
Abstract
Abstract
Fraidenburg, Dustin, Jason Yuan. Current and future targets for pulmonary arterial hypertension. High Alt Med Biol 14:134–143, 2013.—Pulmonary arterial hypertension (PAH) remains a poorly understood disorder with dire consequences. Progression of disease often leads to right heart failure and death without lung transplantation. Limited therapeutic strategies exist for the treatment of PAH and current medical treatment consists of two major categories, supportive care therapeutics and pulmonary vasculature targeted therapy. Supportive care includes anticoagulants and inotropic agents, while pulmonary vasculature targets currently available include endothelin antagonists, phosphodiesterase inhibitors and prostacyclin analogs. While these therapies have shown efficacy in hemodynamic and functional outcomes; halting the progression of disease, reversal, and clinical cure has been elusive. Combination therapy and newer agents may provide innovative insight into the disease process and ultimately change the prognosis of this fatal disease. By utilizing specific targets on the cell membrane, second messengers systems or signaling peptides, novel therapeutic strategies will hopefully emerge. In this review we discuss the currently available therapeutic options and their pulmonary vasculature targets as well as some future therapeutic targets that have promising results in human trials.
Treatment of PAH can be broken down into supportive care therapeutics versus pulmonary vasculature specific therapy. Vasodilators, anticoagulants, and inotropes represent treatment used for many decades, and these treatments, particularly calcium-channel blockers, have been shown to improve pulmonary outcomes dramatically, but this effect is now understood to only benefit a small subset of PAH patients (Sitbon et al, 2005). Therefore, newer classes of agents have been designed and, over the past 20 years, three have emerged: prostacyclin analogs, endothelin antagonists, and phosphodiesterase type 5 inhibitors (see Table 1). These agents have been shown to improve hemodynamic measurements and markers of morbidity, including quality of life and functional capacity, yet only one agent, epoprostenol, has shown a clear mortality benefit (Jing et al, 2011). Though population studies have shown improved survival since the early 1980s, reversal or clinical cure still remains elusive (Benza et al., 2012). Newer agents in these classes with more specific targets, enhanced potency, or improved delivery are continually being developed, but it will likely take a novel agent before we can hope to improve the course of this disease.
A summary of efficacy data available from human trials with current therapeutic agents for PAH. CI, cardiac index; mPAP, mean pulmonary arterial pressure; NS, not significant; PVR, pulmonary vascular resistance.
Supportive Care
Anticoagulation
In situ thrombosis and microthrombi have been implicated in the disease pathogenesis of PAH. In one study, 38% of IPAH patients had evidence of thrombi after dissection, all with low probability V/Q scans or negative pulmonary angiograms (Pietra et al, 1989). Endothelial dysfunction, platelet activation, and abnormal plasma protein concentrations all likely contribute to the professed prothrombotic state and incidence of in situ thrombosis seen on histologic evaluation of PAH. Therefore, anticoagulation has been a mainstay of treatment and is recommended for all PAH patients unless contraindications exist.
Warfarin
A vitamin K antagonist, warfarin is the most common anticoagulant used in practice today and until recently was the only orally bioavailable anticoagulant. It is also the most commonly used anticoagulant for PAH. The evidence to support its use comes from multiple nonrandomized trials (Frank et al, 1997; Fuster et al, 1984; Rich et al, 1992). A survival benefit has been established for IPAH and because of the similarity with other forms of PAH, the recommendation for anticoagulation extends to all WHO group 1 patients. Expert opinion dictate goals of therapy are to maintain an international normalized ratio (INR) of 1.5–2.5 in IPAH, which is slightly lower than therapeutic strategies for venous thromboembolism and CTEPH, though individual treatment strategies need to evaluate the risk/benefit ratio for anticoagulation (McLaughlin et al., 2009).
Unfractionated and low molecular weight heparins, direct thrombin antagonists, and Factor Xa inhibitors
Currently, no controlled trials exist for these other classes of anticoagulants, though case series and clinical experiences have been reported. During pregnancy, warfarin is contraindicated and can produce serious deformities in the fetus; in these instances the use of various other anticoagulants has been employed. Low molecular weight heparins have been recommended in place of warfarin during pregnancy (Huang and DeSantis, 2007). A small case series of 5 pregnant women also highlights the successful use of Factor Xa inhibtors in PAH during pregnancy (Smith et al, 2012).
Aspirin and clopidogrel
A randomized, double-blinded, placebo controlled trial evaluated the effects of aspirin (ASA) and clopidogrel on PAH patients (Robbins et al, 2006). No significant change in symptoms with either clopidogrel or ASA therapy was observed, although both decreased platelet aggregation. Kawut et al. conducted a randomized, placebo-controlled study of 92 PAH patients to evaluate the symptomatic effects of ASA and simvastatin (Kawut et al, 2011). This study showed that 81 mg ASA had no effect on 6-minute walk distance at 6 months. Therefore, the routine use of these medications has not been encouraged.
Digoxin
Digoxin is used as an adjunctive agent for the treatment of left ventricular systolic dysfunction and cardiac dysrhythmia. Positive inotropy, normalizing baroreceptor responsiveness, and decreasing sympathetic overdrive are all thought to improve morbidity in left ventricular dysfunction. Similar dysfunction exists in severe PAH with right ventricular failure (i.e., cor pulmonale). Rich and colleagues were the first to tackle this issue, identifying 17 patients with severe PAH and right heart failure, prospectively looking at the effects of digoxin (Rich et al., 1998). They identified a significant increase in cardiac output without significant changes in baroreceptor responsiveness and inconclusive data regarding sympathetic nervous system effects. There have been no large, randomized trials with digoxin, and therefore its influence on morbidity and mortality remains unknown.
Dobutamine
Dobutamine is a positive inotrope that increases myocardial contractility and reduces vascular resistance in both the pulmonary and systemic circulation (Murali et al., 1991). Dobutamine has limited effect on vasomotor tone, with weak activity on both beta-2 and alpha adrenergic receptors. Pulmonary resistance changes represent the inverse relationship of resistance and flow, as experimental animal models show no flow-independent effects of dobutamine on the pulmonary circulation (Pagnamenta et al., 2003). Increased right ventricular (RV) contractility has been confirmed in mild pulmonary hypertension (Acosta et al., 2005). It is often employed as a first-line therapy for patients with acute right heart failure. In one study of patients with PAH and acute right ventricular failure, survival was independently associated with lower requirements of dobutamine (Sztrymf et al., 2010). This agent is dispensed as a continuous intravenous infusion, therefore it remains a mainstay of inpatient treatment, but its utility in the outpatient setting is very limited.
Statins
The first observations published regarding HMG-CoA reductase inhibitors showed that simvastatin alone or in combination with calcium channel blockers or prostacyclin treatment may improve functional capacity in a small number of patients (Kao, 2005). Prospective, placebo-controlled studies of various statins has followed, but have been unable to show any significant improvement in morbidity or mortality (Barreto et al., 2008; Wilkins et al., 2010; Zeng et al., 2012). Though the data have been strong in animal models, it appears that statins alone or in combination with effective therapy for PAH has little, if any, short-term effects and long-term effects remain unknown.
Targeted Therapy
The pulmonary vasculature represents a unique environment with mechanisms that are distinctive from the systemic circulation. Therefore, cellular and molecular pathways common throughout the human body have distinct roles in the pulmonary circulation. By understanding and exploiting these pathways in the pulmonary vasculature, therapeutic approaches have been created for the treatment of PAH. Membrane receptors, second messengers, and signaling peptides all play essential roles in the pathogenesis of PAH and have the opportunity to become therapeutic targets.
Targeting Membrane Receptors (Fig. 1)
Calcium channel blockers
Vasodilator therapy has been used for nearly three decades to treat PAH. Calcium-channel blockers (CCBs) represent the first, well-accepted vasodilators for the treatment of PAH, with non-dihydropyridines being the most common class, particularly nifedipine and diltiazem. In order to establish safety and efficacy with this class of medications, pulmonary vasodilatory testing has been utilized (Sitbon et al., 1998). Using a very short-acting vasodilatory agent, most commonly inhaled nitric oxide (NO), reversible vasoconstriction can be differentiated from fixed stenosis in patients with PAH. A change in mean PAP of >10 mmHg to an absolute mPAP <40 mmHg without a significant decrease in cardiac output indicates a positive test (Sitbon et al., 2005). Initial studies that used slightly different criteria indicated up to 90% of patients with a positive vasoreactivity test had favorable response acutely to CCBs, where adverse reaction from CCB was seen in 38% of nonresponders (Sitbon et al., 1998). There still remains limited utility of these medications, as recent data have shown a very small proportion of IPAH patients, <10%, will have acute vasoreactivity, and of these patients, only about half will have long-term response to calcium channel blockers (Sitbon et al., 2005).
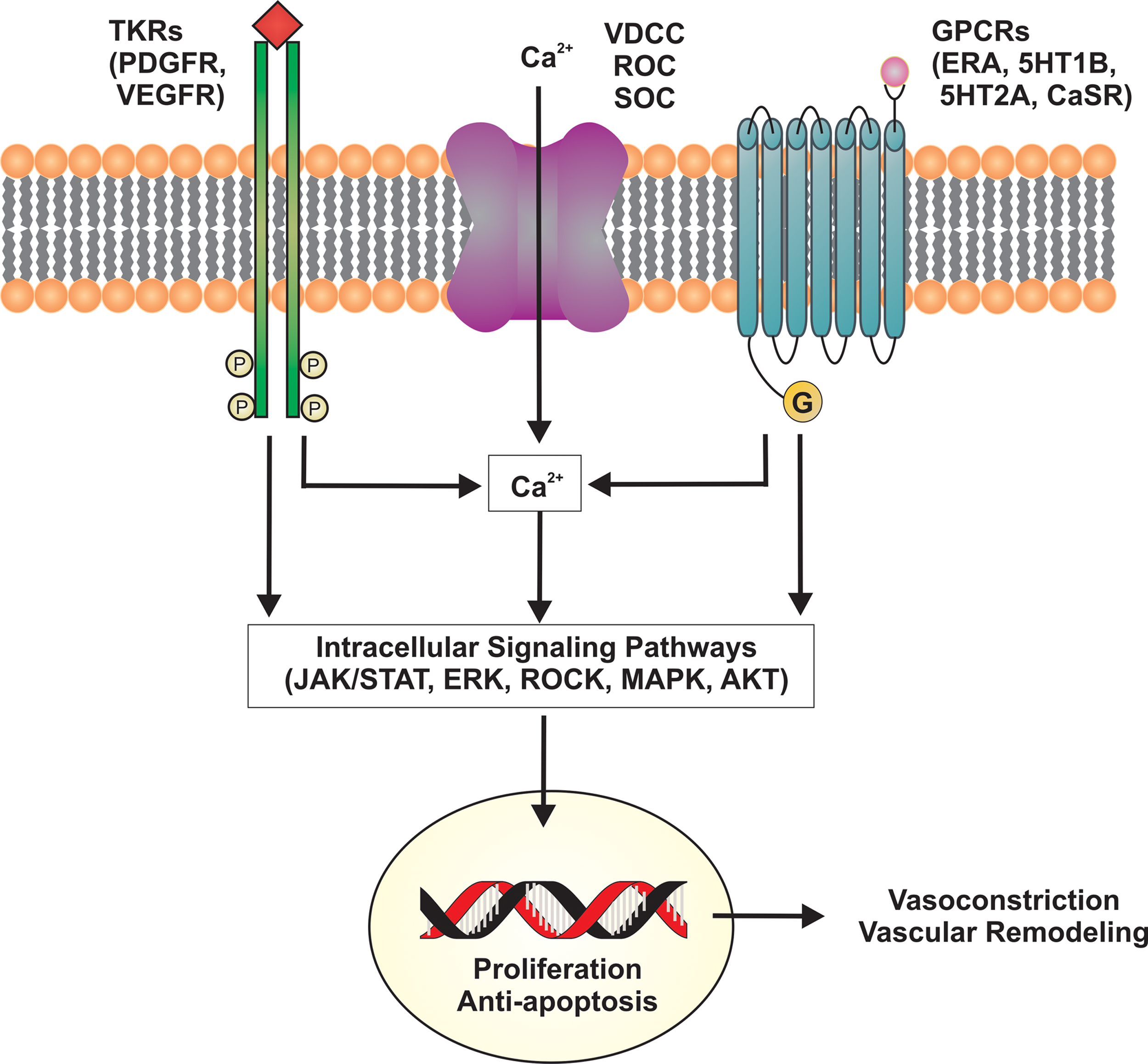
Cell membrane receptors and ion channels targeted in the treatment of PAH. Ca2+, calcium; CaSR, calcium sensing receptor; ERA, endothelin receptor antagonists; ERK, extracellular signal-regulated kinase; GDP, guanosine diphosphate; GPCRs, G-protein coupled receptors; GTP, guanosine triphosphate; 5HT2A, serotonin receptor type 2A; 5HT1B, serotonin receptor type 1B; JAK, Janus kinase; MAPK, mitogen-activated protein kinase; PDGFR, platelet-derived growth factor receptor; ROC, receptor-operated calcium channel; ROCK, rho-associated protein kinase; SOC, store-operated calcium channel; STAT, signal transducer and activator of transcription; TKR, tyrosine kinase receptor; VDCC, voltage-gated calcium channel; VEGFR, vascular endothelial growth factor receptor.
Endothelin receptor antagonists
Endothelin (ET-1) plays a central role in the pathogenesis of PAH through endothelial dysfunction and vascular remodeling. Mainly synthesized in endothelial cells, but also described in vascular smooth muscle cells, ET-1 activation has its primary effect as a vasoconstrictor; it also increases VSMC proliferation and decreases apoptosis (Yanagisawa et al., 1998; Levin, 1995). Both PAH and HAPH patients have been shown to have elevated levels of circulating ET-1, which stimulates both ET-A and ET-B receptors (Giaid et al., 1993; Kojonazarov et al., 2012). ET-A receptors, located on PASMC, are thought to be the primary driver of the vasoconstrictive effect (Seo et al., 1994), while ET-B receptors are primarily located on endothelial cells and have vasodilatory effects (Hirata et al., 1993), although evidence also exists for vasoconstrictive downstream targets of ET-B, including thromboxane A2 (Dupuis et al, 1996). The above findings have led to the development of therapeutic strategies with endothelin receptor antagonists (ERA) for PAH, which has recently been expanded to the treatment of HAPH (Kojonazarov et al., 2012). The first agent, bosentan, is a dual ERA with effects on both ET-A and ET-B receptors, while newer agents are specific ET-A receptor antagonists, thought to block ET-A receptor-mediated vasoconstriction while maintaining the vasodilatory ET-B receptor response.
Hepatotoxicity remains the major adverse effect of the class, and though specific ET-A receptor antagonist, ambrisentan, has shown less significant elevation of liver function tests (Galie et al., 2008); a previous specific ET-A receptor antagonist was recently removed from the world market after life-threatening hepatic failure was reported, thought to be an immune or idiosyncratic reaction (Lavelle et al., 2009; Galie et al., 2011). Macitentan, a new dual endothelin receptor antagonist, is hoped to improve tissue targeting by increasing the lipophilic nature of the compound that allows once daily dosing and may also improve liver toxicity (Siharta et al., 2011). The FDA has recently announced the drug's approval, and results of a phase 3 trial are expected soon.
Serotonin receptor
Serotonin has been implicated in pulmonary hypertension pathogenesis since the first reports of stimulant medications causing PAH. Serotonin receptors, particularly 5HT1B, have both direct effects on vascular contraction, as well as indirect effects on contraction and proliferation through ROS, rho-associated protein kinase (ROCK), and extracellular signal-regulated kinase (ERK) upregulation (Dempsie and McLean, 2008). The serotonin receptor has also been found to be overexpressed in IPAH patients and is thought to play a synergistic role (MacLean and Dempsie, 2010; Marcos et al., 2004). A 5HT receptor antagonist, terguride, has not shown the promising results that were hoped for in PAH treatment, though the utility of this pathway as a therapeutic target will likely continue to be important (Ghofrani et al., 2010).
Tyrosine kinase inhibitors
Imantinib was initially developed as targeted treatment for chronic myelogenous leukemia by targeting the ABL tyrosine kinase receptor, though the compound is known to have many other targets. The target that is most interesting in PAH is platelet-derived growth factor (PDGF) and its receptor that has been linked to vascular smooth muscle hypertrophy, possibly promoting the development of PAH (Humbert et al., 1998). Imantinib as add-on therapy for refractory PAH has shown efficacy in a recently presented oral abstract, though serious adverse reactions were more common with imantinib treatment (Hoeper et al., 2011). Whether toxicity can be mitigated with newer agents or tolerated given the severity of patients being treated remains a question that should be considered before this medication can be widely incorporated into PAH treatment regimens.
Targeting Second Messengers (Fig. 2)
Phosphodiesterase inhibitors
The cyclic guanosine monophosphate (cGMP) pathway is an important target of endothelium-derived nitric oxide, an essential vasodilatory agent (Sausbier et al., 2000). Phosphodiesterase type 5 (PDE5) rapidly hydrolyzes cGMP, inactivating its vasodilatory effects. PDE5 inhibitors have been developed that prolong the effect of cGMP by inhibiting its degradation. Sildenafil has been the first commercially available PDE5 inhibitor for the treatment of PAH. Early trials were able to show both acute hemodynamic improvements and long-term beneficial effects on hemodynamic measurements and exercise capacity (Ghofrani et al., 2002; Galie et al., 2005). Small trials have also shown sildenafil to be an effective treatment for high-altitude pulmonary hypertension, and it may also attenuate mPAP increases in normal subjects exposed to high altitude, though other trials have failed to validate this effect in normal subjects (Aldashev et al., 2005; Richalet et al., 2005; Bates et al., 2011). Oral formulation makes these agents attractive as first-line treatment of PAH, and subsequent PDE5 inhibitors have been developed with enhanced pharmacokinetics that improve duration of action and potency (Galie et al., 2009; Rosen and Kostis, 2003; Jing et al., 2001). Adverse effects of the class are minor, with headache, edema and renal dysfunction being the most common.

Second messengers targeted in the treatment of PAH. cGMP, cyclic guanosine monophosphate; cGTP, cyclic guanosine triphosphate; GMP, guanosine monophosphate; NO, nitric oxide; PDE-5, phosphodiesterase type 5; PKG, phosphokinase G; ROCK, rho-associated protein kinase; ROS, reactive oxygen species; sGC, soluble guanylate cyclase.
Soluble guanylate cyclase
Soluble guanylate cyclase converts guanosine triphosphate (GTP) to cGMP, leading to vasorelaxation. Stimulation of soluble guanylate cyclase by a new agent, riociguat, has shown efficacy in small PAH patient populations (Grimminger et al., 2009; Ghofrani et al., 2010). Randomized, placebo-controlled trials have recently been completed, and oral abstracts have indicated positive results in both PAH and CTEPH patients, leading to an FDA drug submission for approval in the United States (Ghofrani et al., 2012a; 2012b).
Rho/Rho-kinase
The Rho/Rho-kinase pathway is an attractive target in PAH because it acts on several components in the pathogenesis of PAH, including vasoconstriction through NO and calcium sensitization, vascular remodeling through cell proliferation, and inhibition of apoptosis, as well as in situ thrombosis through platelet activation (Fukumoto et al., 2007). Fasudil, a nonspecific ROCK inhibitor, has encouraging results from early human trials, particularly in high-altitude related pulmonary hypertension (Fujita et al., 2010; Kojonazarov et al., 2012).
Targeting Signaling Peptides (Fig. 3)
Prostacyclin analogs
Prostacyclin (PGI2) plays an important role in vasodilation, as well as inhibition of vascular smooth muscle cell proliferation and migration. A product of the metabolism of arachidonic acid, PGI2 binds to the prostacyclin receptor (IPR) on PASMC leading to increased levels of cyclic adenosine monophosphate (cAMP), which promotes vasodilation and antiproliferative effects (Olschewski et al., 2004); as well as having effects on various other cell lines including platelet inhibition. Decreased prostacyclin release has been shown in PAH patients, which is thought to contribute to the pathogenesis of PAH (Christman et al., 1992). Epoprostenol was the first prostacyclin formulation. Initial hemodynamic studies of intravenous infusion in PAH patients showed a dose-dependent decrease in PVR along with increased cardiac output (Rubin et al., 1982). This led the use of epoprostenol as a prognostic indicator of favorable response to traditional vasodilators; although, because of its short duration of action (half-life of 6 minutes) and intravenous formulation, it was not routinely used as a therapeutic agent until a decade later. At that time, continuous intravenous infusion of epoprostenol compared to traditional therapy in PAH patients showed a significant improvement in both exercise capacity and hemodynamic measurements (Barst et al., 1996). Survival in the epoprostenol group was 100% compared to 80% in the conventional therapy group over a 12-week period, an effect not seen with previous agents and not duplicated with any other currently available therapeutics. Common side effects of the class include flushing, diarrhea, HA, jaw pain, nausea, and vomiting. Intravenous epoprostenol remains a mainstay of treatment in the most severe PAH patients.
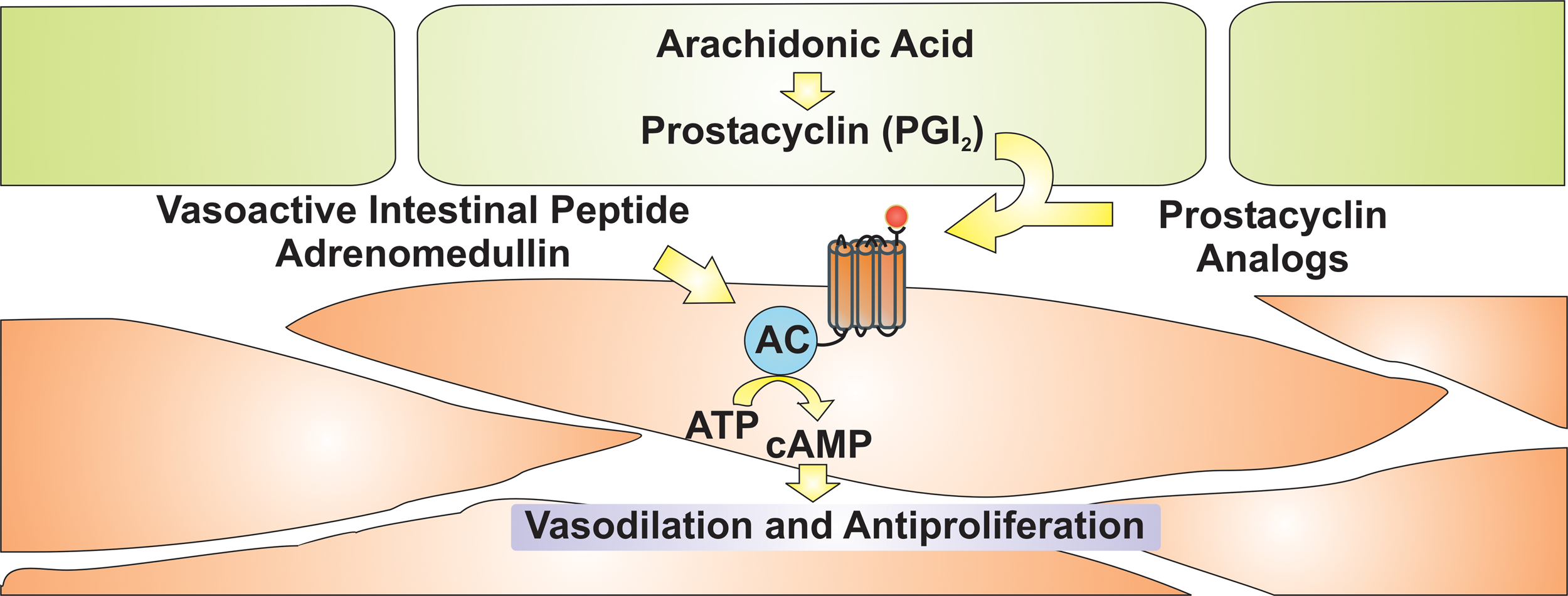
Prostanoids, vasodilatory, and antiproliferative peptides for treatment of PAH. AC, adenylate cyclase; ATP, adenosine triphosphate; cAMP, cyclic adenosine monophosphate.
Complications of continuous intravenous administration led to development of agents with more favorable formulations. The first prostacyclin analog to be available as an inhaled formulation, iloprost was designed to target the pulmonary vasculature with minimal systemic side effects. Initial pharmacodynamics evaluation showed improvement in mean pulmonary artery pressure and cardiac output after a single dose (Olschewski et al., 1996). Long-term treatment improved exercise capacity and hemodynamic measurements which were sustained for one year (Hoeper et al., 2000). Newer delivery systems have improved the duration of action, requiring less frequent dosing (Gessler et al., 2001).
Intravenous treprostinil improved on the initial pharmacodynamics of epoprostenol by increasing the half-life, allowing time for troubleshooting in the case of pump malfunction, though significant adverse events, including bacteremia and death, still occurred (Hiremath et al, 2010). Continuous subcutaneous delivery of this medication decreased the risk of bacteremia but was associated with frequent infusion site reactions (McLaughlin et al., 2003). An inhaled formulation also is available, with improved delivery by metered dose inhaler (Voswinckel et al., 2009), and the many formulations allow more options to both care providers and patients.
Oral formulations of prostacyclin analogs have had less success than other preparations. An oral formulation of treprostinil was unable to show efficacy, though it was proposed that dose-related complications could be mitigated in future trials (Tapson et al., 2012). Beraprost was the first orally available prostacyclin analog and initial studies showed mixed results, while a long-term U.S. study was unable to show efficacy at 12 months (Barst et al., 2003). As a result of this study, beraprost has not been approved by the FDA.
Selexipag is a new agent in the prostacyclin class, though its mechanism is distinct from all previous agents. It is an orally bioavailable, selective prostacyclin receptor agonist rather than prostacyclin analog and therefore has a much lower affinity for prostaglandin receptors, which are thought to produce some of the side effects associated with this class (Morrison et al., 2010). Early data have shown improvement in pulmonary hemodynamics and a phase 3 trial is in progress (Simonneau et al., 2012).
Vasoactive intestinal peptide
Vasoactive intestinal peptide is a ubiquitous hormone that mediates several pathways throughout the human body; it has been linked to vasorelaxation through cAMP and cGMP pathways, which are similar to current treatment strategies of prostacyclin and PDE5 inhibitors. Aviptadil, an inhaled vasoactive intestinal peptide analog had shown early promise, yet the most recent results of a large, multicenter clinical trial has failed to show efficacy (Leuchte et al., 2008; Galie et al., 2012). Whether changes in formulation, delivery, or dose can achieve the desired effect is still to be determined.
Adrenomedullin
This circulating peptide is a potent vasodilator, with its effects mediated by cAMP and NO-dependent mechanisms (Nakamura et al., 1997). Initial human studies of both intravenous and inhaled formulations have shown evidence of efficacy in small samples, though further studies are needed to confirm this effect (Nagaya et al., 2000; 2004).
Combination Therapy
The above agents represent currently available and future therapeutic modalities, yet the best treatment approach remains unclear. It is clear that WHO functional class II patients may benefit from therapy, with a greater benefit seen in WHO functional class III. While the overall number of patients is low, patients with the most severe functional impairments fare far worse in these trials. Orally bioavailable formulations are usually employed as first-line agents because of the ease of use, either ERAs or PDE5 inhibitors. This represents a practical approach, particularly in patients with mild impairment, yet the treatment of more severe disease at presentation remains more controversial. Combination therapy with differing classes of medications, targeting multiple separate biologic pathways, becomes important as severity increases; yet at this time, with only three separate classes available, the treatment of the most severe patients usually results in utilization of all three classes. Surgical intervention or implementation of experimental agents becomes necessary if response is not optimal. Controversy arises in the patients with moderate to severe functional limitations. Single agents produce modest effects, while combination therapy may provide a synergistic effect leading to more dramatic improvement in both symptoms and hemodynamic measurements. Treatment algorithms have been proposed (Fig. 4) (McLaughlin et al., 2009; Desai and Machado, 2011), yet studies to validate these algorithms have not been undertaken. A recent abstract was presented in which a combination of epoprostenol, bosentan, and sildenafil in severe PAH patients resulted in a substantial improvement in functional and hemodynamic measurements; further studies are needed to confirm these results that may help validate the use of combination therapy (Sitbon et al., 2011).

PAH treatment algorithm. Proposed treatment algorithm from Desai et al, (2011). Pulmonary Circulation. ERA, endothelin receptor antagonist; FC, functional class; IV, intravenous; PDE-I, phosphodiesterase inhibitor; PO, oral.
Surgical treatment
Surgical management is infrequently required in all but the most severe PAH patients that do not respond to medical management (McLaughlin et al., 2009). Lung transplant remains the preferred surgical procedure, though significant morbidity and mortality exist, particularly in patients with poor preoperative status (Keogh et al., 2009). As of October 2010, the United Network of Organ Sharing showed IPAH lung transplant survival of 83%, 47.5%, and 34.7% at 1, 5, and 10 years, respectively (United Network, 2012). There is still much debate whether bilateral lung transplant versus heart–lung transplant is preferred, yet recent data suggest that outcomes are similar, although preferential heart–lung transplant is often indicated in right-heart failure (Fadel et al.). For patients in whom lung transplant is not a viable option or donor organs are unavailable, atrial septostomy may provide symptomatic improvement. Puncture of the atrial septum creates a physiological shunt through the atrial septal defect. Atrial septostomy has been shown to improve cardiac output without significant change in mean PAP and at the expense of worsening hypoxemia due to the right-to-left shunt (Law et al., 2007). The procedure was also associated with 23% mortality, which correlated with higher presurgical right atrial pressures. Surgical management, though associated with high levels of morbidity and mortality, remains essential with insufficient medical therapies available for the most severe patients.
Conclusion
The future of PAH therapy appears promising through development of new classes of medications while improving the pharmacokinetic properties of available agents. New agents are attempting to exploit distinct pathways that may lead to more robust changes in the disease course and prognosis. These newer agents represent the future of PAH treatment and we remain hopeful that this debilitating, deadly disorder will soon have a more robust therapeutic arsenal in order to move toward a cure. In addition, new work focusing on the treatment of high-altitude pulmonary hypertension may be able to expand the therapeutic role of both new and established PAH treatment modalities.
Footnotes
Author Disclosure Statement
No competing financial interests exist.