
Abstract
Abstract
Morrison, Shawnda A., Juri Gorjanc, and Igor B. Mekjavic. Mount Everest and Makalu cold injury amputation: 40 years on. High Alt Med Biol. 15:78—83, 2014—Freezing cold injuries (frostbite) of the extremities are a common injury among alpinists participating in high altitude expeditions, particularly during inclement weather conditions. Anecdotally, a digit that has suffered frostbite may be at greater risk to future cold injuries. In this case study, we profile a 62-year-old elite alpinist who suffered multiple digit amputations on both his hands and foot after historic summit attempts on Makalu (8481 m) and Mt. Everest (8848 m) in 1974–1979. We describe the clinical treatment he received at that time, and follow up his case 40 years after the first incidence of frostbite utilizing a noninvasive evaluation of hand and foot function to a cold stress test, including rates of re-warming to both injured and non-injured digits. Finger rates of recovery to the cold stress test were not different (0.8 vs. 1.0°C·min−1) except one (injured, left middle finger, distal phalanx; 0.4°C·min−1). Toe recovery rates after cold-water immersion were identical between previously injured and non-injured toes (0.2°C·min−1). Thermocouple data indicate that this alpinist's previous frostbite injuries may not have significantly altered his digit rates of re-warming during passive recovery compared to his non-injured digits.
Introduction
O
Case Report
A 62-year-old man presented to our laboratory 40 years after suffering multiple freezing cold injuries on both his hands and right foot. Within this follow-up testing, we wanted to determine the detailed patient history of how he suffered multiple frostbite injuries, and to what extent his peripheral vascular circulation is compromised 40 years after the initial incidence. The alpinist did not present with any specific symptoms related to his frostbite injuries. The protocol of this study was approved by the National Committee for Medical Ethics at the Ministry of Health of the Republic of Slovenia, and conformed to the Declaration of Helsinki guidelines. Written informed consent was obtained from the participant prior to participation in the study.
Patient history
Expedition 1. Makalu summit attempt (M1) 1974
During the first Makalu expedition, the alpinist was approaching the summit without supplemental oxygen when adverse weather conditions (high winds, poor visibility) forced the team to descend to Camp 5 (∼8100 m) for the night. Realizing he had suffered frostbite on the right middle finger distal phalanx, the alpinist descended below 8000 m, and with the expedition team, reached basecamp approximately 1 day later. He received no first aid or medications at that time (Table 1).
F, finger; LH, left hand; RF, right foot; RH, right hand; T, toe, 1–5 (digits affected) ; (↓), partial length amputations; (↕), full length amputations.
Expedition 2. Makalu summit–South Face (M2) 1975
Cold injury to the right foot was sustained at an approximate altitude of 8300 m, when the alpinist and a second climber were contemplating a summit push without supplemental oxygen. Of the four oxygen bottles they had carried to Camp 5 (∼8000 m), two were empty, one had a regulator malfunction, and only one was full. The alpinist had previously broken a crampon on his right foot, which he secured by tightly tying additional rope around his foot and ankle. He became very cold and decided to ascend. After the successful summit and descent to basecamp, the alpinist did not know his right foot was injured, and did not seek immediate medical attention. He awoke the next morning to see all five of his right toes (distal phalanges) blackened. The alpinist descended (hiking; 2 weeks) to Kathmandu on his frostbitten foot, but was not in a particular hurry since conventional alpine thinking at the time was “frostbite in January, amputation in June.”
Expedition 3. Everest summit attempt (EV) 1979
The alpinist took his gloves off at ∼8300 m to open a route that had never been climbed before (Everest Southwest ridge). He dropped his pack and supplemental oxygen by a narrow passage, and proceeded to climb the rock-face barehanded (Grade: French scale V), whilst carrying a rope to secure the route. After completing the climb, he put his gloves on and abseiled down to his pack below. He returned to Camp 5 (∼8200 m), but his fingers felt strange, and he knew that he had sustained frostbite (left middle and ring fingers, distal phalanges). Immediately, he heated water and rapidly re-warmed the fingers, aborting his climb. He returned to basecamp the next day where he stayed for 2 days, receiving intramuscular vasodilator injections. After 10 days in basecamp, he was flown by helicopter to Kathmandu.
Acute phase diagnosis and treatment
Each time he returned to Slovenia, he saw the head plastic surgeon of the University Clinical Centre who had experience treating frostbite injuries. For M1, necrosis of the right middle finger distal phalanx (F3) was identified and removed using the thenar flap technique, commonly used to resurface soft tissue trauma on the fingertips (Melone et al., 1982). This surgical technique, first described by Gatewood (1926), involves choosing a proximal flap (often the thumb skin crease parallel to the metacarpophalangeal joint), then utilizing a “W’ or “V”-shaped incision to create an elliptical full-thickness skin graft, which is then attached to the finger. In this case, a forearm flap was used to cover the thenar flap. The alpinist also underwent a surgical cervical sympathectomy, a procedure that severed and removed his right-side sympathetic ganglion, to promote immediate blood flow and potentially reduce future long-term pain. For both later expeditions (M2, EV), the alpinist's treatment began after the surgeon waited approximately 3 weeks for clear demarcation of the fingers or toes to appear. The alpinist and surgeon wanted to preserve as much digit tissue and bone as possible without sacrificing bone coverage, thus the surgeon opted for a cross-hand surgical implant technique. This involved guillotine of the necrotic tissue, some bone was denuded, and fingers implanted into the forearm of the contralateral side for 3–4 weeks. Once a full-thickness flap grew over the bone, the surgeon cut around the tissue so that the digit overtook adequate microcirculation. In this way, they achieved full covering of the denuded bone with quality skin flaps whilst still preserving generous digit length. The functional effect of having more digit length was critical to this alpinist's quality of life since he was a young man at the time of injury. On the right foot, this technique was not possible since the additional tissue would have created an “unstable” forefoot micro-flap that could roll with every footstep, since the thenar flap technique can replace lost digit pulp with full-thickness flaps, not just skin coverings. This feeling of instability was not acceptable to the alpinist; thus, full digit amputation of all five toes to the metatarsophalangeal joint was the preferred option.
Materials and Methods
Forty years following the first incidence of FCI, the alpinist participated in this follow-up investigation, approved by the National Committee for Medical Ethics of the Republic of Slovenia, in conformation with Declaration of Helsinki guidelines. We obtained written, informed consent prior to his participation in the study. Cold stress testing comprised of: submersing the hands and feet (individually, random order) for 5 min in 35°C water, then 30 min in 8°C water, and 10 min passive recovery in room air (21°C, 50% rh) (Felicijan et al., 2008). Briefly, we measured digit temperature on the dorsal surface (proximal to injury) of each nail bed using T-type thermocouples (Almemo, 5990-2, Ahlborn, Holzkirchen, Germany) logging every minute. In the case of amputation, we placed an additional, corresponding thermocouple on the same location on the uninjured, contralateral digit (Fig. 1). After arriving to the laboratory (21°C, 52% relative humidity) and instrumentation (∼20 min), the patient placed his hand or foot in a thin, plastic bag to avoid skin wettedness during water immersion. Skin temperature was also measured using infrared thermography (FLIR B335, FLIR Systems, Inc., Oregon, USA), which has been used in clinical settings to evaluate re-warming rates of patients with cold intolerance ( Ruijs et al, 2008; Davey et al., 2013). The camera was situated approximately 30-cm above the dorsal side of the hands or feet. Infrared skin temperature was measured immediately following the warm and cold bath, and after 5 and 10 min post immersion.

Schematic of thermocouple placements and infrared measurements on injured and non-injured digits. CON, control, non-injured digits of the corresponding, contralateral side; EQU, the equivalent testing location on the non-injured digits that correspond to the injured thermocouple placement sites; INJ, the injured digits.
Results
Examples of IR thermography data taken immediately after the cold bath are presented in Figure 2 for both the fingers and toes. Because IR thermography was taken at only specific time-points during the re-warming phase, data presented herein refer to the continuous thermocouple data. In the foot, there were no differences in individual toe digits' time-to-cool (25 min), or rate of re-warming (0.2°C·min−1). Minimum digit temperature was almost identical (9.0°C vs. 9.2°C) between the non-injured and injured toes (Fig. 3). Mean digit temperatures on the equivalent site of the non-injured foot remained ∼2°C higher during the 8°C bath, although re-warming rates were equivalent (0.2°C·min−1).
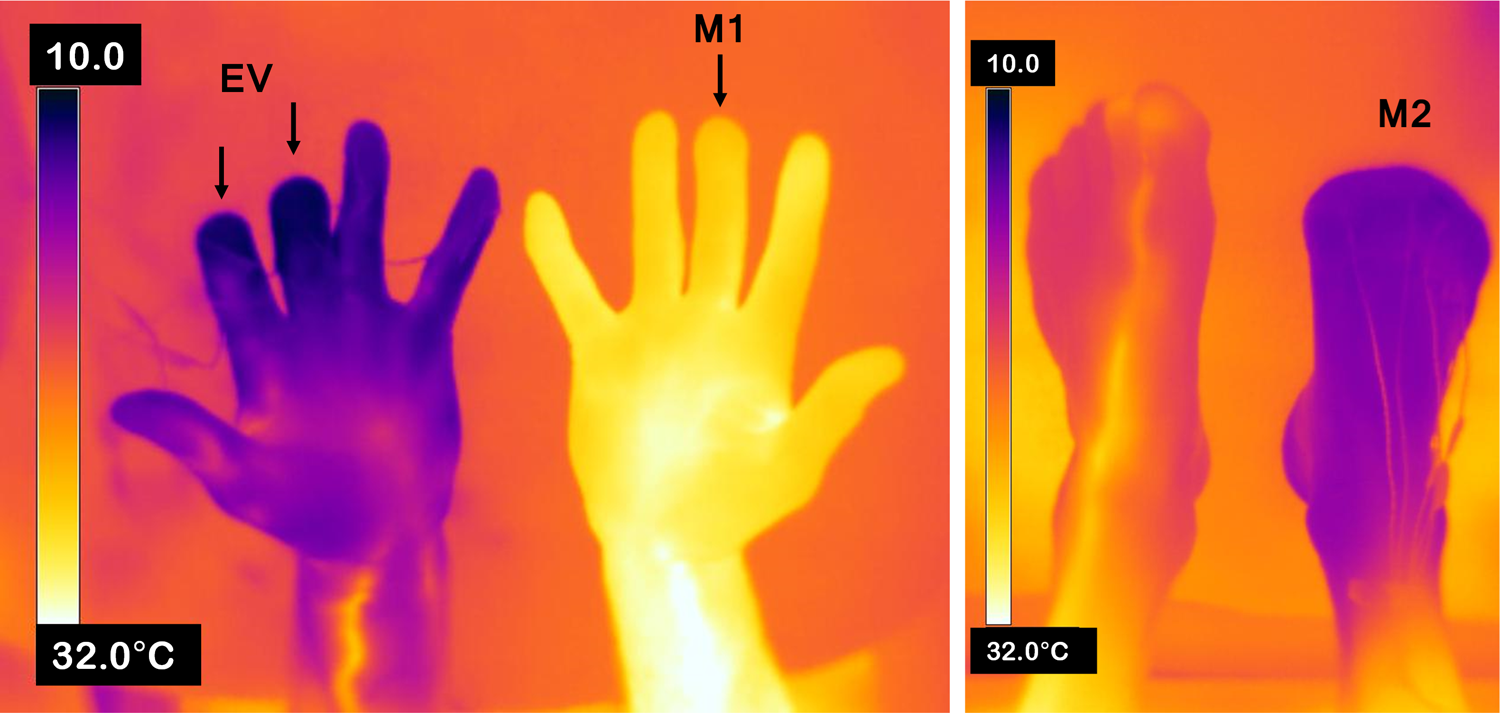
Infrared thermographs for fingers and toes identifying the injured digits. (M1) labels the frostbitten finger from Makalu 1 expedition, (EV) identifies the second and third fingers that were partially amputated following the Everest expedition, and (M2) identifies the full digit amputations on the right foot following Makalu 2 summit expedition. These thermographs were taken immediately following immersion in 8°C water for 30 min for the left hand, and later, the right foot.
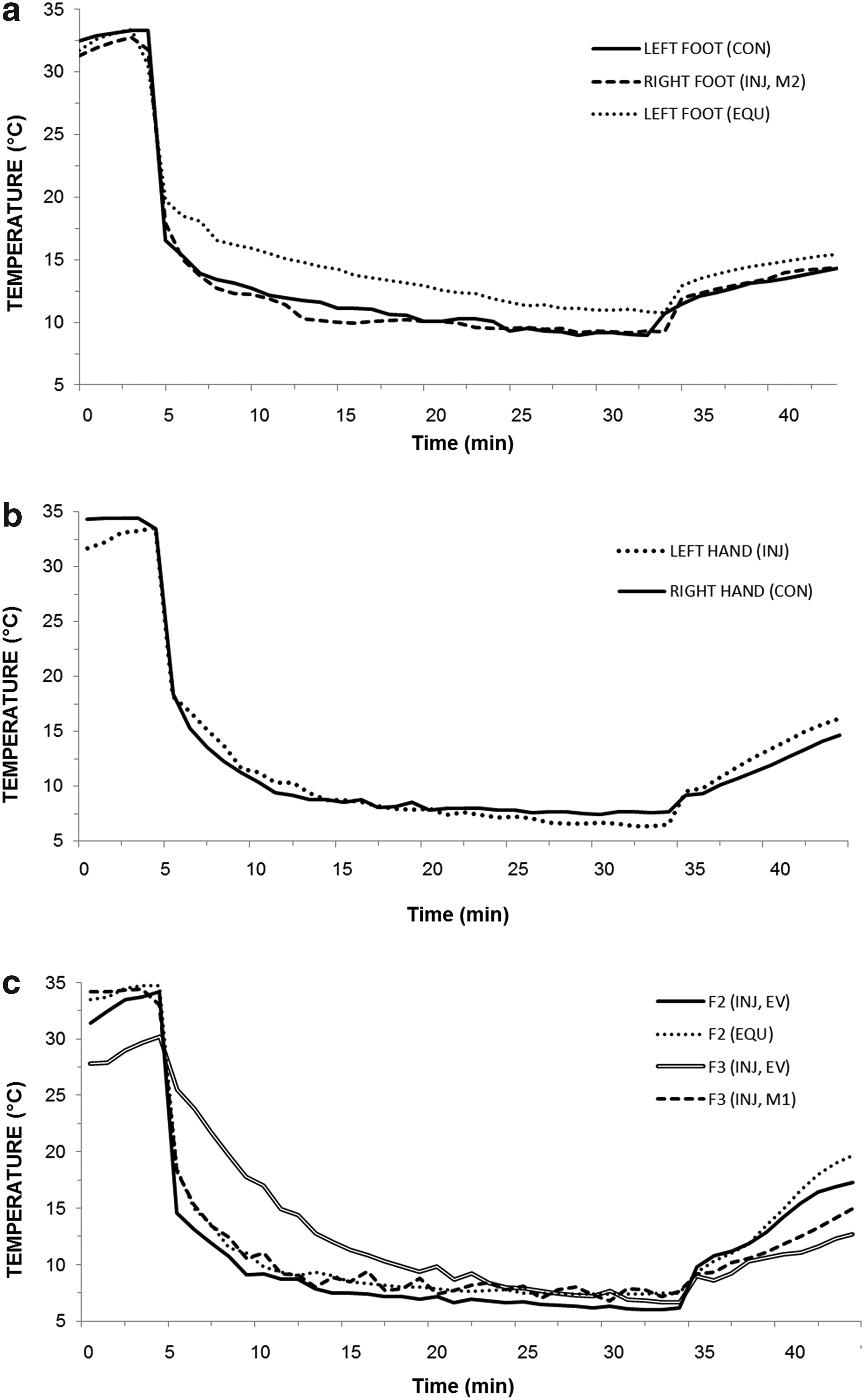
Thermocouple data throughout the cold stress test for
For the fingers, the left hand index finger (F2), which was injured during the EV expedition, showed a comparable thermal profile to its opposite side, uninjured digit (left F2 injured: 0.8°C·min−1, right F2 non-injured: 1.0 °C·min−1), as well as the other digits on its same left side (Thumb F1: 1.1, ring finger F4: 0.5, small finger F5: 0.7 °C·min−1, respectively). However, the left hand middle finger (F3), also injured from the EV expedition (0.4 °C·min−1), was lower, compared to its corresponding middle finger on the right hand (F3; 0.6°C·min−1), injured during the Makalu 1 expedition. Indeed, the left hand middle finger (F3) was a full 5°C colder following the 35°C warm bath, and yet 4°C warmer after 10 min in 8°C water than any other finger digit.
Discussion
The alterations in vasodilator/vasoconstrictor tone between the right and left side fingers may indicate lasting effects of the right-side sympathectomy performed in 1972. However, even the slowest recovering digit on the hand (left middle-finger distal phalange) exhibited faster re-warming rates than non-injured toes. The relevance of this finding indicates that autonomic function of the amputated digits was not as compromised as some frostbite literature suggests (Lazarus and Hutto, 1982; Zook et al., 1998; Hallam et al., 2010) (Table 2). Thermocouple placement and IR thermography was conducted directly on the random-pattern skin flaps, and not the native flesh of the frostbitten digits. Thus, we had hypothesized that it would behave differently (blunted, colder, and slower re-warming times) to native, uninjured tissue, hence placing “corresponding” thermocouple sites, to determine whether there were any differences between native and parasitic skin-flap testing locations.
The unremarkable differences between injured and non-injured digit skin temperatures and rates of re-warming were not expected. Admittedly, skin temperature is a gross surrogate for evaluation of total blood flow (both for nutritional and thermoregulatory purposes), but isolated cold stress testing does give an indication of how vascular beds respond to a physical stress (Ruijs et al., 2008; 2011; Davey et al., 2013), and should be considered when performing follow-up examinations. Since the injured left middle-finger distal phalanx did not respond adequately to either the heating or cooling phase, we would recommend that future cold stress tests include a warm, vasodilatation phase and a cold, vasoconstrictor phase in addition to the recovery period; they should also take place in a warm environment (>20°C) to encourage optimal peripheral cutaneous vasodilation in response to the cold stress test (Flouris et al., 2008).
Direct comparisons between right and left finger digits may not be appropriate in the present study due to the right-side sympathectomy of the patient. However, the only finger to exhibit augmented responses to both the warm and cold phase of the protocol was on the nonsympathectomized left-side middle finger (F3). Since there may have been lasting differences between digits due to the cervical sympathectomy alone, we determined temperature profiles for each injured digit individually, and suggest other researchers do the same when conducting follow-up examinations of freezing cold injuries, since marked differences can be observed both between-sides and within-digits.
Non-thermal factors to freezing cold injury
Behavioral thermoregulation plays a key role in the prevention of cold-related injuries. The alpinist in each case of frostbite made the conscious decision to continue climbing, even when weather, equipment failure, or a difficult route choice may have deterred other climbers from continuing under similar circumstances. Because he was young, fit, and an experienced alpine climber, this alpinist may have underestimated the risks of attaining frostbite due, in part, to his intense desire to summit in each expedition. That said, decision-making strategies and previous experience on high-altitude peaks do not necessarily confer increased survival, according to a large, retrospective cohort study investigating previous experience in Himalayan mountaineering (Westhoff et al., 2012). The authors investigated 23,295 non-porters on 8000 m peaks and found that positive learning experiences accrued over many climbs could be outweighed by other factors, including: new climbing objectives, or increased route difficulty. They propose the incremental decrease in climbing risk is a combination of cumulative knowledge throughout the climbing community and general innovations within the sport.
Alpine equipment and clothing has progressed greatly from the early 1920s to the latter half of the 20th century, such that attempting to scale Mt. Everest and Makalu with double-layer handmade leather boots and two-ply gloves (Table 1), as our alpinist had done, would not be recommended today. Historically, mountaineering clothing consisted of natural fabrics, including layering silk, wool, and cotton, which has been shown to be surprisingly effective, although ∼40% less insulative than modern synthetics (Rodway, 2012).
Frostbite as an “inevitable sequella to climbing” is not the case in modern mountaineering. Changes in attitude towards freezing cold injuries and frostbite are apparent when the alpinist declared that he ‘need not be rushed’ about seeking treatment for his right toes after the Makalu 2 expedition, since they would be amputated some 6 months later. Awareness of one's predisposition to frostbite, advances in thrombolytic therapy, including modern perfusion diagnosis techniques (reviewed by Hallam et al., 2010), can each affect the proportion of salvageable digit tissue if a frostbite does occur, although rapid access to these modern techniques continue to be a concern, especially for Himalayan alpinists. Indeed, in patients with severe frostbite but rapid thrombolytic therapy (within the first 24 h), high salvage rates have been reported (Twomey et al., 2004). Unfortunately, lack of appropriate clothing, inappropriate equipment use, and rapid access to medical therapy are still issues facing alpinists today (Harirchi et al., 2005).
Epilogue
Forty years on, this patient did not report any difference in cold sensitivity in his right side compared to pre-injury, or any particular problems with the sites of amputation due to frostbite per se. He did comment that his right eye had blurred vision after the operation, and that he continues to have ‘droop eye’, or Horner's syndrome, since the sympathectomy. However, he also noted that he found it very advantageous that his right palm did not sweat when climbing after the procedure. Critically, although this alpinist did suffer multiple cases of frostbite over 5 years, these injuries occurred in different locations each time, and none were repeat freezing at or near any original injury sites. The alpinist last summited an 8000 m peak in 2004 (Dhaulagiri, Nepal, 8167 m) at age 54. He found the climb one of his “easiest” yet, assisted by his improved cold injury precautions, acclimation techniques to high-altitudes, and advances in mountaineering equipment. He continues to climb today.
Conclusion
Utilizing a cold stress test to assess digit vascular responses yielded information regarding differential rates of individual digit re-warming. Of all the affected digits requiring amputation, only the injured middle finger of the left-hand (F3) presented significantly altered autonomic function. Since no significant differences were observed in digit temperature recovery rates after cold water immersion between previously injured and non-injured toes, peripheral blood flow during passive recovery may not be as compromised as originally hypothesized in this case study.
Footnotes
Acknowledgments
The authors would like to thank Dr. Rafael Šabec for his first-hand communication of the original surgical procedures performed in 1979, and to Dr. Metka Milčinski for her valuable feedback on manuscript preparation.
Author Disclosure Statement
The authors confirm there are no competing interests or any sources of funding used to complete this research.