was supported by the Zurich Centre for Integrative Human Physiology (ZIHP).
Author contributions: Kerstin Spliethoff: laboratory sample analysis, data processing, statistical analysis, article writing; Daniela Meier: laboratory sample analysis; Isabelle Aeberli: food intake study; Max Gassmann: initiator of this project, study design, article writing; Wolfgang Langhans: study design, article writing; Marco Maggiorini: study design, medical examinations, medical treatment; Thomas A. Lutz: initiator of this project, study design, statistical analysis, article writing; Oliver Goetze: study design, blood sampling, medical examinations, article writing.