
Abstract
Abstract
Weinbruch, Stephan, Karl-Christian Nordby. Fatalities in high altitude mountaineering: A review of quantitative risk estimates. High Alt Med Biol 14:346–359, 2013.—Quantitative estimates for mortality in high altitude mountaineering are reviewed. Special emphasis is placed on the heterogeneity of the risk estimates and on confounding. Crude estimates for mortality are on the order of 1/1000 to 40/1000 persons above base camp, for both expedition members and high altitude porters. High altitude porters have mostly a lower risk than expedition members (risk ratio for all Nepalese peaks requiring an expedition permit: 0.73; 95 % confidence interval 0.59–0.89). The summit bid is generally the most dangerous part of an expedition for members, whereas most high altitude porters die during route preparation. On 8000 m peaks, the mortality during descent from summit varies between 4/1000 and 134/1000 summiteers (members plus porters). The risk estimates are confounded by human and environmental factors. Information on confounding by gender and age is contradictory and requires further work. There are indications for safety segregation of men and women, with women being more risk averse than men. Citizenship appears to be a significant confounder. Prior high altitude mountaineering experience in Nepal has no protective effect. Commercial expeditions in the Nepalese Himalayas have a lower mortality than traditional expeditions, though after controlling for confounding, the difference is not statistically significant. The overall mortality is increasing with increasing peak altitude for expedition members but not for high altitude porters. In the Nepalese Himalayas and in Alaska, a significant decrease of mortality with calendar year was observed. A few suggestions for further work are made at the end of the article.
Introduction
O
High altitude mountaineering (defined in this article as attempting a mountain with an altitude above 5000 m) is inherently associated with high risks due to the harsh environmental conditions, including low oxygen partial pressure, low temperatures, strong winds, as well as steep and difficult terrain. Thus, these ventures often led to fatal accidents since their beginnings in the nineteenth century. A well known example is the death of Albert Frederick Mummery and his two Gurkha porters Ragobir and Goman Singh in August 1895 at Nanga Parpat, during the first serious attempt on an 8000 m peak (e.g., Sale and Cleare, 2000).
The first quantitative risk estimates for high altitude mountaineering were published in the late seventies/early eighties of the last century (Wilson et al., 1978; Weingart, 1980; Ridden, 1983). In the meantime, the number of publications on quantitative risk estimates for high altitude mountaineering has increased significantly (Pollard and Clarke, 1988; Lattimore, 1993; Christensen and Lacsina, 1999; Huey and Eguskitza, 2000, 2001; Huey and Salisbury, 2003; McIntosh et al., 2008; Firth et al., 2008; Salisbury and Hawley, 2011; Westhoff et al., 2012), but data are mainly restricted to the Nepalese Himalayas and Denali in Alaska. In addition to reporting incidence proportions for mortality, the most recent publication (Westhoff et al., 2012) also applies advanced statistical techniques (multivariate analysis, Kaplan-Meier analysis) for hypothesis testing.
In the present article, we review the literature on quantitative risk estimates for high altitude mountaineering. The endpoint investigated is death as reliable data are only available for this outcome. The recent reviews related to mountaineering risks either focus on educational aspects (Windsor et al., 2009), discuss causes of accidents (Knott, 2011), are ristricted to injuries (Mort and Godden, 2011), or are limited to rock and ice climbing at lower altitudes (Schöffl et al., 2010). In contrast, a detailed review of the risk estimates for high altitude mountaineering, including the heterogeneity of risk estimates, as well as confounding, is presented here. The risk estimates are discussed separately for members of expeditions and for hired personnel (i.e., high altitude porters). A few suggestions for further work are given at the end of the article.
Statistical analyses
Statistical parameters (mean values, confidence limits, p values) are in most cases taken directly from the original publications. Logistic regression to analyse the association between mortality and altitude was performed with SPSS version 20. The risk ratio and its confidence limits are calculated according to Rothman (2002).
Quantitative Risk Estimates for Expedition Members
Overall risk estimates
Quantitative risk estimates published in the scientific literature for expedition members are summarized in Table 1. In addition to high altitude mountaineering, risk estimates for mountaineering at lower elevations (e.g., Rocky Mountains, Cascade Range, New Zealand) are also given. All incidence proportions listed in Table 1 are based on detailed exposure data. The characteristics of the reviewed studies are summarized in Table 2; publications discussing mortality of high altitude mountaineering without performing epidemiological analysis of original data are not included. The incidence proportions given in Table 1 are generally of high accuracy, as the number of fatalities as well as the number of exposed climbers (denominator) are known precisely. Some of the estimates for mountaineering at lower elevation (Ferris, 1963; Christensen and Lacsina, 1999; Malcolm, 2001) lack accurate exposure data and have, thus, higher uncertainties. Quantitative risk estimates based on general participation in sports are available for mountaineering in England and Wales (Avery et al., 1990) as well as Austria (Burtscher, 1990, 1996; Burtscher and Nachbauer, 1999; Burtscher et al., 1993, 1994, 1995, 1997a, b). These risk estimates are not included in Table 1, as they are not based on detailed records of the number of exposed. However, they will be discussed when comparing the risks of high altitude mountaineering with other disciplines of mountain sports.
Only members of expedition (hired personnel excluded); *listed are only peaks with >500 members above base camp;
references: (1) Wilson et al., 1978; (2) Lattimore, 1993; (3) McIntosh et al., 2008; (4) Huey and Eguskitza, 2001 (5) Schussman et. al., 1990; (6) Christensen and Lacsina, 1999; (7) Ridden, 1983; (8) Malcolm, 2001; (9) Salisbury and Hawley, 2011; (10) Firth et al., 2008; (11) Huey and Salisbury, 2003; (12) Shlim and Houston, 1989; (13) Shlim and Gallie, 1992; (14) Weingart, 1980; (15) Pollard and Clarke, 1988; (16) Ferris, 1963.
For high altitude mountaineering in Alaska, the Himalayas, Karakoram, Hindu Kush, and Peru, the overall mortality (incidence proportion) varies about one order of magnitude between 3/1000 and 43/1000. As already mentioned by Weinbruch and Nordby (2010), the fatality risk of mountaineering at lower altitudes (below 5000 m) and of trekking in Nepal is more than one order of magnitude lower (0.14/1000 to 0.6/1000). In Alaska and the Nepalese Himalayas a decrease of the fatality risk with time (calendar year) is observed.
Inhomogeneity of risk estimates
The incidence proportions summarized in Table 1 must be regarded as crude estimates, as the fatality risk of high altitude mountaineering is not distributed homogeneously on a given mountain and during the course of an expedition.
Distribution of fatalities on a given route
For the Nepalese Himalayas, it is reported that for expedition members (as opposed to high altitude porters) the summit bid is the most dangerous part of an expedition. During the spring seasons from 1982 to 2006 on Mount Everest, for example, about 82% of the member fatalities on the standard routes occurred during the day of the summit attempt or one day later, compared to a typical duration of an Everest expedition of 60 days (Firth et al., 2008). About 85% of deaths on the North route (i.e., from Tibet) and about 44% on the South route (i.e., from Nepal) occurred above 8000 m. A similar result was reported by Westhoff et al. (2012) for members of commercial expeditions in Nepal who most likely died on their summit bid, in contrast to traditional (i.e., noncommercial) expeditions where members most likely died during route preparation (see also “expedition type” below). The especially high risk during the summit bid can be also seen from the distribution of fatal fall accidents on 8000ers with most incidents occurring above 7500 m (Salisbury and Hawley, 2011).
Looking at individual 8000 m peaks (years 1990–2009) reveals a more complex pattern (Salisbury and Hawley, 2011): the standard routes on Kangchenjunga, Everest (North route only), Makalu, Lhotse, Cho Oyu, and Dhaulagiri I have a higher fatality risk (incidence proportion) for members above the highest camp compared to at or below highest camp. In contrast, standard routes on Manaslu and Annapurna I have a higher mortality risk for members at or below the highest camp, most likely due to an increased probability of avalanches (Salisbury and Hawley, 2011).
A higher risk towards the summit is also observed on Denali (Alaska, USA) where, according to Lattimore (1993), half of the emergencies (not fatal accidents) occurred above 5000 m, where most climbers spend less than 20% of their expedition time of typically 3 weeks.
Distribution of fatalities among different routes on the same mountain
For the Nepalese Himalayas, the results of different publications are somewhat contradictory. According to Huey and Salisbury (2003), the fatality risk is similar for members of the different standard routes at Everest (1980 to 2002, spring season): 18/1000 for the north ridge and 14/1000 for the southeast ridge. For the other routes, a slightly (but not significantly) higher incidence proportion was observed (24/1000). The mortality of members descending from the summit was also similar on all routes (45/1000 north ridge, 26/1000 southeast ridge, 34/1000 other routes). Similar death rates on the different commercial routes on Everest (members, spring season, 1990 to 2005) were also reported by Huey et al. (2007).
These results are corroborated by Westhoff et al. (2012) who observed by multivariate analysis that the use of the standard route was not associated (p=0.14) with the odds of death on 8000ers in Nepal (members, January 1970 to spring season 2010).
In contrast, a significantly higher mortality on non-standard routes was observed for Dhaulagiri I and Everest by Salisbury and Hawley (2011). On Denali in Alaska, a similar observation was made by Latimore (1993) with the fatality risk significantly (p<0.001) increasing with increasing degree of technical difficulty (2.0/1000 for Alaska grade 2; 8.8/1000 for grades 3 and 4; 25.8/1000 for grades 5 and 6). At the same mountain, the likelihood of search and rescue operations was also significantly higher on other routes than the standard West Buttress route (McIntosh et al., 2010).
Death during descent after summiting
Mortality during descent after summiting is reported in a number of publications (Table 3), but is restricted with the exception of Denali (Alaska) and Mount Rainier (Cascade Range, USA) to peaks with altitudes above 8000 m. There are pronounced differences between the individual 8000ers most likely reflecting the variable technical difficulties and objective dangers (e.g., avalanches).
members and hired personnel; *without using supplementary oxygen; +for Everest and K2 only without using supplementary oxygen, for the rest with and without use of supplementary oxygen.
For Everest, the mortality during descent after summiting can be compared to that above base camp, because both parameters are known separately for members and hired personnel as well as for different routes. The mortality of expedition members during descent from the summit of Everest on standard routes is on the order of 27/1000 (Firth et al., 2008), and is significantly higher than the mortality above base camp which is on the order of 16/1000 (Huey and Salisbury, 2003). Although not exactly the same time period is compared, the higher risk during descent from the summit is obvious. A high risk during descent after summiting was also found by Westhoff et al. (2012) for all eight Nepalese 8000ers by multivariate analysis: the odds of death was associated with summit success (odds ratio: 1.50; 95% confidence interval: 1.03 to 2.19; p=0.036). These findings clearly demonstrate the inhomogeneous risk distribution during an expedition.
Ascent versus descent
Publications that differentiate between fatalities occurring during ascent and descent are sparse. In the Nepalese Himalayas (1970 to spring season 2010), a total of 235 fatalities occurred among members of traditional expeditions during their summit bid (45% of all deaths) compared to 43 fatalities (78% of all deaths) among members of commercial expeditions (Westhoff et al., 2012). In both cases, the fraction of fatalities occurring during descent (73% for traditional expeditions; 95% for commercial expeditions) was much higher than during ascent. The higher likelihood of death during ascent to the summit for traditional expeditions may reflect a tendency to select more non-standard routes compared to commercial expeditions (Westhoff et al., 2012). A similar result was obtained on Denali (Alaska): 61% of all fatalities occurred during descent and 21% during ascent (McIntosh et al., 2008). In contrast, for Mount Rainier (Cascade Range, WA) an even distribution of fatal incidents (13 during ascent, 13 during descent, 3 unknown) was observed (Christensen and Lacsina, 1999).
Risk predictors and confounding
The risk estimates discussed above may be confounded by a number of variables related to the person attempting a high peak (gender, age, citizenship, experience, summit arrival time, expedition type, use of supplementary oxygen), the environmental conditions (altitude, peak, season), and calendar year.
Human factors
Gender
High altitude mountaineering is certainly dominated by men, but the exact fraction of women participating in these activities is only known for the Nepalese Himalayas. According to Salisbury and Hawley (2011), the percentage of women among expedition members above base camp almost doubled from 5.5% during the time period 1950–1989 to 10.5% during the years 1990–2009. An increase of the fraction of women (4.7 % for the years 1953–1989; 8.5% for 1990–1999; 10.3% for 2000–2005) was also observed on Everest (Huey et al., 2007). The values given for other time periods for the Nepalese Himalayas (10.2% females for the period 1970–2010; Westhoff et al., 2012) and Everest (7.8% females for the time period 1921–2006; Firth et al., 2008) fit into this general trend.
On Everest (spring seasons 1990–2005, members making their first attempt, Chinese expeditions excluded), the overall mortality (men 16.2/1000; women 16.3/1000; p=0.91) as well as the mortality during descent after summiting (men 23/1000; women 43/1000; p=0.20) are not depending on gender (Huey et al., 2007). A similar result was reported by Westhoff et al. (2012). With the aid of multivariate analysis including gender, age, Nepalese mountain experience, type of expedition, use of standard route, peak, summit success, season, and year of expedition as covariates, it was shown that on Nepalese 8000 m peaks (1970 to spring season 2010) the odds ratio of death for males compared to females was 1.00 (95% confidence interval: 0.56–1.79).
However, these results are valid for 8000ers only. Looking at the unadjusted mortality data for different altitude strata reveals a more complicated pattern. According to Salisbury and Hawlwy (2011), men have an almost 10-fold higher mortality on 7000ers than women (men 21.2/1000; women 2.8/1000; p=0.001). For 8000ers (men 17.1/1000; women 14.5/1000; p=0.43), and for 6000ers (men 6.6/1000; women 3.7/1000; p=0.47) the differences were statistically insignificant (all data for the Nepalese Himalayas, expedition members, years 1950 to 2009). If the three altitude strata are pooled, the differences between men and women remain significant (men 16.1/1000; women 9.5/1000; p=0.004). The reasons for the large difference in mortality between men and women on 7000ers are currently not known. However, it is likely that peak and route selection contribute substantially to this observed difference.
It was proposed by Huey et al. (2007) that the similar odds of summiting, death overall, and death during descent after summiting on Everest for men and women may reflect similar physiological performances in hypoxia and cold. This conclusion is supported by the work of Westhoff et al. (2012) who found that, on the Nepalese 8000ers, the odds ratio for death among males compared to females was 1.00 (see above). We do not want to question the general hypothesis of similar physiological performance of men and women. However, the data presented in Salisbury and Hawley (2011) for 7000 m peaks need further attention. In addition, the fatality risk in mountaineering at lower altitude appears to be higher for men than for women. In Austria, for example, the risk of traumatic and sudden cardiac death in downhill skiing, ski mountaineering, mountain hiking, as well as rock and ice climbing was found to be substantially higher for men than for women (Burtscher, 1996; Burtscher et al., 1993, 1994, 1997a, b). Among elite mountaineers, a higher lifetime risk for fatal accident was observed for men compared to women, although not reaching statistical significance (Weinbruch and Nordby, 2010). In contrast, in the Swiss organisation “Youth and Sports,” incidence rates for injuries during alpinism were not significantly different for men and women (De Loës, 1995). However, mountaineering in “Youth and Sports” is generally supervised by qualified persons who may prevent or at least reduce risky behavior and, thus, even gender differences in risk taking.
Another interesting aspect of gender is the question of safety segregation. There is strong evidence that segregation of men and women at workplaces is related to the accident risk, and women generally appear to be more risk averse than men (e.g., DeLeire and Levy, 2001, 2004; Leeth and Ruser, 2006; Grazier and Sloane, 2008). A similar situation seems to exist in high altitude mountaineering in the Nepalese Himalayas (Fig. 1). If the fraction of women above base camp is plotted against the mortality for expedition members (males plus females; data from Salisbury and Hawley, 2011), two different regions can be recognized. For peaks with higher risks (mortality≥10/1000), the fraction of women above base camp appears to be constant between approximately 0.06 and 0.08. For safer mountains (mortality<10/1000) a higher fraction of women (>0.10) is observed (Fig. 1). Our analysis is restricted to peaks with more than 500 members above base camp in order to obtain meaningful risk estimates. For summits with less than 500 members above base camp, too many cases with no fatality (leading to a mortality of zero) are encountered. The observed difference in participation is remarkable, as it implies that a large fraction of women is aware of the variable risk levels at the different peaks in the Nepalese Himalayas.
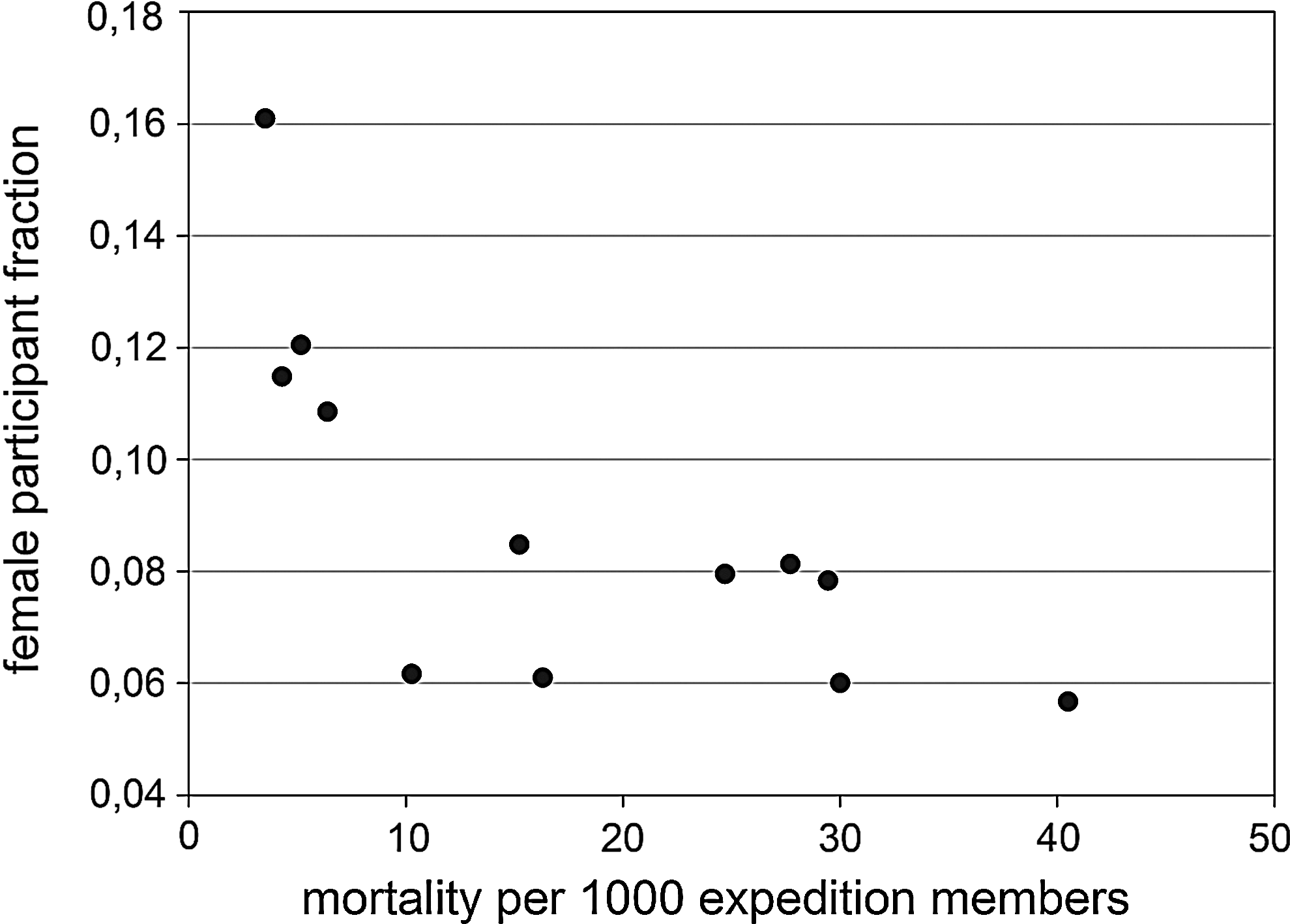
Safety segregation of women on mountains in the Nepalese Himalayas (peaks with more than 500 expedition members above base camp, data from Salisbury and Hawley, 2011).
Age
In the Nepalese Himalayas, the age distribution of expedition members shifted with time (Salisbury and Hawley, 2011). Whereas the majority of expedition members (all peaks) were in their late twenties to early thirties in the time period 1950 to 1989, a shift to an older age and a widening of the age distribution was observed for the time period 1990 to 2009 (Salisbury and Hawley, 2011). A shift to older ages was also reported for Everest (Huey et al., 2007). According to these authors, the fraction of expedition members older than 39 years increased from 19% for the years 1953–1989, 35% for the years 1990–1999 to 46% for the years 2000–2005. Approximately 87% of expedition members attempting a Nepalese peak during the time period 1970–2010 had an age between 20 and 50 years (Westhoff et al., 2012).
The age-specific mortality in high altitude mountaineering was only addressed in a few publications. On Everest (years 1990–2005; expedition members making their first attempt), the mortality remains constant until an age of approximately 60 years and then strongly increases (Huey et al., 2007). The overall mortality was more than three times higher for sexagenarians compared to younger climbers (50/1000 vs. 15/1000), during summit descent even more than ten times higher (250/1000 compared to 22/1000). A similar pattern is reported by Salisbury and Hawley (2011) for the commercial routes on Ama Dablam, Cho Oyu, and Everest (years 1990–2009): the mortality remains approximately constant until an age of 60 years and then strongly increases. A completely different pattern occurs for non-commercial peaks/routes (years 1950–2009) with the mortality steadily declining with age and approaching zero at an age of 65 years (Salisbury and Hawley, 2011). If all peaks are grouped together, no pronounced age dependence of the mortality is found (Salisbury and Hawley, 2011), indicating that the two different age trends cancel each other out. However, it should be kept in mind that the mortality data discussed above are not controlled for confounding. The oppositional trend between commercial and traditional expeditions may be responsible for the observation of Westhoff et al. (2012) that, for 8000ers in Nepal, the age is not associated with the odds of death (odds ratio: 1.01; 95% confidence interval: 0.99 to 1.03; p=0.28). According to McIntosh et al. (2008), also on Denali (Alaska) age is not a significant factor in fatality (p=0.11).
If other mountain sports are regarded, a more complex pattern is observed. For example, the mortality of trekking in Nepal seems to be independent of age, as the frequency of death above 50 years and below 50 years was found to be identical for the time period from January 1984 to June 1987 (Shlim and Houston, 1989). However, according to Shlim and Gallie (1992), the mean age of trekkers in Nepal who died increased from 35±13 years for the period January 1984–June 1987 to 44±16 years for the period July 1987–1991, although not reaching statistical significance (p<0.08).
For mountain sports at lower altitudes, the different disciplines must be discussed separately. In Austria (Burtscher et al., 1994, 1997a), the risk of traumatic death during mountain hiking, ski mountaineering, and downhill skiing increases with increasing age for men. The same is true for women except for downhill skiing where too few fatalities prevent analysis. For rock climbing, the risk of traumatic death increases with age to a maximum at an age of 45–59 years, and then decreases again, irrespective of gender. The risk of sudden cardiac deaths increases in all four disciplines with age for men (for women, the low number of fatalities prevents any meaningful analysis).
The age-specific mortality of elite climbers shows a pronounced maximum for the age interval of 30–39 years, and it is remarkable that this maximum in the age distribution is stable over a time period of 130 years (Weinbruch and Nordby, 2010).
Citizenship
Citizenship appears to be a significant confounder of mortality in high altitude mountaineering. According to Salisbury and Hawley (2011), mortality of mountaineering in Nepal (years 1950–2009) varies between different countries from 56.9/1000 (Slovakia) to zero (several countries including Norway, Ireland, South Africa). The highest values (>30/1000) are observed for citizens from Eastern European countries (Slovakia, Romania, Hungary, Bulgaria, Czechoslovakia, Slovenia) as well as for Greece and Argentina. It was suggested by Salisbury and Hawley (2011) that the higher mortality of mountaineers from Eastern Europe may be the result of a higher proportion of climbers attempting difficult routes or of budgetary concerns leading to the use of minimal or inferior equipment.
Pronounced differences in mortality as function of origin of the mountaineers were also found on Denali (Alaska). According to Lattimore (1993), the following mortalities were observed for the time period 1978–1987: Asia (14.8/1000), Europe (10.1/1000), North America (2.0/1000), and Africa, South America, or Australia (no fatalities). The risks for Asian and European mountaineers were significantly higher than the average (p<0.005). The high mortality for mountaineers from Asia was corroborated by McIntosh et al. (2008) who reported an odds ratio relative to North Americans (time period 1903–2006) of 3.6 (95% confidence interval: 1.6–8.3, p=0.002). For European mountaineers, the odds ratio (relative to North American mountaineers) for mortality on Denali (1.4, 95% confidence interval: 0.61–3.4, p=0.41) was not statistically significant (McIntosh et al., 2008). The higher mortality of Asians and Europeans may be related to a tendency of faster ascent than the 1000 ft/day recommended, as noted by climbing rangers (Lattimore, 1993). According to McIntosh et al. (2010), the probability to require a rescue is also significantly higher (relative to North Americans) for climbers from Asia (odds ratio: 4.1; 95% confidence interval: 3.0–5.8) and from Europe (odds ratio: 1.40; 95% confidence interval: 1.04–1.89).
For elite climbers from Austria, France, Germany, Italy, Switzerland, and the United Kingdom, a homogeneous distribution (p=0.79) of the lifetime risk of fatal mountaineering accident was reported by Weinbruch and Nordby (2010).
Experience
In contrast to the beliefs of many mountaineers (for an illustration, see Westhoff et al., 2012), prior experience on Nepalese peaks seems to have no effect on mortality. According to Huey et al. (2007), climbers on Everest (years 1990–2005; expedition members making their first attempt) with prior experience on a Nepalese peak have a higher summiting rate (39% versus 26%, p<0.001) but the same mortality as climbers without such experience (18/1000 versus 15/1000, p>0.6). A similar result was reported by Westhoff et al. (2012) for 8000ers in Nepal (1970–spring season 2010): after controlling for gender, age, peak, season, use of standard route, summit success, and calendar year, the number of expeditions to peaks in Nepal is not associated with a change in mortality (odds ratio=1.00, 95% confidence interval: 0.96–1.05, p=0.904). In addition, survival analysis (Kaplan-Meier analysis) revealed a linear association between the cumulative mortality and the number of expeditions (i.e., no survival benefit is associated with increased Himalayan experience) (Westhoff et al., 2012). However, both studies are limited to experience gained on Nepalese mountains, high altitude mountaineering experience gained in other countries is not regarded. Also on Denali (Alaska), experience seems not to have any protective effect. According to Lattimore (1993), no significant difference in climbing experience exists on this mountain between search and rescue objects and a control group of randomly selected non-rescued climbers.
Experience may even possibly increase risk of mortality in a mountain sport. According to Burtscher and Nachbauer (1999), the risk of fatal avalanche accident during back country skiing in Austria (1986–1995) is significantly higher for members than for non-members of mountaineering associations (relative risk=1.9; 95% confidence interval: 1.1–3.2). As about 55 % of the members reported to engage in one or more training courses or information sessions each year, it was assumed by Burtscher and Nachbauer (1999) that they have a higher level of training and experience than non-members.
Summit arrival time
The summit arrival time depends on a number of factors, including personal level of fitness and skills, traffic on route, weather conditions, and expedition style. However, as the decision to return before the summit is reached if the time is running late is primarily in the responsibility of each mountaineer, the summit arrival time is regarded by us as a human factor.
On Everest, most survivors (expedition members and high altitude porters) summited between 6
Expedition type
The effect of commercialization on survival in mountaineering on Nepalese 8000 m peaks (January 1970–spring 2010) was investigated recently by Westhoff et al. (2012). According to these authors, members of commercial expeditions were more likely than members of traditional expeditions to summit (44% vs. 28%) and less likely to die (7/1000 vs. 17/1000). Multivariate analysis revealed that the lower odds of death during commercial expeditions is not statistically significant (odds ratio=0.63; 95% CI: 0.37–1.1; p=0.10). Mountaineers of traditional expeditions most likely died during the route preparation phase (47%) or their summit bid (45%) in contrast to commercial expeditions where most members (78%) died during their summit bid and a much smaller fraction (13%) during route preparation (Westhoff et al., 2012).
On Denali (Alaska), the hiring of a professional guide had no protective effect. The fraction of groups accompanied by a professional guide was identical for search and rescue objects compared to a control group of nonrescued climbers (Lattimore, 1993). On the other hand, approximately 70% of the fatalities on the same mountain involved unguided expeditions (McIntosh et al., 2008). However, as the average team size of guided and unguided expeditions is not known, the significance of this observation cannot be judged.
There are indications that being a member of an organized group may lead to increased risks. In trekking in Nepal (July 1987–December 1990), 77% of the fatalities from high altitude sickness occurred in organized groups (Shlim and Gallie, 1992). As the fraction of people trekking in organized groups is estimated to be only approximately 40%, trekking in an organized group appeared to be a risk factor for dying from high altitude sickness (p<0.01). The risk for dying from trauma or other illness was not significantly different from unorganized trekkers. It is speculated by Shlim and Gallie (1992) that the tight schedule of organized groups, competition between group members, and the pressure on tour leaders to avoid the logistic difficulties arising when members are left behind may explain this remarkable observation.
Two other aspects of expedition style are team size and ratio between hired personnel and expedition members. Both parameters seem to have no systematic influence on mortality, except for solo climbers on Everest who have a much higher mortality than teams consisting of two or more members (Salisbury and Hawley, 2011).
Oxygen use
The potential influence of the use of supplementary oxygen on mortality during high altitude mountaineering was first studied by Huey and Eguskitza (2000). On Everest and K2 (years 1978–1999), the use of supplementary oxygen led to a significant (p<0.001) reduction of the odds of death during descent from summit. On Everest, 32 fatalities were observed among 1077 ascents with supplementary oxygen compared to 8 fatalities among 96 ascents without use of supplementary oxygen, for K2 the corresponding numbers are 0 fatalities out of 47 ascents versus 22 fatalities out of 117 ascents. Controlling for non-independence of climbers (by analyzing summit teams instead of individual climbers) corroborated the association between the use of supplemental oxygen and decreasing mortality during summit descent (p=0.03). As already discussed by Huey and Eguskitza (2000, 2001), this observed association may be causal due to the higher physiological stress from hypoxia. However, other explanations, as for example, mountaineers using supplementary oxygen are more risk averse or are better equipped, cannot be ruled out presently (Huey and Eguskitza, 2000; Huey et al., 2001).
More detailed data on the association between the use of supplementary oxygen and mortality on Nepalese 8000ers was published recently (Salisbury and Hawley, 2011). Only for Everest, a significant difference (on the 5% level) in mortality during descent from summit was observed between expedition members using and those abstaining from supplementary oxygen. For the other Nepalese 8000 m peaks, mortality during descent from summit shows no clear association with the use of supplementary oxygen. The same is true for mortality above the highest camp for all Nepalese 8000ers including Everest (Salisbury and Hawley, 2011).
Environmental factors
Altitude
The relation between the height of a mountain and overall mortality was investigated by Huey and Eguskitza (2001) based on a very limited number of peaks (Rainier 4392 m, Foraker 5306 m, Denali 6193 m, K2 8616 m, Everest 8850 m). According to these authors, the overall mortality significantly increases with altitude (p=0.04) and is significantly higher for the two 8000ers (p=0.04).
As the overall mortality was known for only a few peaks, Huey et al. (2001) investigated the mortality during summit descent for all 8000ers from the year of first ascent through the year 2000. On Everest and K2, climbers using supplemental oxygen were excluded, the use of oxygen on other peaks was neglected. In total, 145 fatalities occurred after 3803 ascents, leading to an overall incidence proportion of 38.1/1000. The incidence proportion varied between 173/1000 on K2 and 4/1000 on Cho Oyu. The mortality increased significantly with altitude (linear regression; r2=0.39; p=0.009). The association between mortality during descent from summit and altitude remained significant after controlling for confounding factors (use of supplemental oxygen, individual strong storm events, elevation difference between base camp and summit). This association is remarkable, as the maximum altitude difference of the peaks studied by Huey et al. (2001) is only approximately 800 m.
More detailed data on the overall mortality on individual mountains in Nepal (years 1950–2009) became available recently (Salisbury and Hawley, 2011) and are shown in Figure 2 as a function of altitude. Displayed are only peaks with more than 500 expedition members above base camp (for summits with less than 500 members above base camp, too many cases with no fatality, leading to a mortality of zero, are encountered). In agreement with the findings of Huey and Eguskitza (2001), the overall mortality on Nepalese peaks is associated with altitude (r2=0.13). However, the large deviations from the regression line (logistic regression, this contribution) indicate that the different peaks have their individual characteristic (e.g., technical difficulty, avalanche risk) which has a strong effect on overall mortality. Nepalese peaks with high overall mortality (>20/1000) include Annapurna I, Dhaulagiri I, Kangchenjunga, Manaslu, and Pumori; the safest peaks (overall mortality<10/1000) are Ama Dablam, Annapurna IV, Baruntse, and Cho Oyu. Unfortunately, the multivariate analysis carried out by Westhoff et al. (2012) was limited to peaks with an altitude above 8000 m. Thus, no further conclusions can be drawn from their publication.

Mortality of expedition members as function of altitude (Nepalese peaks with more than 500 expedition members above base camp, data from Salisbury and Hawley, 2011).
It is interesting to note that also for trekking in Nepal (January 1984–June 1987) altitude appears to play a minor role in mortality (Shlim and Houstan, 1989). Based on the even distribution of the number of deaths (not the incidence proportion!) in the different altitude ranges between 2000 and 6000 m, it was concluded by these authors that the main risks of trekking are not related primarily to altitude but to the hazardous terrain and to illness occurring in a remote area. In contrast, an obvious increase of mortality during trekking with altitude was mentioned by Burtscher et al. (1995) and Huey and Eguskitza (2001): 2.3 deaths per 106 exposure days for England and Wales (Avery et al., 1990), 5.7 per 106 exposure days for Austria (Burtscher et al., 1995), and 10.6 per 106 exposure days for Nepal (Shlim and Houstan, 1989). However, as mortality during trekking is affected by many other factors than altitude, Huey and Eguskitza (2001) concluded that these data are suggestive at best.
Peak
As discussed in the previous paragraph, different peaks seem to have their individual risk characteristics depending, beside altitude, on a number of factors such as, for example, technical difficulty, rock quality, and avalanche risk (see also Fig. 2). Indeed, in a multivariate analysis (Westhoff et al., 2012), the choice of peak was significantly (p<0.001) associated with the odds of death on Nepalese 8000ers (January 1970–spring season 2010).
Season
Data for different climbing seasons are only available for the Nepalese Himalayas, where most climbing activity (approximately 95% of expedition members above base camp; 1950–1989) takes places during spring (March to May) and autumn (September to November) due to favorable weather conditions (Salisbury and Hawley, 2011). The ratio of climbers between spring and autumn strongly depends on the region within Nepal. The western regions attract more climbers (expedition members above base camp; 1950–2009) in autumn (approximately 2/3 in autumn, 1/3 in spring), the eastern regions more in spring (50%–65 % in spring and 35%–50 % in autumn).
The climbing season seems to have a marginal influence on mortality. According to Huey and Salisbury (2003), the mortality of expedition members on Everest (1980–2002) is similar in autumn and spring on both the South Col (19/1000 vs. 14/1000) and the North Col route (11/1000 vs. 18/1000), despite the fact that the success rate is much lower in autumn. A similar result was obtained by Salisbury and Hawley (2011) for the time period 1950–2009 and all Nepalese peaks: the difference in mortality between seasons is statistically insignificant for expedition members. Multivariate analysis by Westhoff et al. (2012) for Nepalese 8000ers (January 1970–spring 2010) showed that season is not associated with the odds of death (p=0.91). Also for trekking in Nepal, a similar mortality was found for the spring and autumn season (Shlim and Houston, 1989).
Calendar year
Huey and Salisbury (2003) were the first to study the time dependence of mortality in high altitude mountaineering. For Everest (all routes) and the spring seasons from 1980 to 2002, they found no significant change for expedition members.
Later studies, which investigated a longer time period and a larger number of peaks, did not corroborate these findings. According to Salisbury and Hawley (2011), a steady decrease in mortality is observed in the Nepalese Himalayas (all peaks) from the 1970s onward with 34.9/1000 members above base camp for the time period 1970–1974 to 9.2/1000 members above base camp for 2005–2009. From 1950 until 1970, the data were unstable due to the much lower number of climbers. Alike, mortality on Nepalese 8000ers (expedition members, January 1970–spring 2010) was found to decrease significantly (p=0.01) with calendar year (Westhoff et al., 2012). Multivariate analysis yielded an odds ratio of death with every unit change of year of 0.98 (95% confidence interval: 0.96–0.99).
A decreasing mortality with calendar year was also reported for Denali (Alaska). According to McIntosh et al. (2008), mortality on Denali decreased an average of 4% each year from 1932 (the first fatality occurred in this year) to 2006 (odds ratio: 0.96; 95% confidence interval: 0.95–0.98; p<0.0005). A part of this reduction seems to be related to the introduction of a registration system by the National Park Service in 1995. The mortality decreased from≈14/1000 climbers in the early 1970s to≈0.6/1000 during 2000–2006. Compared to the Nepalese Himalayas (Salisbury and Hawley, 2011), the decrease on Denali is more pronounced (i.e., is higher by a factor of approximately 6).
Occupational Exposure
Occupations involved in high altitude mountaineering include high-altitude porters, lowland porters (to carry loads to the base camp), base camp personnel, and professional mountain guides. Currently, mortality data are only available for high altitude porters in the Nepalese Himalayas (Huey and Salisbury, 2003, Firth et al., 2008; Salisbury and Hawley, 2011). Compared to expedition members, the knowledge on mortality of high altitude porters is rather limited. The information may be unreliable, as pointed out by Firth et al. (2008) for age data, or missing completely (e.g., mountaineering experience, summit arrival time, oxygen use).
Overall risk estimates
According to Salisbury and Hawley (2011), a significantly lower mortality in the Nepal Himalayas (all peaks) was observed for high altitude porters (18.5/1000) compared to expedition members (25.4/1000) in the years 1950–1989 (risk ratio=0.73; 95% confidence interval: 0.59–0.89). In the time period 1990–2009, the mortality was lower for both groups (9.1/1000 for porters and 10.7/1000 for expedition members), but the risk reduction seems to be more pronounced for expedition members, as the risk ratio is not significant any more (0.85; 95% confidence interval: 0.68–1.07).
On individual peaks a more complex situation emerges. In Table 4, the mortality (years 1950–2009) of high altitude porters is listed for all peaks with more than 500 expedition members above base camp, which corresponds to a number of at least 208 high altitude porters above base camp (data from Salisbury and Hawley, 2011). The overall mortality of high altitude porters is for most peaks not significantly different from expedition members. Two exemptions are Baruntse and Everest with a significantly higher and lower mortality for high altitude porters, respectively. However, as the value for Baruntse is based on a small number of fatalities for both expedition members and porters, the risk ratio has a large uncertainty. A significantly lower mortality for porters compared to expedition members on Everest was also reported by Huey and Salisbury (2003) and Firth et al. (2008).
Inhomogeneity of risk estimates
As for expedition members, the incidence proportions for high altitude porters summarized in Table 4 are crude estimates. The risks are not distributed homogeneously on a given mountain and during the course of an expedition.
The distribution of fatalities on a given route is only reported by Firth et al. (2008) and Salisbury and Hawley (2011). According to the former, fatal incidents on Everest involving high altitude porters occurred on average at a significantly (p<0.001) lower altitude (6927±116 m; mean value±1 standard deviation; 44 incidents) than for expedition members (7854±918 m; 103 incidents). Expedition members and high altitude porters seem to die predominantly during different phases of an expedition. On the standard routes of Everest (1982–2006, spring season) 82% (n=51) of the fatalities among expedition members occurred during the summit bid and only 18% (n=11) during route preparation. For high altitude porters, the relative proportions are almost reversed: 27% (n=4) of the fatalities occurred during the summit bid and 73% (n=11) during route preparation (Firth et al., 2008). If all Nepalese peaks and the time period 1950–2009 are regarded, the difference between expedition members and high altitude porters is less pronounced (Salisbury and Hawley, 2011). An equal proportion of fatalities of expedition members occurred during the summit bid (44%, n=266) and during route preparation (44%, n=270). Still, a much higher fraction of high altitude porters died during route preparation (55%, n=122) than during the summit bid (13%, n=28). The different location of fatal incidents for expedition members and high altitude porters is also obvious when looking at individual Nepalese 8000 m peaks as well as different altitude strata (Salisbury and Hawley, 2011). With the exemption of Kangchenjunga, the mortality for high altitude porters on Nepalese 8000ers is higher at or below highest camp compared to above highest camp. The same is true if all Nepalese peaks and the three altitude ranges of 6000ers, 7000ers, and 8000ers are regarded (Salisbury and Hawley, 2011).
Mortality data for different routes on the same mountain are also sparse. According to Huey and Salisbury (2003), the differences in mortality of high altitude porters on the different routes on Everest (N-ridge: 1.8/1000, SE ridge: 8.4/1000, other routes: 3.0/1000) are not statistically significant. If standard and nonstandard routes on Nepalese 8000ers are compared (Salisbury and Hawley, 2011), it appears that the mortality for high altitude porters (at or below highest camp) is generally larger on the latter. An especially large increase in risk on nonstandard routes is observed for Makalu and Cho Oyu.
Mortality during descent from summit is also generally lower for high altitude porters than for expedition members. According to Huey and Salisbury (2003), the overall mortality during descent from the summit of Everest (1980–2002, spring season) is 6.1/1000 for high altitude porters and 34.5/1000 for expedition members (risk ratio=0.18; confidence intervals cannot be calculated as the number of expedition members and porters is not given). This result was corroborated by Firth et al. (2008) for the standard routes on Everest (1982–2006; spring season). The mortality during descent from summit was significantly (p<0. 001) lower for high altitude porters (4.1/1000) than for expedition members (27.1/1000).
Risk predictors and confounding
Human factors which may confound the crude risk estimates (gender, age, citizenship, experience, summit arrival time, expedition type, use of supplementary oxygen) were not investigated to date for high altitude porters. The influence of gender may be impossible to study, as the number of females employed as high altitude porters is very small. At Everest (years 1921–2006), for example, only 2 out of 6108 high altitude porters were females (Firth et al., 2008). Age data were considered to be unreliable and, thus, not analyzed (Firth et al., 2008). A meaningful analysis of the influence of supplemental oxygen on mortality is prevented by the small number of fatalities among porters on summit bids (Salisbury and Hawley, 2011). The summit arrival time for survivors and non-survivors (Firth et al., 2008) are not reported separately for expedition members and porters. The same is true for the data on use of supplemental oxygen (Huey and Eguskitza, 2000; Huey et al., 2001).
Environmental factors that may confound the crude risk estimates for high altitude porters include altitude, peak, and season. The influence of altitude and peak can be estimated only from the data given in Salisbury and Hawley (2011). The overall mortality of high altitude porters on individual mountains in Nepal (years 1950–2009) is shown in Figure 3 as a function of altitude. In our analysis, only peaks with more than 500 expedition members above base camp are displayed, which corresponds to a number of at least 208 porters above base camp. In contrast to expedition members, the overall mortality on Nepalese peaks is not significantly correlated with altitude. The odds ratio for every increase in altitude of 1000 m (adjusted for member/porter status) is 1.2 (95% confidence interval: 1.1–1.4). Nepalese peaks with high overall mortality for high altitude porters (>20/1000) include Annapurna I, Dhaulagiri I, Makalu, Manaslu, Pumori; the safest peaks (overall mortality<10/1000) are Ama Dablam, Annapurna IV, Cho Oyu, Everest, and Lhotse. The different peaks appear to have their individual characteristic (technical difficulty, rock quality, avalanche risk) which has a stronger effect on overall mortality than altitude.
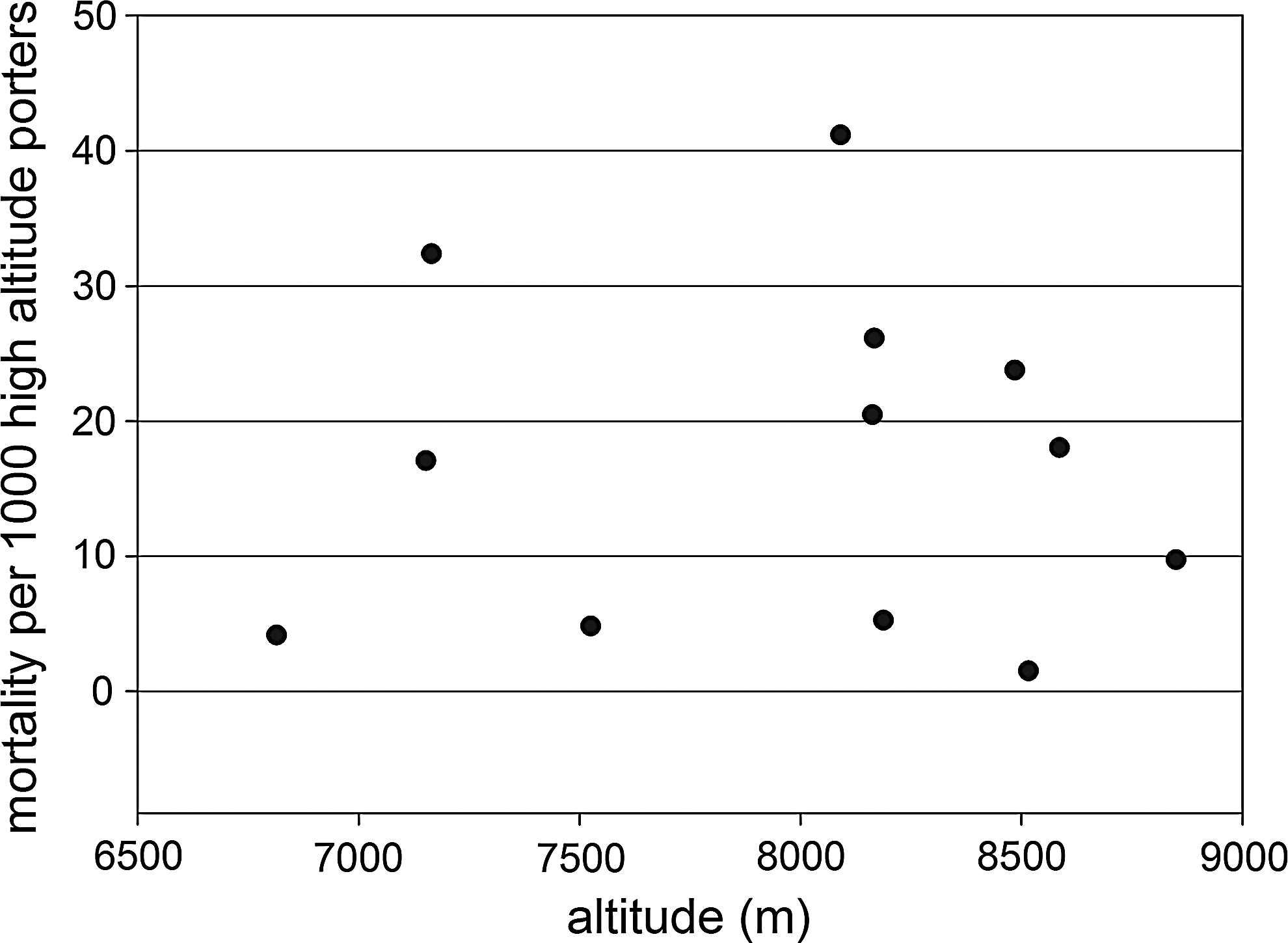
Mortality of high altitude porters as function of altitude (Nepalese peaks with more than 500 expedition members above base camp, data from Salisbury and Hawley, 2011).
As already mentioned above, data for different climbing seasons are only available for the Nepalese Himalayas, where most climbing takes places during spring and autumn. In contrast to expedition members, the mortality of high altitude porters on Everest (years 1980–2002) is significantly higher in autumn than in spring for both, the South Col (21/1000 vs. 8/1000) and North Col (28/1000 vs. 2/1000) routes (Huey and Salisbury, 2003). A statistically significant higher mortality for autumn compared to spring on Everest was also reported by Salisbury and Hawley (2011) for the time period 1950–2009. Looking at individual mountains reveals a more complex pattern: the mortality of high altitude porters may be substantially higher in autumn than in spring (Annapurna I, Baruntse, Everest, Kangchenjunga) as well as lower (Dhaulagiri I, Manaslu). However, except for Everest, these differences do not reach statistical significance on the 5% level. If all Nepalese peaks are grouped together, the higher mortality of high altitude porters in autumn compared to spring is statistically significant (Salisbury and Hawley, 2011).
According to Huey and Salisbury (2003), the mortality of high altitude porters on Everest (all routes, spring season) did not change significantly with calendar year (1980–2002). In contrast, a steady decrease in mortality of high altitude porters from the 1970s onward was reported by Salisbury and Hawley (2011) for the Nepalese Himalayas (all peaks). From 1950 until 1970, the data were unstable due to the lower number of high altitude porters.
Suggestions for Further Studies
Although the number of publications on mortality during high altitude mountaineering has increased substantially, quantitative risk estimates are available mainly for the Nepalese Himalayas and Alaska (USA). Thus, additional studies from other high altitude mountain ranges are certainly required to check the consistency of the published risk estimates. In principal, all mountains requiring permits (thus enabling detailed records of mountaineering activity) and attracting a large number of climbers (e.g., the Russian Pamir, Kilimanjaro in Tanzania, or several National Parks in South America) are well suited for such studies. In addition, studies from cold regions (Antarctica, Greenland, Spitsbergen) could help to separate the effects of high altitude (i.e., low oxygen partial pressure) from low temperature and strong winds.
Another desideratum is the conduction of well-designed prospective cohort and case-control studies to address the role of potential confounders such as gender, age, citizenship (as a proxy for risk cultures), and previous mountaineering experience. As discussed in detail above, the literature on these topics is currently inconclusive, clearly underlining the need for further work.
Although being a seminal paper on mortality in high altitude mountaineering, the multivariate analysis published by Westhoff et al. (2012) did not include altitude, citizenship, and use of supplementary oxygen as covariates. All three parameters were previously shown to be potential confounders. Thus, the unique data set contained in The Himalayan Database (American Alpine Club, 2004; updated bi-annually) should be re-analyzed with these parameters included.
Finally, the mortality of high altitude porters was not studied thoroughly. This is partly caused by incomplete or unreliable data. However, prospective cohort studies could possibly close this gap of knowledge in the future.
Note Added to Proof
Since acceptance of the manuscript three additional articles with relevance for the present review were published. The most important findings of these articles are summarized here.
An overall mortality of 0.77/1000 mountaineers was reported for Aconcagua (Argentina) for the years 2001–2012 (Westensee et al., 2013), which is considerably lower than the values reported for other mountains with an altitude above 6000 m.
Using advanced statistical techniques from reliability engineering (total time on test transform), it was shown by Cheng (2013) that the risk of death for expedition members on Nepalese 8000 m peaks is consistent with a constant failure rate. This finding corroborates the conclusion of our review that prior high altitude mountaineering experience in Nepal has no protective effect.
According to Sherman and Chatman (2013), nationally diverse expeditions are more likely to experience injury or death than nationally homogeneous teams.
Footnotes
Acknowledgments
Reviews by Jeremy Windsor and an anonymous reviewer helped to improve the manuscript and are gratefully acknowledged.
Author Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose.