
Abstract
Abstract
Mellor, Adrian, Christopher Boos, David Holdsworth, Joe Begley, David Hall, Andrew Lumley, Anne Burnett, Amanda Hawkins, John O'Hara, Stephen Ball, and David Woods. Cardiac biomarkers at high altitude. High Alt Med Biol 15:452–458, 2014.—
Methods:
48 participants were assessed post-trekking and at rest at three altitudes: 3833 m, 4450 m, and 5129 m. NPs, hs-cTnT and hsCRP, were quantified using immunoassays, PASP was measured by echocardiography, and AMS scores were recorded.
Results:
Significant changes occurred with ascent in NPs, hs-cTnT, hsCRP (all p<0.001) and PASP (p=0.006). A high PASP (≥40 mm Hg) was associated with higher NPs, NT-proBNP: 137±195 vs. 71.8±68 (p=0.001); BNP 15.3±18.1 vs. 8.7±6.6 (p=0.001). NPs were significantly higher in those with AMS or severe AMS vs. those without (severe AMS: NT-proBNP: 161.2±264 vs. 76.4±82.5 (p=0.008)). The NPs correlated with hsCRP. cTnT increased with exercise at HA and was also higher in those with a high PASP (13.8±21 vs. 7.8±6.5, p=0.018).
Conclusion:
The NPs and hs-cTnT are associated with high PASP at HA and the NPs with AMS.
Introduction
C
NP release may also be stimulated by hypoxia (Due-Andersen et al., 2008; Casals et al., 2009) and they have been found to be elevated in association with pulmonary artery hypertension (Nagaya et al., 2000; Blyth et al., 2007; Shiina et al., 2009) at sea-level (SL). High altitude pulmonary edema (HAPE) is a noncardiogenic form of pulmonary edema, a central feature of which is an exaggerated pulmonary vascular response with a marked rise in pulmonary artery systolic pressure (PASP) (Maggiorini et al., 1990; Bartsch et al., 2005). Around 4% of people at 4559 m (Maggiorini et al., 2001) suffer from HAPE, with around 53% suffering the syndrome of acute mountain sickness (AMS). Both conditions represent a significant diagnostic and therapeutic challenge at high altitude (HA). An association between the NPs and AMS has been reported at HA (Bartsch et al., 2005; Woods et al., 2011; Woods et al., 2012) and we have recently reported a relationship between abnormally high PASP and the NPs in a small cohort at HA (Woods et al., 2013).
Recent work has shown a rise in cardiac troponin with exercise in patients with pulmonary hypertension (Volkers et al., 2013), and although several studies have examined the troponin response to exercise at SL in healthy individuals (Shave et al., 2010), there is a paucity of data at HA. Marked inflammatory states can stimulate NT-proBNP secretion (Piechota et al., 2007; Wolff et al., 2007) and increases in inflammatory markers have previously been reported at HA (Hartmann et al., 2000; Bailey et al., 2004; Shintaro et al., 2006; Smith et al., 2011). In this study we therefore sought to expand on our previous findings in a much larger cohort and to investigate the cardiac biomarkers BNP, NT-proBNP, hs-cTnT, and hsCRP and their relationship with abnormally high PASP and AMS.
Methods
The study protocol was approved by the Ministry of Defence Research Ethics Committee (MODREC), UK, and conformed to the standards set in the Declaration of Helsinki. All subjects gave written informed consent.
Subjects
48 healthy participants from the UK Defence Medical Services expedition to the Cordillera Real region, Bolivia, were studied. 20 of these subjects were also studied at sea-level (SL) pre- and post-exercise (a 6-hour trek) 6 weeks before the expedition. Participants flew from UK to La Paz (altitude 3600 m). Subjects were studied at three altitudes post-trek and at rest: 3833 m, 4450 m, and 5129 m.
Ascent profile: Day 1: arrive La Paz, 3681 m; Day 2: 6-hour trek with 600 m altitude gain to sleep at 3833 m; day 3: rest at 3833 m, day 4: La Paz, 3681 m; day 5; road move then 4-hour trek with 200 m altitude gain to 4450 m; day 6: 4450 m rest; day 7: 4710 m, day 8: 4710 m; day 9: 5129 m (4-hour trek with 400 m altitude gain); day 10: 5129 m (rest). The majority of data acquisition was performed on “study days” immediately post-trek and at rest the following morning: on day 2/3833 m (after 6-hour trek, distance 16.8 km); day 5/4450 m (after easy trek, 5.61 km), and day 9/5129 m (after an intense 1.59 km trek).
Twice-daily physiological data (heart rate, blood pressure, oxygen saturation (Sp
BNP and NT-proBNP assay
Venous blood samples were taken from the antecubital fossa. Briefly, BNP was assayed from an EDTA-anticoagulated whole blood sample on-site using a Biosite Triage Meter and Triage BNP test kits (Alere, Cheshire, UK). The BNP range reported by the test system is 5–5000 pg mL−1. Coefficient of variation at a mean BNP is 9.2% and 45.6 pg/mL. NT-proBNP was analyzed on return to the UK using a serum sample that had been frozen at −20°C. The assay was performed using the Roche NT-proBNP assay (Roche Diagnostics, Mannheim, Germany) with a range from 5 to 35000 pg mL−1 and a coefficient of variation at a mean NT-proBNP of 474 pg mL−1 of 5.8%.
Troponin assay
On return to UK, a highly sensitive cardiac troponin T (hs-cTNT) assay was performed using an electro-chemiluminescence immunoassay (ECLIA) on a Cobas Analyser (Roche Diagnostics). This assay has a range from 3–10000 ng/L. The upper reference limit (99th percentile) for this assay in healthy volunteers is 14 ng/L (pg/mL). This assay has a range from 3 to 10,000 ng/L. The coefficient of variation at a mean hs-cTnT level of 13.5 ng/L is 5.2%, 8.5% at 5.3 ng/L, and 1.8% at 28.5 ng/L (all cTNT assays were performed in a single run) (Boos et al., 2014).
CRP assay
A commercially available, highly-sensitive, immunoturbidimetric assay (Roche Diagnostics) was used to measure CRP on samples taken at the same time-points as the NPs. This assay has a measuring range of 0.1–300 mg/L and a between run coefficient of variation between 2.5% and 5.7%.
AMS scores
AMS scores were assessed using the Lake Louise score (LLS) (Hackett and Oelz, 1992). The LLS is a self-assessment questionnaire that allocates a score of 0 to 3 (symptom not present to severe) for symptoms of AMS (headache, gastrointestinal symptoms, fatigue/weakness, dizzy/light-headedness, difficulty sleeping). A score of 3 or more in the presence of headache is consistent with AMS, a score of 6 or more with severe AMS.
Statistical analysis
For statistical calculations the software package SPSS 14.0 was used. Subjects were excluded who took drugs to aid acclimatization (n=3). Parametric or nonparametric statistical tests were applied after performing the Shapiro-Wilks statistic.
Changes in dependent variables between altitudes were initially tested by Student's paired t test or Wilcoxon signed ranks test. For independent variables, an independent-samples t test or Mann Whitney test was used. Either a within subjects ANOVA or a Friedman test was performed to investigate any serial changes in measures (e.g., PASP or BNP) with ascent. A correlation analysis between BNP and NT-proBNP was performed using Spearman's rank correlation.
As the maximal PASP response in healthy subjects to hypoxia is thought to be 40 mm Hg, and as non-HAPE susceptible individuals have a mean rise of PASP to 37±4 mmHg during exercise in hypoxia (Grunig et al., 2000), data were also analyzed according to a PASP cut-off of 40 mmHg. Logistic regression was used to assess the relationship between the NPs and the presence or absence of AMS/severe AMS and high PASP. A ROC (receiver operating characteristic) analysis was done to investigate the utility of the NPs in identifying AMS/severe AMS and a PASP>40 mmHg.
A p value<0.05 was considered significant throughout. All data presented as mean±sd (±range where appropriate).
Results
The subjects were 35.2±9.1 years old, 175.5±9.5 cm in height, and 77.5±13.9 kg in weight. 45 subjects reached the highest study altitude (5129 m).
LL scores
Repeated measure (RM) ANOVA revealed a significant change in LL score between altitudes (p<0.001). Over the six study time points at HA, 65 LL scores (24.4%) were consistent with AMS (LL score≥3) and 18 (6.8%) consistent with severe AMS (LL score≥6). The incidence of AMS and severe AMS at each altitude is reported in Table 1.
These values represent all observations (n=276), LLS data, NT-proBNP and BNP was available for 266 observations.
BNP and NT-proBNP
BNP and NT-proBNP values for each study point are detailed in Table 2. NT-proBNP and BNP significantly correlated (rho 0.763, p<0.001). NT-proBNP (p<0.001), but not BNP, rose modestly following exercise at near-SL in the UK. Repeated measures analysis demonstrated a significant change in BNP and NT-proBNP between altitudes (p<0.001 for both). Peak BNP and NT-proBNP levels were seen at 3833 m. There was no significant difference in BNP at rest or post-exercise between SL and 5129 m. NT-proBNP was significantly higher at rest at 5129 m vs. SL (p=0.008) but not following exercise.
Data presented as mean±sd, range.
hs-cTnT
Repeated measures analysis showed a significant change in cTnT at HA (Table 2). Peak values were seen after exercise at SL and after trekking at 5129 m. Subjects with a cTnT above the upper limit of normal (ULN, 14 ng/L): SL post-exercise: 6; SL rest: 0; 3833 m post-trek: 14; 3833 m rest: 4; 4450 m post-trek: 2; 4450 m rest: 2; 5129 m post-trek: 11; 5129 m rest: 7. cTnT was significantly higher in those with a PASP>40 mm Hg than those without: (cTnT: 13.8±21 vs 7.8±6.5, p=0.018). ROC analysis (to investigate the utility of cTnT in detecting a high PASP) revealed an AUC of 0.607 (95% CI 0.520–0.693, p=0.018) There was no difference between cTnT and presence of AMS or severe AMS.
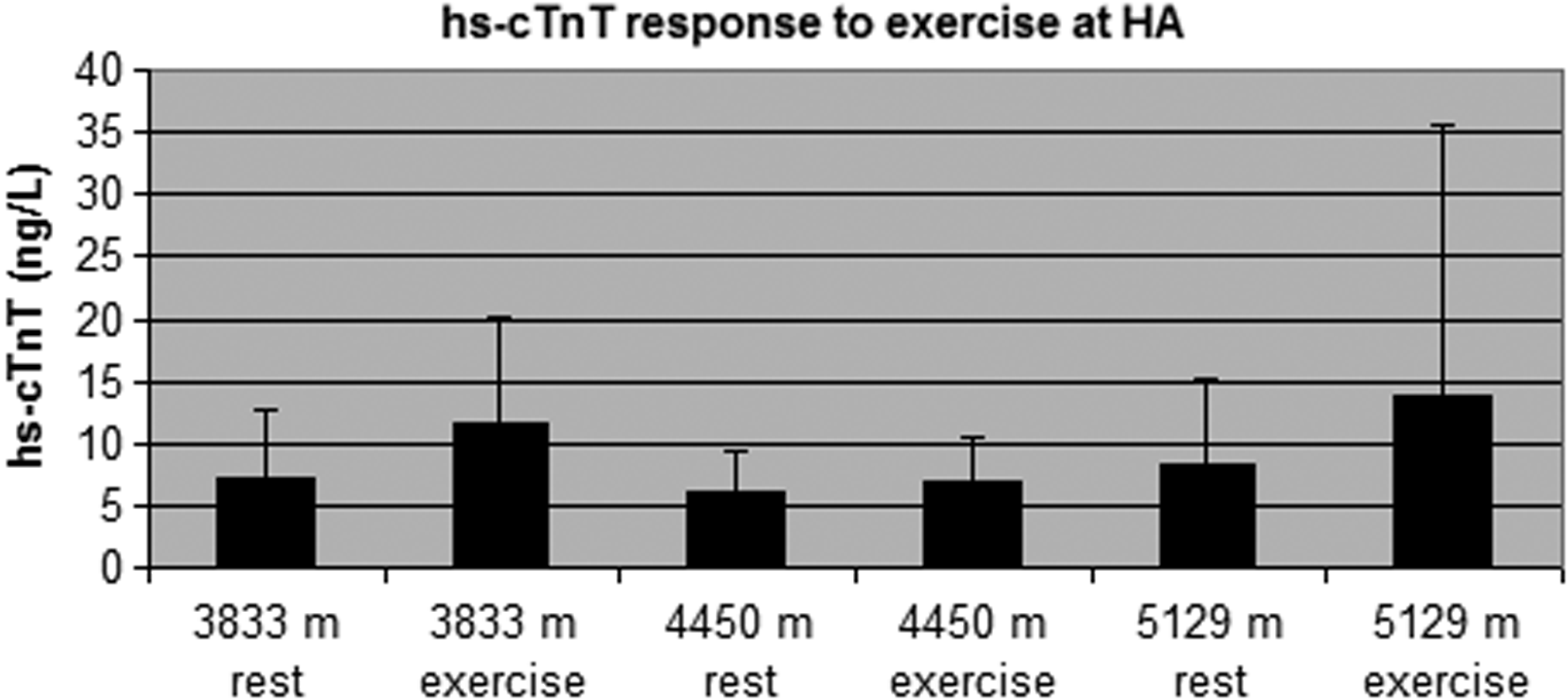
The hs-cTnT response to exercise at HA. hs-cTnT rose significantly with exercise at 3833 m and 5129 mm but not at 4450 m. There were 11 subjects with hs-cTnT above the upper limit of normal (14 ng/L) at 5129 m post-trek.
hsCRP
Repeated measures analysis showed a significant change in hsCRP at HA (p<0.001), see Table 2. Overall there was a weak correlation between hsCRP and NT-proBNP (rho=0.367, p<0.001) and BNP (rho=0.263, p<0.001). However, there was no difference in hsCRP according to presence or absence of AMS (6.3±19 vs. 5.6±12, respectively) or severe AMS (6.3±15 vs. 5.7±14, respectively).
PASP
RM ANOVA showed a significant rise in PASP between altitudes (p=0.006), data presented in Table 2. PASP correlated inversely with Sp
AMS scores and BNP/NT-proBNP
At altitude there were 266 simultaneous recordings of a LL score at HA with a simultaneous BNP and NT-proBNP. NT-proBNP and BNP were significantly higher on those occasions when LL score was consistent with AMS (n=65, 24.4%) vs. those without (NT-proBNP: 113±164 vs. 72±78, p=0.034; BNP 13.1±16 vs. 8.7±7, p=0.008). On those occasions when LL scores were consistent with severe AMS (n=18, 6.8%) NT-proBNP and BNP were also significantly higher than those without (NT-proBNP: 161.2±264 vs. 76.4±82.5, p=0.008; BNP 17.1±25 vs. 9.2±8, p=0.007).

NT-proBNP at HA according to PASP. NT-proBNP was significantly (p=0.001) higher in those with an abnormally high PASP at HA.
Logistic regression analysis showed that BNP (p=0.008 and p=0.017) and NT-proBNP (p=0.031 and 0.022) were statistically associated with the presence or absence of AMS or severe AMS, respectively.
ROC analysis (to investigate the utility of BNP and NT-proBNP in detecting AMS and severe AMS) revealed an AUC of 0.601 (95% CI 0.519–0.682, p=0.015) for BNP with an AUC of 0.588 (95% CI 0.506–0.67, p=0.034) for NT-proBNP in AMS. ROC analysis for the NPs in severe AMS revealed an AUC for BNP of 0.675 (95% CI 0.553–0.797, p=0.013) and for NT-proBNP an AUC of 0.686 (95%CI 0.56–0.813, p=0.008). An NT-proBNP of 80.5 had a sensitivity of 61% and a specificity of 69% for detecting severe AMS.
PASP and BNP/NT-proBNP
At altitude there were 245 echocardiographic assessments of PASP with simultaneous BNP or NT-proBNP values. Of these 52 (21%) had a PASP ≥40 mm Hg. NT-proBNP and BNP were significantly higher in those with a high PASP vs. those without (NT-proBNP: 137±195 vs. 71.8±68, p=0.001; BNP 15.3±18.1 vs. 8.7±6.6, p=0.001).
Logistic regression analysis showed that BNP (p=0.001) and NT-proBNP (p=0.003) were statistically associated with the presence or absence of high PASP.
ROC analysis (to investigate the utility of BNP and NT-proBNP in detecting a PASP ≥40 mm Hg) revealed an AUC of 0.645 (95% CI 0.557–0.732, p=0.001) for BNP with an AUC of 0.648 (95% CI 0.566–0.730, p=0.001) for NT-proBNP.
Peak BNP and NT-proBNP occurred at 3833 m at rest. At that point there were 6 subjects with a PASP ≥40 mm Hg. Their NT-proBNP and BNP were higher than those with a lower PASP (NT-proBNP: 370±413 vs. 101±72, p=0.003; BNP: 37.5±38 vs. 10±6.7, p=0.003).
Discussion
This significant cohort at HA demonstrates that NT-proBNP and BNP are higher in those with a high PASP, AMS, or severe AMS. cTnT was also found to be higher in those with a high PASP and exercise, even of short duration at HA, was a significant stimulus to cTnT release. The NPs were also are positively, though weakly, correlated with hsCRP.
Diagnosing HAPE in the field can be a significant clinical challenge and although a high PASP is a key feature of HAPE (Maggiorini et al., 1990; Bartsch et al., 2005) echocardiography is not typically available. A surrogate biochemical marker could therefore be extremely useful and facilitate both early detection and diagnosis. While it could be argued, and we would accept, that the diagnostic ability of the NPs in detecting a high PASP is not at present clinically robust, it must be noted that we have currently applied the test in all subjects, irrespective of symptoms, at HA. As such, the pre-test probability of detecting a markedly elevated PASP will naturally be low. The clinical utility of the NPs in detecting asymptomatic left ventricular systolic dysfunction in apparently healthy populations is also highly variable with BNP values between 45–50 pg/mL giving 95% specificity but very low sensitivity (13%–27%) (Vasan et al., 2002). The AUC for BNP in detecting mild systolic dysfunction is around 0.60 in women and 0.72 in men (Goetze et al., 2006), not dissimilar to what we have found for a high PASP. However, in the context of a breathless patient who presents to the emergency room, the pre-test probability of CCF is much higher and the ability of the NPs in detecting the condition are well proven with an AUC of between 0.804 and 0.883 (Boldanova et al., 2010). We have recently reported (Boos et al., 2013) the case of a research participant who presented on this expedition at 3883 m complaining of dyspnea and chest tightness. The clinical findings of hypoxia (Sp
Prolonged endurance exercise leads to increases in NT-proBNP (Hew-Butler et al., 2008; Scharhag et al., 2005; 2008). It has previously been reported (Toshner et al., 2008) that following arrival by vehicle at 5200 m (after 5 days acclimatization at 3600 m) no rise in NT-proBNP occurred despite a rise in PASP. This emphasizes the importance of prolonged exercise at HA in the release of NPs. It would seem likely that the peak NP levels seen at 3833 m reflect the fact that this was the longest (6 hours) trek of the expedition with the greatest ascent (600 m) and therefore arguably the greatest exercise stimulus.
We have also confirmed, in this much larger cohort, our previous finding that AMS, and in particular severe AMS, are associated with higher NPs. A novel finding was that at HA hsCRP is positively, though weakly, correlated with the NPs. While it is known that marked inflammatory states are a potent stimulus for NT-proBNP secretion (Piechota et al., 2007; Wolff et al., 2007), this is the first report of any association at HA. hsCRP has previously been reported to increase at HA (Hartmann et al., 2000; Bailey et al., 2004; Shintaro et al., 2006; Smith et al., 2011) and although one report has suggested hsCRP may be associated with AMS (Shintaro et al., 2006), we found no evidence to support this.
It has previously been reported that at SL exercise stimulates hs-cTnT release (Shave et al., 2010; Legaz-Arrese et al., 2011; Duttaroy et al., 2012; Eijsvogels et al., 2012). We also found an exercise-induced rise at SL, 3833 m, and 5129 m. We did not see a rise in hs-cTnT at 4450 m, but the exercise stimulus was perceived to be mild. Although the trek to 5129 m was shorter than that to 4450 m, it was of a greater intensity and physically more strenuous. It would seem that exercise intensity, whether over long (30–50 km walking) (Eijsvogels et al., 2012), or short duration, (high intensity over 30–60 min) (Shave et al. 2010; Duttaroy et al. 2012) is key to the stimulation of cTNT release. We also found significantly higher cTnT in those with a high PASP. Similar to the relation between NPs and PASP, further work is needed in symptomatic subjects at HA to evaluate the use of cTnT in identifying those with an abnormally high PASP. Whether the cTnT release we have seen is secondary to increased membrane permeability or true myocardial necrosis remains to be elucidated. Although several participants demonstrated a rise in cTnT into the range that, in an alternative context, may be associated with a myocardial infarction (Thygesen et al., 2012), we did not observe clinical or echocardiographic features that suggested significant myocardial ischemia.
There are some limitations of this study worthy of consideration. While we have managed to study a reasonable size cohort at a significant altitude, we acknowledge that this is still a small cohort for the investigation of biomarkers and as such may be underpowered to detect certain differences. In addition, we also acknowledge that we were not directly investigating these biomarkers in the diagnosis of HAPE but in relation to PASP using echocardiography. While right heart catheterization is the most robust method for assessing PASP and would have been preferable, this would not be possible or practical for a remote field study like this. Nevertheless, allowing for its known limitations such as the need for good acoustic windows and an adequate tricuspid regurgitation jet, echocardiography remains the noninvasive gold standard method for PASP quantification and has been well validated against right heart catheterization (Yock and Popp, 1984). We also acknowledge that the biomarkers measured in this study have significant variability and that NPs, in particular, may be affected by age, sex, and renal function. However, this variation is small in healthy individuals aged <65 years without known renal dysfunction as were included into this study and is supported by the very low baseline NP levels (Clerico et al., 2002; McCullough and Sandberg, 2003). We would also accept that the performance of the Triage BNP assay is not as good as a laboratory-based assay but does offer the advantage of giving a point-of-care result.
In summary, we have demonstrated an association of BNP and NT-proBNP with AMS, severe AMS, and a high PASP at HA. In addition we report an exercise-associated rise in cTnT at HA and a higher cTnT in those with high PASP. Further, we confirm a rise in hsCRP with HA and suggest some association between hsCRP and the NPs. The challenge for future studies evaluating biomarkers at HA is to further delineate the pathological from the physiological by investigating those who are symptomatic and where the differential diagnosis may lie between respiratory infection or HAPE. A biomarker that could detect an abnormally high PASP or HAPE at HA could significantly improve diagnosis, management, and outcome, similar to that seen with the use of biomarkers in CCF and acute coronary syndromes.
Footnotes
Acknowledgments
We thank all participants of DMS Bolivian Venture; Med and GS, DE and S, Foxhill, Donnington for equipment support; Alere Ltd, Cheshire for unconditional loan of Biosite machines.
Author Disclosure Statement
There is no conflict of interest to declare. This research was sponsored by the Surgeon General's Research Strategy Group and funded by the Joint Medical Command and the Drummond Foundation.