
Abstract
Abstract
Kriemler, Susi, Flavia Bürgi, Christian Wick, Birgit Wick, Melanie Keller, Urs Wiget, Christian Schindler, Beat A. Kaufmann, Malcolm Kohler, Konrad Bloch, and Hans-Peter Brunner-La Rocca. Prevalence of acute mountain sickness at 3500 m within and between families: A prospective cohort study. High Alt Biol Med. 15:28—38, 2014.—
Methods:
87 children, 70 adolescents, and 155 parents (n=312) were assessed for AMS 8–10 and 20–24 hours after fast passive ascent by the Lake Louise Score (LLS). Pain sensitivity and oxygen saturation (SO2) were measured and familial clustering was assessed.
Results:
AMS prevalence was significantly lower in children (21%) compared to adolescents (34%) and adults (39%) on day 1 (p<0.05), but not on day 2 (18% vs. 19% and 25%). Cumulative prevalence of AMS was 30, 37, and 45% in children, adolescents, and adults, respectively (p<0.001). Familial clustering of AMS was consistent and explained 25%–50% of variability in AMS. Pain sensitivity significantly increased from low to high altitude and was higher at low altitude in those with compared to those without AMS. SO2 at high altitude was not related to the presence of AMS.
Conclusions:
After fast ascent to 3500 m, AMS prevalence was lower in children than in adolescents and adults on day 1, but not on day 2. Thus, children may travel at least as safely to an altitude of 3500 m as adolescents and adults, even if risk factors (pain sensitivity and heredity) are present.
Introduction
W
The precise pathogenesis of AMS is not yet clear. The existence of cerebral dysfunction possibly due to mild cerebral oedema as a consequence of inadequate acclimatisation to hypobaric hypoxia is the dominant hypothesis (Hackett and Roach, 2001; Imray et al., 2010). Yet, oxygen saturation (SO2) has been shown to be (Roach et al., 1998; Karinen et al., 2010) or not to be (Chen et al., 2012; Wagner et al., 2012) related to AMS. Furthermore, the individual's sensitivity to pain might play a role in determining the severity and prevalence of AMS symptoms (by sympathetic activation) as hypoxia is known to reduce the pain, taste, or tactile threshold to sensory stimuli as shown in nonacclimatized lowlanders upon acute exposure to HA (Noel-Jorand et al., 1996). Whether children perceive pain differently compared to adults under normoxic or hypoxic conditions that might potentially influence the occurrence or severity of AMS symptoms has never been studied. We, therefore, tested the prevalence and distribution of symptoms of AMS in children and adolescents of both genders in comparison to their parents upon fast ascent to an altitude of 3450—3650 m over the first 2 days of exposure. We further tested the relation between the individual perception of pain, SO2, and AMS.
Methods
Design
The study was performed in the summers of 2005, 2007, and 2009. Participants were investigated before and after ascent to HA. Baseline tests were performed at LA (450 m, barometric pressure 718 mmHg) within 4 weeks prior to ascent or 2 months after ascent. The families reached altitude by train in approximately 3 hours. The tests were repeated 8–10 h after arrival on day 1 (HA1), and 20–24 h after arrival in the morning of day 2 (HA2) after an overnight stay at the research station at 3450 m (2005 and 2007) or a nearby located mountain hut at 3650 m (2009), which was reached after a 45 min walk (Fig. 1). The experimental protocol was approved by the ethics committees of the ETH Zürich and the University of Basel. All participants or their legal representatives provided oral and written informed consent.

High altitude research station of Jungfraujoch (3450 m) and hut of Mönchsjoch (3650 m), Switzerland.
Study participants
A total of 87 prepubertal children (34 girls; Tanner stage 1), 70 adolescents (33 girls; Tanner stage >1), and at least one biological parent (88 fathers and 67 mothers) were recruited through announcements in the Swiss Alpine Club journal (total N=312). Exclusion criteria were symptoms and signs of cardiovascular or pulmonary abnormalities, any sleeping problems, previous history of perinatal pathology, and those with a recent (within 2 months) history of respiratory infections. Subjects were not allowed to stay at altitudes above 2000 m during 2 months prior to the study. The day prior and during all testing, subjects were not allowed to take any drugs other than acetaminophen. They abstained from substances such as alcohol or caffeine and they had a minimum of 8 h of night rest prior and during the study.
Measurements
Physical examination
An physical exam, including Tanner stage (for youth) and the cardiopulmonary system, was taken at LA and daily at HA. The clinical exam of AMS was done right before or after the completion of the questionnaires. It included the documentation of the mental state, of ataxia by the “heel-to-toe walking,” and of peripheral edema.
AMS questionnaires
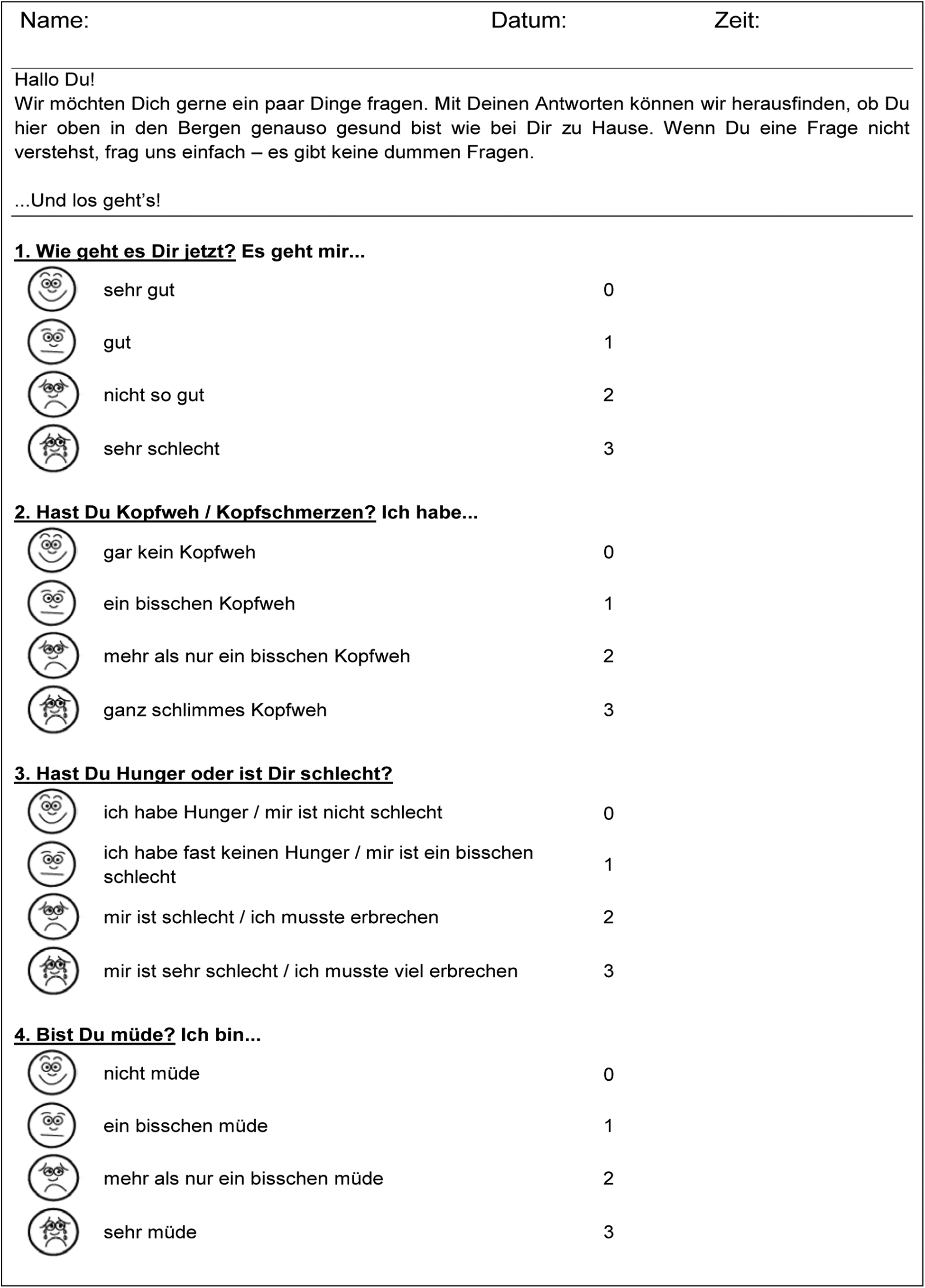
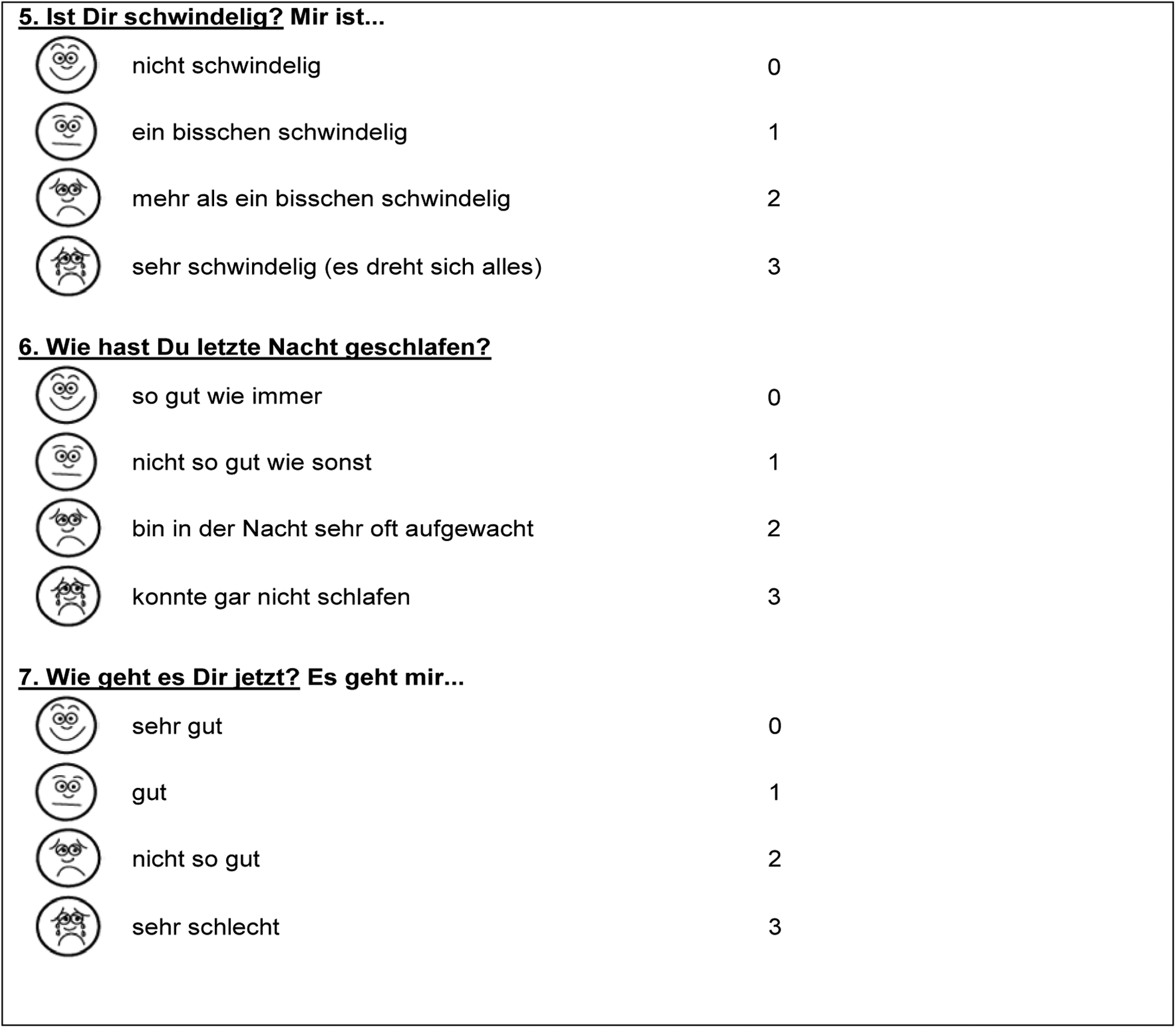
AMS was assessed by the adult version of the Lake Louise AMS Scoring system (LLS) (Roach et al., 1993) and a single question of the AMS-C score of the environmental symptoms questionnaire (ESQ) (Sampson et al., 1983). The latter question asked: “Do you feel sick”? on a 6-point Likert scale. The LLS is composed of five items that are graded from 0 (not present) to 3 (severe), including headache, gastrointestinal symptoms (nausea, vomiting, loss of appetite), dizziness, fatigue, sleep disturbance, and three clinical items including mental state, ataxia, and peripheral edema with a total score ranging from 0 to 23. Sleep disturbance between HA1 and HA2 was taken for the score of HA1 and HA2, as it makes no sense to include sleep disturbances from low altitude. Only in children, the child version of the LLS (CLLS), a modified questionnaire for children based on the LLS for adults and a published child version of the LLS, was used in addition (see Appendix 1) (Southard et al., 2007). An LLS-Score of ≥5 was defined as diagnostic for AMS (Roach et al. 1993). Children, adolescents, and adults answered the questionnaire independently of each other. An investigator was always present and answered all questions by the subjects in a neutral way. The intake of painkillers to treat headaches was whenever possible postponed until the questionnaires were filled out.
The cold pressure task (CPT) is a method to assess pain tolerance in humans (von Baeyer et al., 2005). It includes the assessment of the time until the person has to withdraw the hand after putting the non-dominant hand in water of 5°C because of pain or discomfort (maximum duration 240 sec) (von Baeyer et al., 2005). The CPT is widely used, also in children (von Baeyer et al., 2005), and is free of interference factors such as nausea, fatigue, fear of pain-inducing therapies, and does not cause negative effects (von Baeyer et al., 2005). Initially, the hands were washed with warm soap water. Thereafter, the non-dominant hand was put in water of 36°C for 5 min to standardize initial temperature of the extremity. The hand was then taken out of the water, dried with a towel, and put into ice water of 5°C up to a marked position 5 cm proximally of the wrist. The water was softly stirred by an investigator to prevent the water surrounding the hand from warming up.
The arterial oxygen saturation (SO2) was measured twice noninvasively by pulse oximetry (OxiMax N-595, Nellcor, Leuag AG, Stans, Switzerland) from the index finger; once when going to bed after a 10 min rest period and again before getting out of bed in the next morning. Values were noted at the end of each minute of assessment and the average of the last 5 min was taken for analyses.
Statistics
Numerical data are described by mean and SD when normally distributed or by median and interquartile range otherwise. Differences among AMS scores between the three study arms and by gender were initially assessed using regression analyses. We used mixed linear models with total AMS scores at HA1 and HA2, respectively, as dependent variables, generation, and gender as fixed factors, and the family (cluster) as random effect. We also tested whether the intake of painkillers did change results. Corresponding analyses for binary endpoints including analyses of concordance of AMS prevalence within families in families with both parents taking part in the study were performed using mixed logistic regression models. In secondary analyses, potential interactions between generation and gender were tested. Mixed linear models were also used to assess differences in scores across time or between instruments (LLS and CLLS), with a special focus on potential heterogeneity across generations. To assess corresponding differences in binary outcomes, we used linear regression with adjustment of standard errors for clustering of data within families (PROC GENMOD of SAS). In case of significant generation effects, analyses were stratified between children, adolescents, and adults. In addition, we tested agreement between a single criterion question of the ESQ questionnaire (a value of equal 1 was given if there was at least a slight feeling of sickness) and the LLS questionnaires by percentage of agreement (A) and Cohen's kappa (K) with 95% confidence intervals. Attractiveness of the different questionnaires was assessed by asking the children which of the questionnaires they preferred. Statistical analyses were performed with the use of the commercially available statistical package Stata 10. A p value of <0.05 was considered significant.
Results
Baseline characteristics are shown in Table 1. As there were no significant differences in AMS scores among the three study periods or between genders (data not shown), data were pooled. Significantly more adults documented having had symptoms of AMS in the past, but data on children were based on a limited past period. Thirty percent of all participants, irrespective of generation, had one or more AMS symptoms at LA, mostly fatigue and/or headache. One adult fulfilled the criteria for AMS at LA due to a migraine attack.
Score values are expressed as mean (±SD) or median (IQR). Differences among generations:*p<0.05, ***p<0.001 compared to adults
AMS, acute mountain sickness.
Scores and prevalence of AMS by age group are given in Table 2 and 3, as well as in Figure 2. Two mothers, one with an attack of severe migraine one h after arrival at HA, and the other with severe dizziness and a panic-like feeling of being sick, left soon after arrival. One prepubertal girl and one adolescent boy had to be treated with dexamethasone 4 and 6 h after arrival due to severe AMS (both) and pulmonary artery hypertension (girl) (Kriemler et al. 2006), respectively, and had to be withdrawn from the study for day 2. Their data were included for day 1, since the exams were taken prior to treatment.
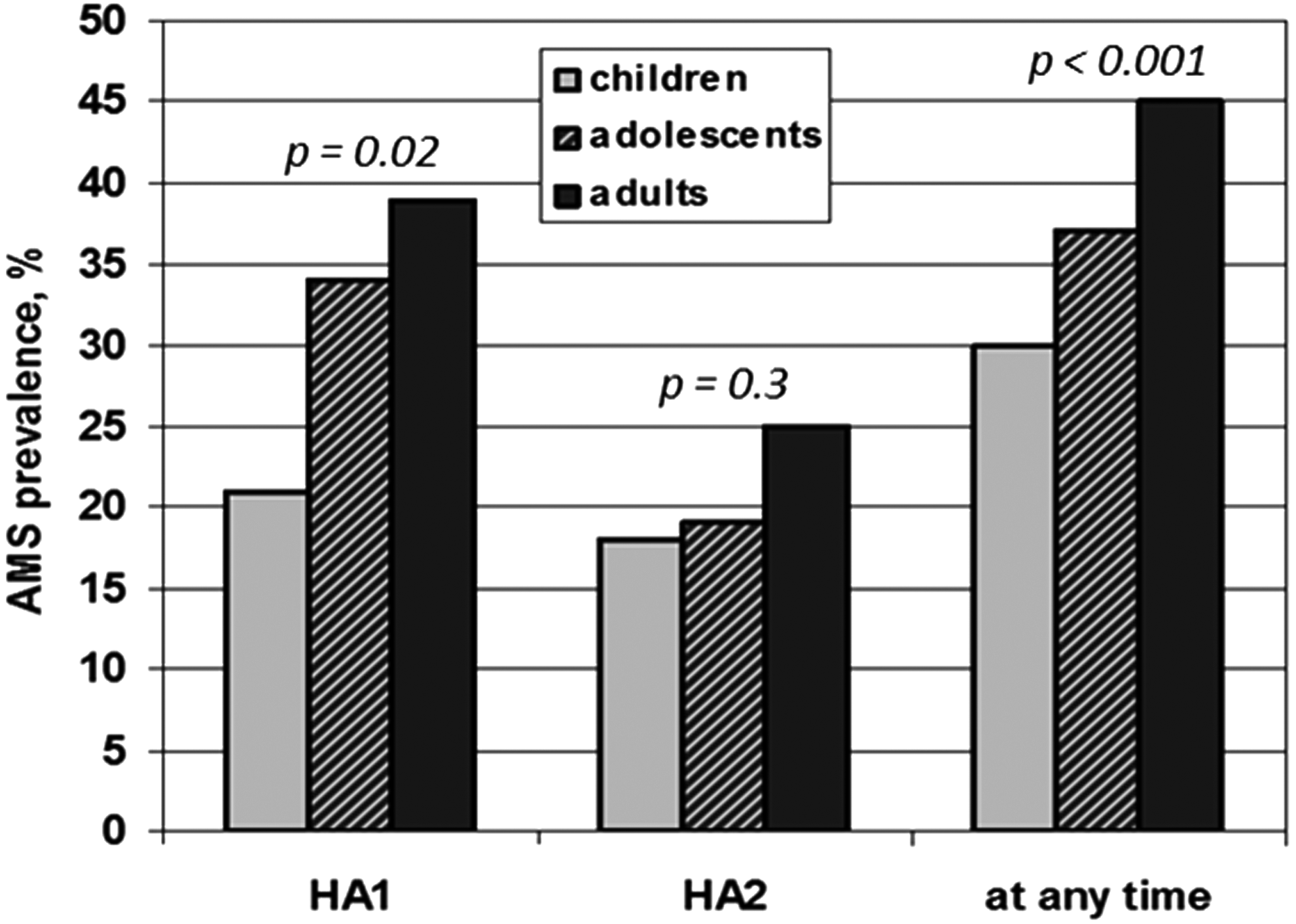
Prevalence of AMS by Lake Louise score and day 1 (HA1) and day 2 (HA2) and cumulative of high altitude at 3500 m in children (n=87), adolescents (n=70), and adults (n=155).
Score values are expressed as median and interquartile range (IQR) of AMS scores (assessed by LLS).
different from adults, †different from HA1.
HA1, day 1 at high altitude 8–10 hours after arrival; HA2, day 2 at high altitude 20–24 hours after arrival; LLS, Lake Louise Score.
Values denote prevalences by numbers (percentage) of subjects with AMS or with the feeling of being sick.
different from adults, †different from HA1 (p<0.05)¶ different between prevalence of being at least slightly sick and the LLS questionnaire, p<0.05.
HA1, day 1 at high altitude 8–10 hours after arrival; HA2, day 2 at high altitude 20–24 hours after arrival; LLS, Lake Louise Score; feeling at least slightly sick=single question from the ESQ questionnaire asking: “Do you feel sick?” Positive answers given by a 6 point Likert scale (from not at all=0 to strongly=6 with feeling at least slightly sick (Likert scale≥2).
Cumulative prevalence of AMS assessed by the LLS questionnaire was significantly lower in children (30%) as compared to adolescents (37%) and adults (45%), respectively (p<0.001). This was mainly due to lower AMS scores and prevalence in children compared to adults at HA1, but not HA2, while there was no difference between adolescents and adults (Table 2). There was a significant decrease in scores and prevalence over time in adolescents and adults, whereas in children, they remained unchanged between day 1 and 2. Seven (8%) children, nine (13%) adolescents, and 19 (12%) adults had severe AMS with LLS scores above 6 on HA1 or HA2 (p=ns). Omiting the symptom sleep from the LLS reduced prevalence significantly in adolescents and adults but not in children. Prevalence of “being at least slightly sick” corresponded reasonably well to a LLS-cutoff ≥5 (for children: A=75%, K=0.5 [0.3–0.7]; for adolescents: A=80%, K=0.6 [0.4–0.8]; for adults: A=73%, K=0.5 [0.4–0.6], respectively). AMS scores, prevalence, and symptoms of the LLS and CLLS in children were not different (see Appendix 1). The inclusion of the intake of painkillers as covariate into the model did not change results.
The prevalence of headache was lower in children compared to the older groups on HA1, and lower in children and adolescents compared to adults on HA2 (Table 4). Moreover, sleep disturbances in children and adolescents were significantly less prevalent than in adults. The other AMS symptoms did not differ significantly between the groups. All symptoms decreased over time; this was mostly significant only for adolescents and adults. Ninety-five percent of children liked the CLLS more than the LLS.
Values are expressed as numbers (percentage) of subjects with a specific symptom by the LLS questionnaire.
different from adults, †different from HA1, significance level p<0.05.
HA1, 8–10 hours after arrival; HA2, 20–24 hours after arrival, sleep disturbance refers to the night between HA1 and HA2; LLS, Lake Louise Score.
Figure 3 shows the concordance of AMS measured by the cumulative LL-Score between youth and adults. OR were 5.1 (95% CI 1.1 to 23.2, p=0.037) for children and adolescents to have AMS with both parents compared to none of the parents with AMS. If only one parent was affected, there was no higher risk of AMS (OR 1.5 (0.5 to 5.1)). Overall, familial clustering of AMS was consistent and accounted for 25%–50% of total outcome variance, and was 27% for the cumulated AMS prevalence by the LL-Score.

Significant concordance of AMS within 123 families. Bars denote the population of youth (58 children and 65 adolescents) and the correspondeing parents-pairs (34 single parent families excluded) categorized into AMS +/+ (both parents affected), AMS +/− (one parent affected), and AMS −/− (both parents healthy). Odds Ratio (OR) was calculated taking family clustering into account.
Results of the CPT are shown in Table 5. At LA, time in cold water was significantly shorter in children and longer in adolescents than in adults. At HA, it was shorter in children than in adults. Time in cold water at LA was significantly lower in those who developed AMS at HA than in the group that did not develop AMS. This difference was larger and statistically significant in children and adolescents. Time in cold water at HA1 was significantly lower in adults with than without AMS, while there was no difference for the younger groups. SO2 differed neither among groups or days nor among those with and without AMS.
Score values are expressed as median and interquartile range (IQR); Of note: CPT was not performed in the first, but only in the second and third study period.
different from adults, †different from no AMS, ‡different from low altitude, significance level p<0.05.
Discussion
This is the first report of a study that prospectively investigated severity, pattern, and prevalence of AMS in families comprising prepubertal children, adolescents, and adults upon acute exposure to 3500 m. Children were less affected by AMS on the first day of altitude exposure, whereas similarly low scores were observed in all groups on the second day of the altitude sojourn. The overall picture of the symptom distribution was similar in all groups. Differences in prevalence rates among generations were explained by less sleep disturbances in children that might be explained by the finding that children had less periodic breathing and therefore less arousal during the night than adults (Kohler et al., 2008). Children and adolescents from AMS affected parents showed OR of 3.4 to 6.5 to be affected as well compared to those from AMS-free parents. Overall, familial clustering explained 25%–50% of variability in AMS. Pain sensitivity increased at HA, but interestingly, it was significantly higher in those developing AMS compared to those that remained free of AMS. Differences in SO2 between those with and without AMS did not exist.
Strengths and limitations of study
We investigated AMS prevalence in prepubertal children, adolescents, and adults under standardized conditions at an altitude that is often reached in professional and recreational life. The results reassure that children tolerate high altitude at least as well as adults. Even prepubertal children from an age of 9 years on could easily report symptoms of AMS by a simple questionnaire, such as the LLS score. Moreover, the layout of the study enabled us to look at familial clustering of AMS which indeed occurred. Limitations of the study include the three different time periods used to run the study including a slightly different altitude (+200 m) and a different place of overnight stay. Yet, this is real life and none of the outcomes differed. Moreover, an altitude difference of 200 m is related to an ambient pressure difference comparable to the variability by weather conditions. It needs to be noted that we did not investigate younger children (<9 years). The history of AMS among generations cannot be taken as reliable source of information as children have a very limited past compared to adults. Due to parallel measurements of ventilatory parameters in some of the participants (not reported here), we asked all subjects to abstain from caffeine intake that may have biased the study results due to the potential occurrence of withdrawal headaches(Juliano and Griffiths, 2004). And finally, analyses of familial clustering of AMS were only done in families in which both parents took part, potentially limiting generalizability of findings.
Comparison with other studies
Although similar prevalence and severity of AMS in children of different age in comparison to adults has been suggested (Pollard et al., 2001; Kohler et al., 2008; Bloch et al., 2009), it has never been proven in sufficiently large, standardized trials. The prevalence of AMS in our study was comparable to other studies in adults (Maggiorini et al., 1990; Hackett and Roach, 2001) and adolescents (Bloch et al., 2009), although some higher or lower rates have also been reported (Hackett and Roach, 2001). Since different ascent speed, latitudes, and different diagnostic criteria were used, this is neither surprising nor contradictory (Schneider et al., 2002), but still might represent differences in individual susceptibility in different populations. Previous studies included much smaller numbers of children (Moraga et al., 2002; Moraga et al., 2008; Bloch et al., 2009; Pradhan et al., 2009) compromising generalizability. As previously shown, there was no significant difference in AMS prevalence between females and males (Hackett et al., 1976; Maggiorini et al., 1990). Only a tenth of the population had severe AMS with LLS scores above 6 at HA1 or HA2, and nobody developed high altitude pulmonary or cerebral edema.
There is no best way to document AMS as it is a subjectively assessed symptom complex combined with some clinical signs. Most scientists nowadays use the LLS, which is simple to use and translated into many languages. As shown in this study, the questionnaire can also be used for children from school age on. The value of including sleep disturbances is open for debate as assessment of sleep disturbances to determine AMS the first day of altitude exposure cannot be done, and there may not be an “ill-value” in an environment of reduced sleep comfort in huts and dormitories. This may be the reason why concordance of “being at least slightly sick” was higher when the symptom sleep was omitted from AMS scores (see Table 3). Yet, there was still a significant difference in adults (not in children and adolescents) between AMS prevalence and the “ill-feeling question” which is not easily explained. A possible explanation may be that many altitude-experienced adults don't perceive symptoms of AMS as a state of sickness, but rather take it as normal adaptation to high altitude and know that symptoms usually cease within little time.
Several studies have found specific genes that may, beside an environmental component, help to explain high altitude disease (MacInnis et al., 2010), but few have looked at epidemiological patterns or familial clustering that would be consistent with genetically influenced conditions (Yaron, 2001). This is the first study clearly documenting clustering of AMS within families with a high concordance between children and parents in AMS prevalence as classical marker of a genetically influenced trait. OR were 5-fold in children and adolescents to get AMS with both parents compared to no parents affected. Further studies with more participants may reveal whether there exist genes associated with biological pathways of AMS, or whether these findings are rather or also explained by intra-familial behavioral patterns, as shown in other domains (Christakis and Fowler, 2007).
Pain sensitivity to cold increased from normoxia to hypoxia and was higher in those with AMS. There is one study that tested pain thresholds and discrimination performances of electrical stimuli to the skin at low altitude and 6 days later at 3500m in adult lowlanders (Noel-Jorand et al., 1996). They found increased sensory discrimination and reduced thresholds to detect pain at comparable altitudes in a subacute hypoxic setting. They also measured psychological attitude towards imagined painful situations which did not change at high altitude, suggesting that increased sensory discrimination of pain is an adaption to hypoxia. These findings are in accordance to our findings of lower pain tolerances upon acute exposure to HA which hypothetically may facilitate ventilatory acclimatization due to an earlier onset of respiratory and other sensory perceptions (Noel-Jorand, 1996). Although pain sensitivity was higher in those with AMS at LA, it did not discriminate sufficiently to be used as screening test. Yet, it may partly explain the occurrence and severity of pain related symptoms such as headache.
Despite the fact that oxygen saturation is an easy measurable, noninvasive test often being recommended for diagnostic reasons, as it correlated with AMS (Roach et al., 1998; Burtscher et al., 2004), it was not a predictor of AMS in our study. Overall, SO2 values did not differ between groups with or without AMS. This is in agreement with some (Chen et al., 2012; Wagner et al., 2012), but not all studies (Karinen et al., 2010, 2012). Moreover, oxygen saturation may be difficult to measure in a standardized way depending on the conditions in the field. Also, multiple other factors affect the oxygen-dissociation curve such as age, hemoglobin concentration, plasma volume shifts, or cold in mountaineers exposed to HA. Therefore, measures of SO2 at HA have to be interpreted with sufficient caution.
Implications of study
AMS affected about one in five children during the first 2 days of altitude exposure to 3500 m that can easily be measured by the adults' or children's version of the LLS. AMS scores were in all generations mild to at most moderate and no serious problems were seen. Only on rare occasions (1%–2% in our sample), more severe AMS in children and adolescents may occur (Pollard et al., 2001; Kriemler et al., 2006), requesting medical treatment and/or immediate descent. These events were not life-threatening and disappeared quickly after treatment or descent. Thus, there are no reasons to discourage families with children aged 9 years or older to travel to high altitude. There are no studies about effects of treatment modalities in children with AMS, but body mass adapted evidence-based medications for adults seem to work similarly for all generations (Pollard et al., 2001).
Unanswered questions and future research
AMS prevalence and severity in children below the age of 9 years has not yet been sufficiently studied. We did not find any evidence that AMS prevalence and severity may increase with lower age, but appropriate family-based studies including measures focusing on heritability of high altitude illness are required to address this question. Even in adults, mechanisms of AMS secondary to (hypobaric) hypoxia are not well understood and should be studied in more detail. Postulated physiological responses potentially involved in AMS such as hypoventilation, impaired gas exchange, increased sympathetic drive, or alterations in fluid homeostasis should be specifically addressed in future research, including both adults and children. Likewise, emergency medications that may be applied in case of severe AMS including potentially harmful steroids should be tested in clinical trials, but due to increasingly precautious ethical committees, particularly in children, this might never happen.
Footnotes
Acknowledgments
We thank all participants and especially the children for their valuable contribution to the study. We also thank all team members of the High Altitude Research Station Jungfraujoch for their competent and extraordinary support. The study was supported by the Federal Council of Sports, Magglingen, Switzerland. They had no role in the design and conduct of the study, collection, management, analysis, and interpretation of the data.
Author Disclosure Statement
All authors declare to have no conflicting interests. All authors had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. There was no industry sponsoring.
Appendix 1
|
|