
Abstract
Abstract
Richards, Paul, and David Hillebrandt. Clinicians Corner: The practical aspects of insulin at high altitude. High Alt Med Biol 14:197–204, 2013.—With the increasing prevalence of diabetes and current social philosophy of enablement, many more diabetics are travelling to high altitude where the rate of AMS in Type 1 diabetic mountaineers is no different than nondiabetics. Numerous effects of exercise, both degree and duration, dietary change, illness, stress, mountain sickness, counter-regulatory hormones, and altitude increased sympathetic output, and catecholamines have led to conflicting accounts of insulin requirement increasing or decreasing at altitude. Overall, it would appear that the effects of diet and exercise outweigh those of altitude. Good control requires continual insulin dose adjustment with frequent feedback from blood sugar testing, but glucometers can over- or under-read at altitude. Additionally, heat or cold exposure can degrade insulin efficacy; strategies for storing insulin are described.
Introduction
This article focuses on the management of insulin in Type 1 diabetics in the high altitude environment. Unfortunately, as is often the case in altitude medicine, there is a paucity of studies to guide clinical practice, and indeed much of the physiological research of the effects of exercise or hypoxia on glycemic and metabolic control have been conducted on nondiabetics. The information within derives from the published literature where it exists, and where it doesn't exist, the opinion and hypotheses of the authors are given, these being derived from their practical experience as mountaineering diabetics and advisors to a commercial mountaineering guiding company, and from the practical experience of the wider mountaineering diabetic public (Mountains for Active Diabetics, 2013).
Crossing Time Zones
Reaching the World's Greater Mountain Ranges often involves long distance travel across time zones. When this occurs rapidly, for example by air, adjustment of insulin dose is usually required. When travelling East to West, the day is effectively prolonged and an extra meal is often included, requiring extra insulin (usually fast acting). Conversely, when traveling West to East, the day is effectively shortened and the insulin dose should be reduced. Up to 2–4 hours time difference can often be tolerated by many diabetics (American Diabetes Association, 2013; Chandran and Edelman, 2003; Diabetes UK, 2013) as part of the day-to-day 10%–20% intra-individual variability in insulin metabolic effect (Heinemann et al., 1998). Some diabetics prefer to continue on home-time, making adjustments to the time of taking food and insulin by 2–3 hours per day until destination time is matched. For this, a second watch with reminder alarm is useful.
Factors Affecting Insulin Requirement
Insulin promotes glucose transport into muscles, liver, and adipose tissue. The liver is the main organ of glucose homeostasis, producing glucose [from glycogenolysis of liver glycogen, gluconeogenesis from lactic acid, fatty acids (via glycerol) or some amino acids] in response to a lowering of blood glucose, raised glucagon, catecholamines, and growth hormone, and taking up glucose from the blood in response to insulin to form liver glycogen, or if this is replete, fatty acids. Blood glucose level is therefore a result of the interplay of the above hormones. Travel, stress, anxiety, circadian dysrhythmia, infection, unfamiliar food, hypobaric hypoxic gastrointestinal disturbance, and AMS may all affect appetite or glycemic control.
Exercise facilitates non-insulin-dependent glucose transport into skeletal muscle (via uprating of membrane GLUT-4 transporters) and reduces a diabetic's insulin requirement for several hours (MacDonald, 1987). Guidelines suggest that basal insulin may need reducing 10%–20% the night after exercise to prevent subsequent hypoglycaemia, whilst insulin doses may need to be increased on rest days (Perry and Gallen, 2009). Upper limb exercise (Ahlborg et al., 1986) or short bursts of intense exercise (Gallen, 2005) can produce hyperglycemia due to enhanced counter-regulatory hormone response. The added effect of altitude however complicates, as it appears that insulin requirement may increase with altitude (de Mol et al., 2011; Pavan et al., 2003), in one case producing unexpected hyperglycemia in spite of markedly increased exercise with unchanged food intake or insulin (Valletta et al., 2011). The effect has been attributed to increased sympathetic activity, counter-regulatory hormones, cortisol, growth hormone, and catecholamines (Leal. 2005). Post expedition HBA1c increases in both diabetics (in spite of increasing insulin) and nondiabetics, suggesting altitude has a detrimental effect on glycemic control (Pavan et al., 2004). It is possible that these changes reflect a similarity of catecholamines associated with an equal prevalence of AMS in both groups. Hyperglycemia with exercise may also represent over-reduction in baseline insulin or an issue with dose timing. Reducing insulin by 50% in compensation for lower oral carbohydrate due to anorexia may have contributed to hyperglycemia and ketosis in four climbers on the Diabetes Federation of Ireland Kilimanjaro Expedition (Moore et al,. 2001b). Admetlla et al. (2003) found on Aconcagua that overall, diet and exercise had a greater influence on glycemia than altitude.
Delayed gastrointestinal carbohydrate absorption at altitude>5000 m has led to postprandial hypoglycaemia, but later hyperglycemia in which case bolus insulin would be better taken with or even just after a meal rather than the usual pre-prandial dosing (Admetlla et al., 2001). Additionally, the tendency to favor a carbohydrate diet at altitude may require insulin dosage adjustment.
Dexamethasone raises insulin resistance even in nondiabetics (Zarkovic et al., 2008) so should be avoided for prophylaxis. The seriousness of HACE justifies emergency use but will require frequent (hourly) blood glucose monitoring. Both increases and decreases in blood glucose have been reported with acetazolamide in rodents (Boquist et al., 1980a; 1980b; Pharmacy Retailing (NZ) Limited,2010; Sener et al., 2007), so if its use is contemplated for AMS prophylaxis then trial before departure with appropriate insulin dose adjustment is advised. During the Diabetes Federation of Ireland Kilimanjaro Expedition 1999, the two sickest diabetics had been taking acetazolamide and one remained acidotic, even after achieving euglycemia and resolution of ketonuria (Moore et al., 2001b). Overzealous insulin dose reduction above, continued exertion whilst ketonuric and dehydration were likely contributory as a later study, again on Kilimanjaro with a similar ascent profile where 8 of 11 Type 1 diabetics took acetazolamide, did not have these problems (Kalson et al., 2007). Nevertheless, with the potential to worsen acidosis, some caution in the use of acetazolamide is advised.
Overall, it would appear that insulin requirement is an integration of hypoglycemic factors (exercise, reduced dietary intake) and hyperglycemic factors (short intense exercise, stress, or AMS giving raised counter-regulatory hormones, dawn phenomenon). Hence, an individual's dosing of long and rapid insulin requires a great deal of ‘trial and error’ and acquisition of experience, and it is important that diabetics are well practised in their own particular dose adjusting requirements in environments and with the degree and duration of exercise, similar to those anticipated on the mountain (Panofsky, 2002).
Insulin
It follows that flexibility in insulin dosing is essential for optimising control during exercise or altitude travel. Nondiabetics secrete a low level baseline insulin with bolus release to process carbohydrate meals (Galloway and Chance, 1994) (Fig. 1).
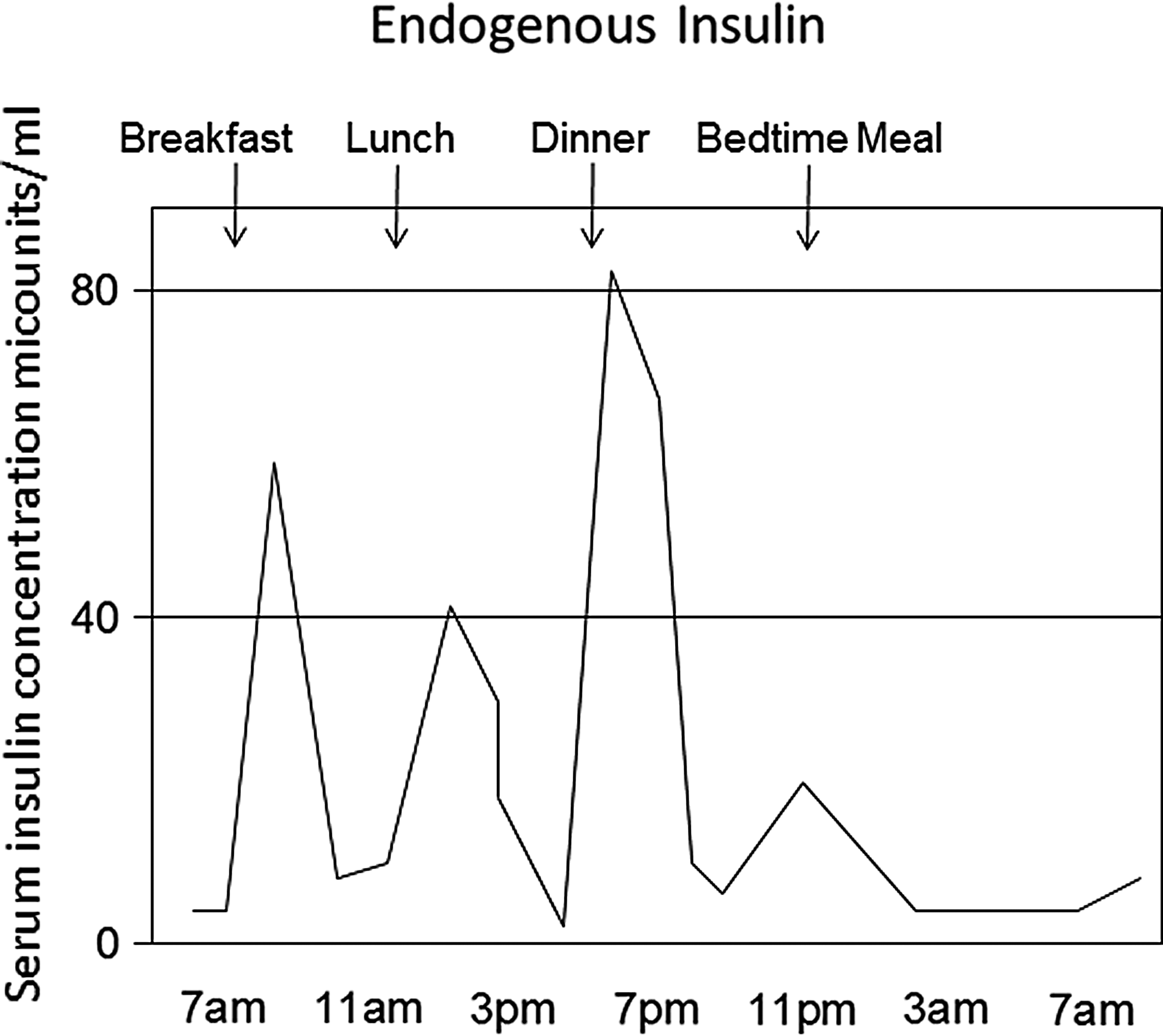
Timing of insulin release in nondiabetics. Adapted from Galloway and Chance (1994).
Fixed mixtures of short acting (peak 1–2 hours, duration 6–8 h) and intermediate ( peak in 4–6 h, duration 8–12 h) insulins typically in a 30:70 or 50:50 ratio may limit the possibility of frequent adjustment and require a more regular routine (Fig. 2a). The most flexible dosing aims to mimic normal physiological response, hence the popularity of Basal-Bolus regimes (Gallen, 2005). This can be achieved by separate injections of intermediate acting baseline twice a day, with short acting boluses for meals (Fig. 2b). Newer insulin analogues such as Insulin Detemir or Insulin Glargine give a long-acting (16–24 h) smooth almost peakless profile and can be given once a day, though some find better control at twice daily (Fig. 2c) (MIMS, January 2013). New rapid-acting insulin analogues such as Insulin Aspart, Lispro, or Glulisine have onset in 10–20 min (peak in 1 h, duration of 3–5 h) enabling dosing actually with, or just after, eating, thus removing the necessity to dose and plan eating 20–30 min ahead, which is often not possible in the mountains. The dose of mealtime rapid-acting insulin is calculated depending on the carbohydrate load, the degree, type and duration of activity, and with consideration of any remaining activity from previous insulin doses.
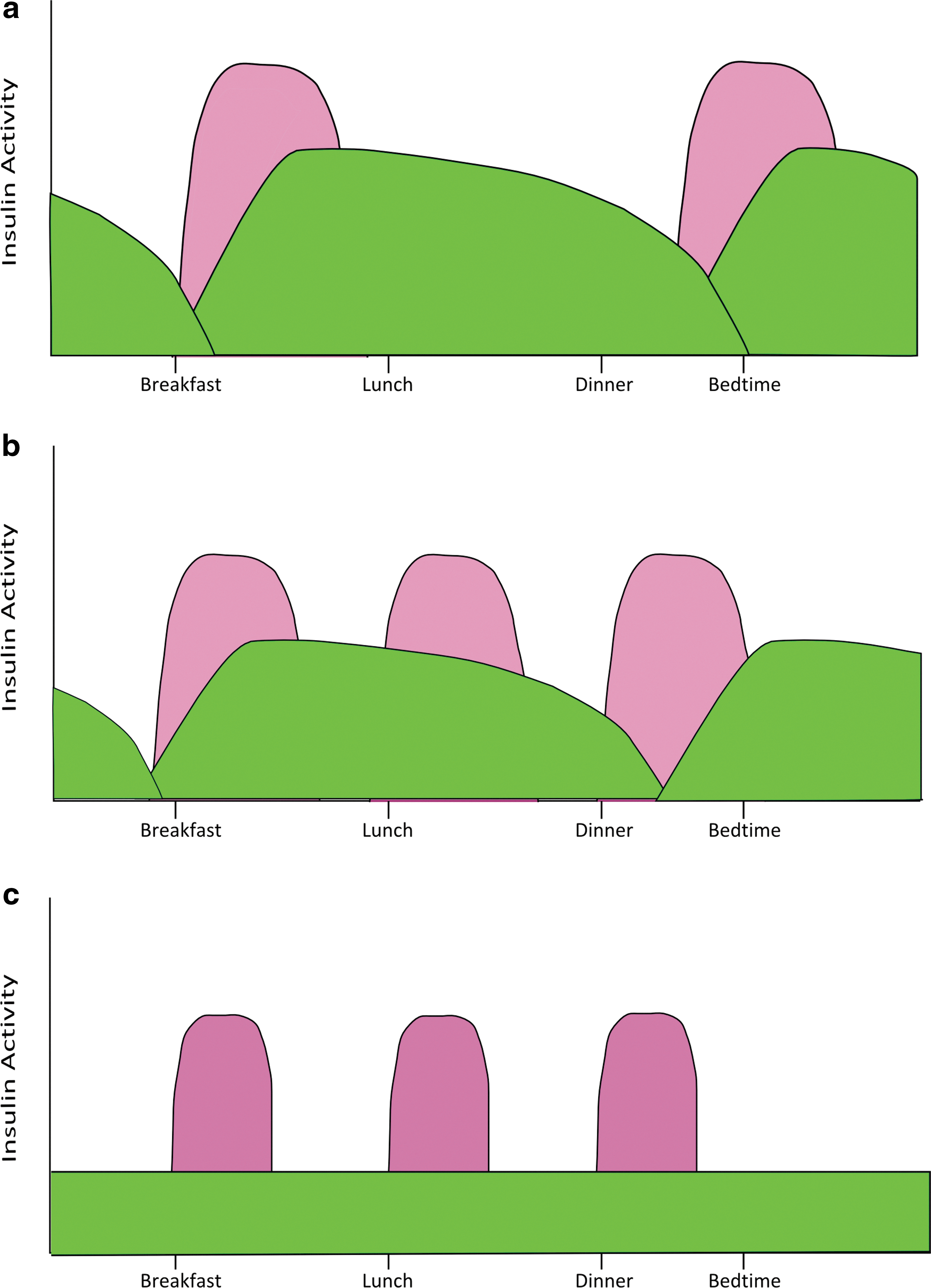
Twice daily fixed short/intermediate insulin mix. (Rigid Routine) Illustrative, after MIMS January (2013),
Traditional insulin delivery systems of a bottle with separate needle and syringe have been superseded by convenient pen devices, either as wholly disposable units or with replaceable disposable insulin cartridges (Fig. 3). Unlike traditional syringes, the dose is determined simply by rotating a dial, and pens can be obtained calibrated in half units for children or those on low doses. Some pens have accessories to ease use with arthritic hands, which are useful when wearing gloves. Pens may not be available in some countries, so traveling with adequate supplies is essential. Additionally U40 or U80 (cf U100 used in USA and Europe) concentration insulins are still available in some countries, needing care if purchasing emergency supplies locally.

Insulin pens.
Diabetics usually rotate injection sites to prevent lipohypertrophy. Absorption is fastest from the abdomen, arm, then thigh, though thigh absorption is increased during leg exercise due to enhanced subcutaneous blood flow (Koivisto and Felig, 1978).
Insulin pumps are gaining in popularity, giving a continuous low dose infusion of subcutaneous rapidly-acting insulin. These pumps afford the most precise microadjustment of dosing but require training and familiarity. They have the advantage of being set up in the warmth of a tent, and injection sites do not require recurrent exposure during the day, though there is possibly an increased risk of local injection site infection. Pressure change even at aircraft cabin altitude (2000 m equivalent) can cause bubble formation as dissolved air comes out of solution and existing bubbles expand, both leading to displacement of insulin and increased dosing on ascent (possibly leading to hypoglycemia 1–2 h later) with converse on descent (King et al., 2011). Anecdotally, the effect seems to be minimal compared with the multitudinous other factors acting above, but it would seem wise to be aware of the phenomenon and to remove any bubbles from the system before ascent and every 1000 m (Panofsky, 2002). Similarly, care is required not to inject air bubbles rather than insulin when using pens.
Manufacturers specify insulin must not freeze, be protected from light, and stored between 2–8°C, but advise viability at room temperatures (<25°C) for up to a month, after which they recommend it should be discarded (January 2013; 2013a; 2013b; 2013c). Beyond 1 month, or at higher temperatures, degradation does not become harmful but efficacy is not guaranteed and indeed higher temperatures such as 32–37°C for 28 days resulted in loss of potency of 14%–18% in one study (Vimalavathini and Gitanjali, 2009). Viability of diluted Insulin Lispro at 30°C was however unchanged at day 32 (Stickelmeyer et al, 2000). Physical agitation of the molecule may possibly contribute to degradation. Doses may need increasing over time to compensate for reduced efficacy.
Needles should be removed from pens/vials after injection as air pressure or temperature changes can cause expulsion of fluid, potentially affecting homogeneity of the insulin.
Glucometers
It is important that the diabetic checks the end-effect (ie, blood glucose on a regular basis) before basal and meal dosing, and in between when exercising. This may result in testing 10 times a day, or more when exerting (Gallen, 2005). Several factors influence blood glucometer readings, including temperature, hematocrit, hypoxia, and site of sampling (Ginsberg, 2009). Modern meters operate typically between 10°C and 40°C and will alert or refuse to work outside these ranges. Low blood oxygen tension theoretically would cause glucose oxidase-based meters to over-read, which was reported to be as much as 6%–15% in one study where glucose dehydrogenase-based strips were more accurate at altitude (Oberg and Ostenson, 2005), whereas other studies have shown the converse at moderate altitude (Olateju et al., 2012). Several studies confirm over- or under-reading at altitude of both reagents (Bilen et al., 2007; Fink et al., 2002; Gautier et al., 1996; Giordano et al., 1989; Olateju et al., 2012; Pavan et al., 2004; Pecchio et al., 2000) and discrepancy between simulated and real altitude (de Mol et al., 2010). Technological improvement may reduce these errors (Bailey et al., 2012; Lock et al., 2011) and in any case the clinical effect would appear minimal unless over-reading on the borders of hypoglycemia.
Blood sampling site is also important when low temperature reduces skin blood flow. This is more important at sites such as the forearm with prolonging of the usual 15–30 min lag time (Haupt et al., 2005). Fingertips are least affected due to arteriovenous shunting.
Continuous Glucose Monitors (CGM) are useful for showing trends, but as they measure from interstitial fluid, not capillary blood, they have a prolonged lag time and should not be relied upon for dosing, rather prompting normal capillary blood testing.
Most meters are now amperometric, measuring current as electrons are released by chemical interaction with glucose, and there are few photometric meters now available (eg., Accucheck Active) where glucose measurement is indicated by change of reagent strip color. The latter is useful for manual reading backup in case of meter failure, but is not reliable in the orange tinge or other colored light inside a tent! Test strips can be damaged by high temperatures or humidity and must be stored with desiccant in sealed containers.
Hypoglycemia
The major concern of many diabetics is hypoglycaemia, particularly in safety critical situations and many diabetics choose to run their sugars slightly high (7–9 mmol/L) when away to minimize the risk. Hypoglycemia symptoms show inter-individual variability, but are usually consistent within an individual and may manifest as fatigue, hunger, agitation, trembling, difficulty with fine motor tasks (buttons, ropes), sweating, palpitations, aggression, or behavioral change or, if particularly severe, reduced Glasgow Coma Scale (GCS), coma, or seizures. Blood glucose<4 mmol/L requires prompt treatment with fast acting carbohydrate to which the diabetic should always have ready access, for example, snack bars or glucose sweets/drinks. Glucose gels (Glucogel®) can be applied to the buccal membrane by companions or glucagon 1 mg SC/IV/IM injected. Absorption of the latter will be impaired by cool muscles and will be ineffective if the hypoglycemic episode has been caused by depletion of glycogen stores, which is quite possible at the end of a long mountain day. Hypoglycemia can lead to hypothermia, and both can be confused with AMS (Moore et al., 2001a). Any unwell diabetic should have prompt and repeated blood glucose measurements. A treated significant ‘hypo’ leaves the diabetic feeling fatigued with clouded judgement for up to 2 hours.
Hypoglycemic awareness, where the diabetic is able to recognize symptoms associated with hypoglycemia in sufficient time to take remedial action, can be impaired with frequent hypoglycaemia, resulting in a six-times increase in the risk of severe (ie., requiring the assistance of a another person) hypoglycemia (Geddes et al., 2008). Awareness can be regained after 3 to 4 weeks of good diabetic control absent of hypoglycaemic episodes (Bakatselos, 2011; Cranston et al., 1994; Dagogo-Jack et al., 1994).
Hyperglycemia and Ketoacidosis
General advice in the wilderness to monitor hydration by observing urine color is complicated in diabetics by an osmotic diuresis once blood glucose exceeds 10 mmol/L. Thus, the relatively clear urine may give false reassurance, when in fact the hyperglycemic diabetic is dehydrating. In a wilderness setting, ketoacidosis carries a high risk of mortality (Basnyat,1995; Shlim and Gallie, 1992). It would appear that it is a relative lack of insulin (reduced or no dosing, reduced efficacy from environmental/heat damage, misdosing due to meter error) in conjunction with other factors such as dehydration, infection, AMS, or continuing to exercise with ketonuria that particularly raises risk (Leal, 2005; Moore et al., 2001b).
Practicalities
For customs, carriage of medication in original packaging is advised along with a letter from the prescribing physician. Airport security X-ray machines are not considered harmful to insulin itself, but these or airport body scanners might damage insulin pumps or continuous glucose monitors, which should be removed and checked manually (Cornish and Chase, 2012). Security now commonly requires separate manual presentation of liquids to staff for examination. Twice the estimated maximum required amount of insulin, needles, test strips, lancets, and other consumables for the trip, along with spare glucometers and batteries would be recommended, carried in hand luggage to prevent freezing in baggage holds and, at destination, split between team members in case of individual bag loss. Pump users should carry spares, and for all, a low-tech option such as traditional insulin needles and syringes in case of failure of the primary system and the need to obtain local insulin supplies. The availability of the latter and location of local health clinics is best determined pre-departure; The International Society of Travel Medicine provides a register for worldwide clinics that can give a starting point for researching local facilities. If possible, some insulin should be stored in a reliable refrigerator at the arrival city so that at the end of the expedition the diabetic can return to fully efficacious insulin.
In cold environments, many diabetics utilize body warmth to prevent insulin, meters, and batteries freezing by storing in pouches, sometimes commercially available like old transceiver bags or otherwise homemade from fleece or other insulating material, worn outside their base layer thermal underclothes, similarly taking kit inside sleeping bags at night (Fig. 4). Such holders and use of tape and tethering cord also reduce risk of dropping the kit when on climbs. Others carry their insulin wrapped in bubble wrap inside food/drink type vacuum flasks or create homemade closed-cell foam pouches heated by disposable chemical heat pads. In hot conditions, water evaporative cooling from proprietary pouches such as Frio® or Poucho® palpably reduce insulin temperature by a few degrees (Fig. 5).

Homemade protective warming pouch (Dianna Maynard).
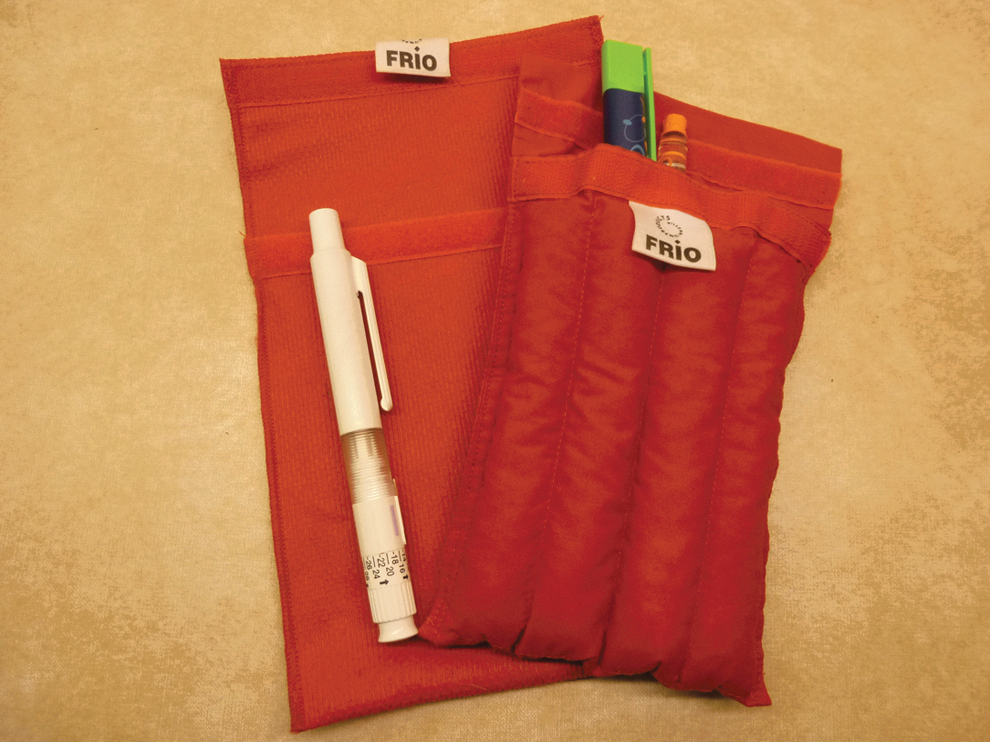
Frio® evaporative cooling pouch.
Blood sugar testing can be difficult in a storm, and wet or windy conditions tend to be more problematic than snow. Some diabetics will cut the tips off inner gloves to give a testing flap. Thigh ventilation zips enable access for injections, and some manufacturers will adapt clothing with extra zips/Velcro® to assist access at other sites. In really bad weather conditions, a bothy bag provides warmth and wind protection. Equipment such as climbing harnesses may prevent access to usual injections sites and alternatives should be practiced pre-departure. Direct injection through clothing, although practised by some, risks introducing infection or fiber fragments into the skin, pre-degrades sharpness of needles before skin contact, and is likely to require longer needles to ensure adequate penetration.
Small sharps boxes (eg., 0.3 L– 0.5 L) are available for safe carriage of used needles, lancets, and test strips during the trip. Safe disposal may follow local guidelines where they exist but in some developing economies it may be more appropriate to repatriate and dispose at home at least of the sharps. In this case, a needle cutter (eg., BD Safe-Clip®) drastically reduces sharp waste volume.
It is vital to inform companions of the diabetes, not least as any illness is likely to impact their trip, maybe even placing them into danger. It is also sensible to educate them in hypoglycemia recognition and treatment. Ideally diabetics should be accompanied by someone who knows them well and who can detect subtle signs of hypoglycemia prompting glucose testing. It is wise for all to share accommodation at high altitude so that severe illness might be detected, but particularly so for diabetics. Insurance that includes medical cover, search, and rescue and repatriation by air ambulance is advised and best sought in good time as it may require a specialist provider.
Conclusion
• Ensure travel with adequate testing and insulin supplies with 100% spares in case of loss or delays. Carry in hand luggage, as aircraft holds may have a freezing risk.
• East to West Travel: Day prolonged. Additional carbohydrate meal and insulin bolus.
• West to East Travel: Day shortened. Reduce total insulin dose.
• Hyperglycemic factors: Under dosing insulin; stress, intercurrent illness, short intense bursts of exercise, AMS.
• Hypoglycemic factors: Insulin, sustained steady exercise, reduced food intake.
• Possible delayed GI carbohydrate absorption at altitude predisposes to postprandial hypoglycaemia: take insulin with or just after meals.
• Overall, diet and exercise probably have a greater influence on glycemia than altitude.
• Hypoglycemia in a wilderness environment can be particularly dangerous, so many diabetics choose to maintain their sugars slightly raised but controlled. Companions should be aware of presenting signs and symptoms and remedial action (oral glucose/IM glucagon).
• Insulin Basal-Bolus regimes afford greatest flexibility in matching insulin to diet and activity.
• It is essential for the diabetic to be familiar with managing diabetes and insulin dose adjustment in the environment and with the degree and duration of exercise anticipated at altitude. Trial runs at lower altitude can assist in gaining experience.
• Insulin must not freeze but will remain viable at ‘room temperature’ for a month with loss of efficacy in higher temperatures or after this date. Storage in insulated containers or use of proprietary evaporative cooling bags assist in maintaining a temperature nearer optimal.
• Glucometers may under- or over-read at high altitude but the clinical significance is probably minimal.
• With frequent capillary blood sugar testing and a basal-bolus regime, many conflicting theoretical considerations can be minimized, as it is all dealt with on a practical level.
Further Information
Mountains for Active Diabetics. http://www.facebook.com/groups/131297830871/An international group of mostly lay diabetic mountaineers and active outdoor enthusiasts with a wealth of practical experience in managing diabetes in extreme conditions.
Think Like a Pancreas 2nd Ed. Gary Scheiner. Pub: Da Capo Lifelong Books; Nov 2011; ISBN-10: 0738215147; ISBN-13: 978-0738215143
Diabetic Athlete's Handbook. Sheri R. Colberg. Pub: Human Kinetics Europe Ltd; 1 edition Jan 2009; ISBN-10: 0736074937; ISBN-13: 978-0736074933
Type 1 Diabetes: Clinical Management of the Athlete. Gallen I. Pub Springer March 2012; ISBN-10: 0857297538; ISBN-13: 978-0857297532
Declaration of Interest
Both PR and DH are active insulin-dependent diabetic mountaineers and advisers to a commercial high altitude trekking and mountaineering company.
Appendix: Case Vignette
A previously fit and experienced 42-year-old mountaineer was diagnosed as suffering from late onset Type 1 diabetes 5 months before departing on an expedition attempting to climb Mount Everest. He had a good theoretical knowledge of his problem but little time to gain practical experience of insulin use in high mountain terrain due to the normal pressures leading up to an expedition departure. At base camp, the night before a pre-dawn departure through the Khumbu icefall, he had an unexplained hypoglycemic episode (capillary glucometer reading at 5400 m of 3.2 mmmol/L) that required self-administered rescue carbohydrate with resultant rebound hyperglycemia and the apparent need for additional insulin prior to departure.
The conditions were clear but very cold as he faced sustained exercise in hypoxia, interspersed with short bursts of increased exertion on the fixed ladders. Hypoglycemic awareness was intact, but appreciation of symptoms may have been blunted by the environment, the previous night's hypoglycemic event, and some degree of anxiety. His usual hypoglycemic symptoms of agitation, hunger, fatigue, and reduced dexterity were initially abolished by consumption of emergency carbohydrate in various jacket pockets but, later in the climb, when these symptoms worsened, all easily accessible stocks had been exhausted. He had to stop in a particularly dangerous part of the icefall, exposed to daunting seracs, to enable him to retrieve additional reserves from deep within his rucksack. On improvement some minutes later, he was able to climb the nearby ladder to join his companions who had sensibly decided to continue to a place of relative safety. After a recovery period, they were then able to continue the ascent to Camp 1 without further incident.