
Abstract
Abstract
Xiaodan Yan. Cognitive impairments at high altitudes and adaptation. High Alt Med Biol. 15:141–145, 2014.—High altitude hypoxia has been shown to have significant impact on cognitive performance. This article reviews the aspects in which, and the conditions under which, decreased cognitive performance has been observed at high altitudes. Neural changes related to high altitude hypoxia are also reviewed with respect to their possible contributions to cognitive impairments. In addition, potential adaptation mechanisms are reviewed among indigenous high altitude residents and long-term immigrant residents, with discussions about methodological concerns related to these studies.
Introduction
T
Cognitive Impairments at High Altitudes
The amount of cognitive impairments at high altitudes is related to the chronicity of exposure. Acute exposure usually refers to a duration of several weeks, whereas chronic exposure usually refer to “extended permanence” in the high altitude environment (Virués-Ortega and others, 2004). The altitude of ascending or residence is another factor affecting the severity of impairments. This review will first summarize the cognitive impairments in acute exposure, then talk about impairments in chronic exposure, with discussions about the effect of altitudes in corresponding sections.
Cognitive impairments associated with acute exposure
Impaired cognitive performance is certainly notable during acute exposure to high altitudes. In existing research, cognitive performances have been evaluated with psychological experiments utilizing various tasks such as digit span, number/letter sequence recognition, n-back working memory tasks, pattern completion tasks, card sorting tasks, word generation tasks, and word association tasks (Cahoon, 1972; Hornbein and others, 1989; Pavlicek and others, 2005; Zhang and others, 2011; Aquino Lemos and others, 2012); variations of these tasks allow researchers to isolate specific cognitive processes and investigate their changes after high altitude ascending. There is a large number of cognitive processes of interest, such as simple reaction time vs. complex reaction time, verbal fluency, cognitive flexibility, emotion regulation, verbal and spatial working memory, as well as decision making. To investigate cognitive changes associated with high altitude ascending, studies have been conducted on subjects exposed to high altitude hypoxia either via laboratory simulated hypobaric chambers or after naturalistic expenditure to high altitude regions (Nelson, 1982; Fowler and others, 1987; Kramer and others, 1993). Impairments have been documented across a wide range of cognitive systems including short-term memory, verbal fluency, language production, cognitive fluency, and metamemory, although in general complex cognitive processes are more susceptible to high altitude related impairments (Table 1) (Virués-Ortega and others, 2004). Psychological testing at high altitudes frequently reports longer reaction time; it has also been documented that subjects tend to sacrifice reaction time to maintain accuracy when performing cognitive tasks under conditions of hypoxia (Cahoon, 1972).
The severity of impairments is related to the extent of high altitude ascending. Studies have shown that with higher altitudes come more serious impacts. At medium altitudes up to 2000–3000 meters, minimal impairments have been reported (Pavlicek and others, 2005; Zhang and others, 2011), at 3000–4000 meters visible psychomotor impairments have been shown (Wilson and others, 2009), while at extremely high altitudes above 6000 meters, somesthetic and visual illusions have been documented (Virués-Ortega and others, 2004) (Fig. 1).
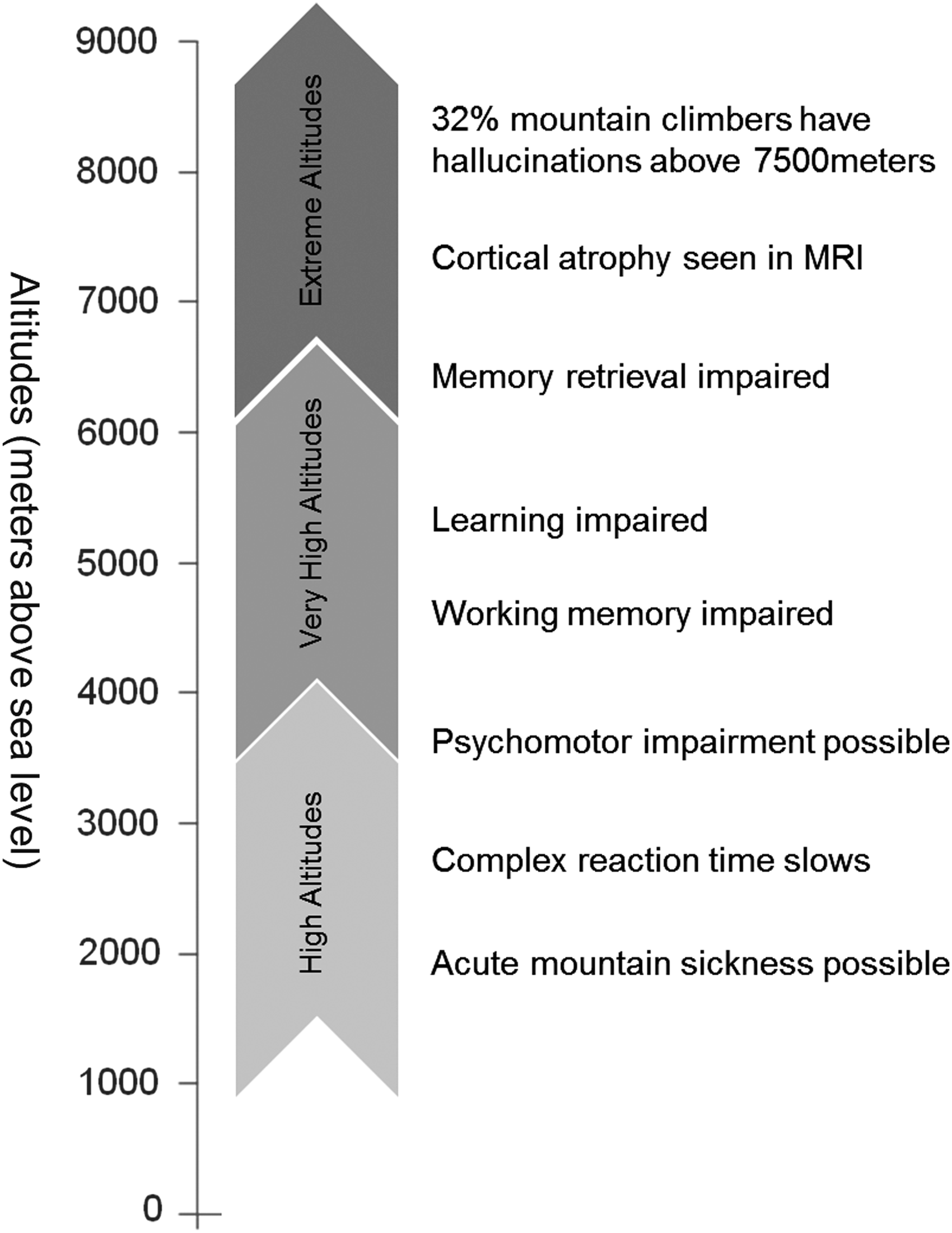
High altitude-related neurocognitive impairments with ascending attitudes in acute high altitude exposure (Wilson and others, 2009).
Cognitive impairments associated with chronic exposure
Compared to the amount of studies about cognitive impairments after acute high altitude exposure, there are fewer studies about the cognitive impairments associated with prolonged chronic exposure to high altitude hypoxia. Cognitive impairments have been observed among long-term high altitude residents. A series of recent studies systematically investigated infants, children, and adolescents who lived in Bolivia (∼500 m, ∼2500 m, and ∼3700 m),and revealed that these participants had reduced motor speed, cognitive processing speed, and cerebral blood flow velocity as a function of residence altitudes (Hogan and others, 2010).
Another series of studies looked at young adults who were third- or fourth-generation decendents of immigrants to high altitudes. The study participants were born and raised at altitudes of about 2600–4200 meters until early adulthood, and they were compared with a control group of the same ethnic group and well-matched on age, gender, education levels, and socioeconomic status, except that the control group were born and raised at low altitude regions (below 400 meters). Both groups were living at the same low altitude region within the past year at the time of study. These studies revealed that the original high altitude residents showed reduced performance accuracy in a verbal working memory task and longer reaction times in verbal and spatial working memory tasks (Yan and others, 2011a; 2011b). Compared to exposure to high altitudes since early childhood, another study showed that a comparatively short period of residence (about 7 months) at moderate altitudes (2260 meters) of those who were originally from low altitudes did not seem to induce significant cognitive impairments (Zhang and others, 2011).
There are some methodological concerns pertaining studies about cognitive impairments associated with prolonged chronic high altitude exposure. Some studies compared indigenous high altitude residents with indigenous low altitude residents; in this case, when inferring about neuropsychological/cognitive differences, the cultural differences between the two populations have to be considered (Lu and others, 2001; Virués-Ortega and others, 2006). For example, it has been reported that neurodevelopment of Quechua infants may be delayed due to the traditional garment used to protect infants, which significantly limits the stimulation opportunities of the child (Tronick and others, 1994). Another study showed that the mathematical abilities of Tibetan (indigenous high altitude residents) secondary school students are lower than age-matched Han (indigenous low altitude residents) students, and multifactor analyses showed that this could be related to differences in intelligence development profile and various non-intelligence factors such as stability, inquisitiveness, self-discipline, and individuality (Lu and others, 2001), many of which could have been culturally shaped behavioral patterns. Studies comparing local residents of different regions should consider cultural differences as well as potential disparity in the socioeconomic developments of these regions, all of which could have significant impacts on the neurocognitive developments of the local residents.
Neural Changes Related to High Altitudes
Oxygen is critical for neuronal functioning and growth in the brain. Although the human brain takes up only about 2% of the body weight, it consumes about 20% of the oxygen intake (Clark and Sokoloff, 1999; Raichle, 2010; Raichle and Gusnard, 2002) (Fig. 2). The amount of oxygen in the air decreases with increasing altitudes. The hypoxic condition at high altitude regions poses significant challenge to the functioning and growth of neurons in the brain (Leblond and Krnjevic, 1989). These neuronal impairments may be underlying the cognitive impairments observed at the behavioral level.

The human brain consumes about 20% of the total oxygen intake, which is disproportional to its size (about 2% of the total body weight). In this figure, oxygen consumption is reflected from glucose consumption in positron emission tomography (PET) (Alavi and Reivich, 2002).
Some neuronal impacts are reversible; however, studies have shown that some hypoxia-related neuronal changes may not be restored even with enriched oxygen supply. For example, in laboratory experiments on rodents, it has been shown that the reduced hippocampal capillary density induced by hypoxia was reversible with reoxygenation, but decreased myelination in corpus callosum was irreversible (Kanaan and others, 2006). An MRI study on humans showed that mountain climbers with repeated expenditure, compared to subjects with no lifetime history of high altitude exposure, had reduced white matter density in the primary (BA 4) and supplementary (BA 6) motor cortex (Paola and others, 2008). Another study revealed decreased gray matter density at bilateral prefrontal cortex and bilateral insula among subjects who were born and grew up at high altitude regions until early adulthood, even after their living at low altitude regions for more than 1 year (Yan and others, 2010). It is possible that some of the irreversible neuronal impacts directly or indirectly undermine the long lasting cognitive impairments that were observable even after individuals return to sea level regions after their high altitude ascending (Virués-Ortega and others, 2004; Rostrup and others, 2005). Therefore, although oxygen enrichment was suggested to be an effective way for improving mental performance and well-being at high altitudes (West 1999; 2002), due to the possible irreversible neuronal impairments, it may have limited capability in reversing all cognitive impairments caused by exposure to high altitude hypoxia.
Physiological Factors Related to Cognitive Impairments
Besides neural impairments, other physiological factors may also have significant contributions to the cognitive impairments at high altitudes. For example, sleep disturbance is very common among individuals with high altitude exposure, with reduction in the later sleep phases, reduced rapid eye movement (REM) sleep, and increased night arousals (Buguet and others, 1994; Matsuzawa and others, 1994). One study revealed significant correlations between indicators of sleep quality and cognitive functions at high altitudes, such as a significant positive correlation between REM latency and working memory and a significant negative correlation between REM sleep and inhibitory control (Aquino Lemos and others, 2012). Other physiological symptoms, such as reduced appetite, fatigue, and headache may also impose significant impacts on cognitive performances, but their specific relationships with cognitive impairments are complicated. A study showed that about 25% of those who recently ascended to an altitude of above 2000 meters developed acute mountain sickness (AMS), with symptoms including poor appetite, nausea, vomiting, weakness, lightheadedness, dizziness, and reduced sleep quality (Honigman and others, 1993; Montgomery and others, 1989). The effect of AMS on cognitive functions is controversial. Virués-Ortega et al. (2004) suggested that AMS is a “sufficient but not necessary condition for altitude neuropsychological impairment.” Some studies revealed that there was no significant correlation between scores of AMS and the extend of cognitive dysfunction (Abraini and others, 1998), and two studies revealed that those who developed AMS had different cognitive impairments compared to those who did not; results of these studies showed that subjects who developed AMS showed more impairment in conceptual tasks, whereas those who did not develop AMS showed more impairment in short term memory (Forster, 1985; Kramer and others, 1993). These studies have only evaluated the relationship between AMS and cognitive impairments, while the long-term effects of AMS on cognitive impairments still require further study.
Adaptation to High Altitudes
The possibility of adaptation to high altitude hypoxia has always been an intriguing issue. In the acute cases, the human body does have some capacity for acclimatization, which varies significantly for different individuals (Tissandier, 1875; Kramer and others, 1993). The question is, in chronic cases, for example, does growing up at high altitude regions guarantee sufficient adaption to occur to compensate for the risk of cognitive impairments? Existing research tends to suggest that, although some level of adaptation does occur, neural and cognitive impairments are still observed in these populations who are native or long-term residents at high altitude regions (Virués-Ortega and others, 2006; Niermeyer and others, 2009). One study suggested that Quechua natives, who are indigenous to the high Andes between about 3700 and 4900 meters altitude, had cerebral hypometabolism as a potential defense mechanism against chronic hypoxia (Hochachka and others, 1994). However, another study with the same experimental approach conducted on Sherpa, who are natives of the Himalayas, did not reveal reduced metabolic rates compared to low land natives (Hochachka and others, 1996). It was proposed that the two populations may have different routes of adaptation (Beall, 2007). Primary methodological concerns with these studies are the cultural, socioeconomic, and even potential genetic differences (Simonson and others, 2010; Yi and others, 2010; Peng and others, 2011) between the indigenous high altitude residents and low altitude residents, which complicates the interpretation and attribution of these findings.
Although multiple studies have suggested that growing up at high altitudes is associated with cognitive impairments, it is not to say that adaptation does not happen with prolonged chronic exposure to high altitudes. One study has revealed that as a function of the length of low altitude residence (across the range of 1–5 years), some neuroimaging parameters of original highlanders who grew up at high altitude regions had shown the trend of converging towards the patterns of original low altitude residents, although such changes were not accompanied by statistically significant changes in cognitive performance (Yan and others, 2010). It is possible that, given sufficiently long time for normoxia adaptation, the neural and cognitive impairments associated with high altitude hypoxia may be alleviated to a certain extent.
Conclusion
In summary, various cognitive impairments associated with high altitude hypoxia have been reported from existing studies, which are accompanied by findings about neural impairments, suggesting that these cognitive impairments have legitimate neural basis. The specific relationships between physiological symptoms and cognitive impairments appear to be complicated and require further elucidation. There are cognitive impairments associated with both acute and chronic exposure to high altitudes; however, particular caution should be taken when interpreting the findings about cognitive impairments among native high altitude residents because of the differences in cultural and socioeconomic factors. Existing studies have suggested that there can be some level of adaptation to high altitudes, in spite of the fact that some neuronal impairment may be irreversible.
Footnotes
Author Disclosure Statement
No competing financial interests exist.