
Abstract
Abstract
He, Jiang, Jianhua Cui, Rui Wang, Liang Gao, Xiaokang Gao, Liu Yang, Qiong Zhang, Jinjun Cao, and Wuzhong Yu. Exposure to hypoxia at high altitude (5380 m) for 1 year induces reversible effects on semen quality and serum reproductive hormone levels in young male adults. High Alt Med Biol 16:216–222, 2015.—This study investigated the effect of hypoxia at high altitude on the semen quality and the serum reproductive hormone levels in male adults. A total of 52 male soldiers were enrolled in this cohort study. They were exposed to hypoxia at high altitude (5380 m) for 12 months when undergoing a service. After exposure, they were followed up for 6 months. The samples of semen and peripheral blood were collected at 1 month before exposure (M0), 6 months of exposure (M6), 12 months of exposure (M12), and 6 months after exposure (M18). The semen quality was assessed with computer-assisted analysis system, and the serum levels of reproductive hormones, including prolactin (PRL), luteinizing hormone (LH), follicle-stimulating hormone (FSH), and testosterone were analyzed by ELISA. Compared with those at M0, total sperm count, sperm density, motility, survival rate, and serum levels of LH, PRL and testosterone were significantly decreased, whereas the liquefaction time was significantly prolonged and serum FSH level was significantly increased at M6 (p<0.05). At M12, total sperm count and sperm density increased, whereas sperm motility, survival rate, and the liquefaction time further decreased. Sperm velocities, progression ratios, and lateral head displacements were also decreased. Serum FSH level decreased while serum LH, PRL, and testosterone levels increased. Compared with those at M6, the changes in these detected parameters of semen and hormone at M12 were significant (p<0.05). At M18, all these detected parameters except testosterone level returned to levels comparable to those before exposure. In conclusion, hypoxia at high altitude causes adverse effects on semen quality and reproductive hormones, and these effects are reversible.
Introduction
T
Similarly, chronic hypoxia causes a decrease in sperm count and sperm motility in men (Okumura et al., 2003; Verratti et al., 2008). In the study reported by Okumura et al., specimens were collected from subjects who stayed above 5100 m altitude for 21 to 24 days and above 6700 m altitude for 4 to 5 days. Subjects in the study reported by Verratti et al. were exposed to Karakorum Expedition (altitude ranging from 2000 m to 5600 m) for 26 days exposure. Interestingly, these reported effects of hypoxia are all reversible.
Although many studies on the effect of hypoxia at high altitude are reported, the results are controversial because of different models used, different altitude or different exposure time. The effect of hypoxia at 5380 m altitude on male reproduction after long time exposure (e.g., 12 months) is not reported and needs to be clarified.
The mainly affected reproductive hormones in male include prolactin (PRL), luteinizing hormone (LH), follicle-stimulating hormone (FSH), and testosterone. PRL is a protein hormone secreted by the pituitary gland. It has many functions such as promoting the development of mammary gland in females (Horseman et al., 1997) and promoting the growth of prostate and seminal vesicles in males (Nevalainen et al., 1997). FSH, a glycosylated protein hormone secreted by the anterior pituitary basophils, promotes spermatogenesis (Kumar et al., 2003). Testosterone, which is mainly secreted by Leydig cells of the testis, is the major type of androgens, with its synthesis regulated by LH (Bjelic et al., 2014).
Studies have reported the effects of hypoxia on the secretion of pituitary hormones (Basu et al., 1997; Savourey et al., 1998; Richalet et al., 2010). However, the results are controversial. For example, Çoksevim et al. (2006) reported that hormone levels of PRL, FSH, and LH were significantly increased after exposing to 3200 m altitude when compared with those at 1050 m altitude. However, the testosterone level did not change significantly. Instead, Sawhney et al. (1985) reported that after exposing to 3500 m high altitude, PRL level significantly increased whereas levels of LH and testosterone were significantly decreased. FSH level did not change significantly. Therefore, further studies are needed to clarify the role of hypoxia at high altitude in regulating pituitary hormone secretion.
This study is a cohort study of longitudinal research. A total of 52 male soldiers were enrolled and exposed to hypoxia at high altitude (5380 m) for 12 months. After exposure, they returned to 1400 m altitude and were followed up for 6 months. Thus, they were followed up for 18 months, including 12 months at high altitude and 6 months at 1400 m altitude. Peripheral blood and semen samples were collected before, during, and after exposure. The effects of hypoxia at high altitude on male reproductive functions, including semen quality and serum reproductive hormone levels, were investigated.
Materials and Methods
Subjects
This study is a cohort study of longitudinal research. Initially, 58 male adults going to serve the garrison at high altitude were included in this study. During follow-up, 6 of them were lost to follow up because of personal reasons. Thus, the data from 52 male adults was further analyzed. Their mean age was 20.8±1.5 years (ranging from 18 to 21 years). The inclusion criteria were listed as follows. All subjects were unmarried healthy males and did not live at high altitude before. They were all Chinese Han people. The average altitude of the area they usually lived in was 1400 m, while the average altitude of the garrison was 5380 m.
Subjects with chronic obstructive pulmonary disease, chronic pulmonary edema, diabetes, or apnea syndrome were excluded. Their average body mass index (BMI) was 21.47±0.63 kg/m2. Their average Sa
Prior written and informed consent were obtained from every patient and the study was approved by the ethics review board of Urumqi General Hospital of Lanzhou Command, PLA.
Specimen collection
Peripheral blood (5 mL) was collected from each subject at 8 o'clock in the morning during fasting period (which lasted for 10 h), and the serum was isolated 1 h later at room temperature. According to WHO criteria (World Health Organization, 2010), semen was collected by masturbation into sterile container from each subject after abstinence for 4 to 7 days, and then kept in 37°C water bath.
Semen analysis
The semen samples were analyzed according to the fifth edition of the WHO Laboratory Manual for the Examination and Processing of Human Semen (World Health Organization, 2010). The color, viscosity, and other properties of the semen samples were observed with naked eyes, whereas the liquefaction time and the semen volume were measured in completely liquefied semen. Semen parameters of the total sperm count, sperm density, motility, and survival rate were evaluated with the Sperm Class Analyzer (SCA) and computer-aided semen analyzer (MICROPTIC®, Barcelona, Spain).
The characteristics of sperm motility, including velocities, progression ratios, and lateral head displacements, were also assessed in these semen samples, which were indicated by the curvilinear velocity (VCL), average path velocity (VAP), and straight-line velocity (VSL); the linearity (LIN), straightness (STR), and wobble (WOB); the mean angular displacement (MAD), amplitude of lateral head displacement (ALH), and beat/cross frequency (BCF). Remaining semen specimens were centrifuged (500 g) to isolate seminal plasma, and then placed in −20°C.
ELISA
Reproductive hormone levels in serum, including PRL, LH, FSH, and total testosterone, were analyzed by commercial DRG ELISA kits (DRG Diagnostics GmbH®, Frauenbergstr, Germany) according to the manufactures' instructions. The reference range for FSH and LH was 2.0–10.0 mIU/mL and 3.0–12.0 mIU/mL, respectively. The reference value for PRL and testosterone was 6.44 ng/mL and 6.9 ng/mL, respectively. The absorbance value was measured with a BioTek ELx800 absorbance microplate reader (BioTek®, Winooski, VT, USA).
Statistical analysis
Data were expressed as mean±standard error (SE). Analysis was performed using SPSS software (version 10.0). Comparisons between each two time points were conducted with repeated measures analysis of variance (ANOVA) and subsequently post hoc test. A p value<0.05 was considered statistically significant.
Results
Semen quality before, during, and after exposure to hypoxia at high altitude
To investigate the influence of hypoxic environment at high altitude (5380 m) on the semen quality in male adults, the characteristics of semen volume, total sperm count, sperm density, motility, survival rate, and liquefaction time were assessed before, during, and after exposure to high altitude. As shown in Figure 1A, compared with that at M0, the semen volume at M18 was significantly increased (p<0.05). The total sperm count at M6 was significantly decreased (p<0.05) compared with that at M0 (Fig. 1B). Compared with that at M6, the total sperm count at M12 and M18 was significantly decreased (p<0.05).

Semen quality before, during, and after exposure to hypoxia at high altitude. The semen volume
Sperm density at M6 was also significantly decreased (p<0.05) compared with that at M0 (Fig. 1C). Sperm density at M12 increased than that at M6 but was still significantly lower than that at M0. Compared with that at M6, sperm density at M12 and M18 was significantly increased (p<0.05). Compared with that at M12, sperm density at M18 was significantly increased (p<0.05). As shown in Figure 1D, sperm motility at M6 and M12 was significantly lower than that at M0 (p<0.05). Compared with that at M6, sperm motility at M12 was further decreased (p<0.05). However, sperm motility at M18 returned to levels similar to that at M0 and was significantly increased than that at M6 and M12 (p<0.05).
Interestingly, the changes in sperm survival rate (Fig. 1E) were similar to those in sperm motility. Sperm survival rate decreased during high altitude exposure (M6 and M12) and returned to levels similar to that at M0 after exposure (M18). However, the changes in sperm liquefaction time were different from other indicators of semen quality. As shown in Figure 1F, compared with that at M0, the liquefaction time at M6 and M12 was significantly prolonged (p<0.05). At M18, the liquefaction time returned to levels similar to that at M0. Compared with that at M6 and M12, the liquefaction time at M18 was significantly shortened (p<0.05). Collectively, at M18, the levels of all the indicators of semen quality returned to levels similar to those at M0.
The parameters of sperm motility, including sperm velocities (Fig. 2A), progression ratios (Fig. 2B), and lateral head displacements (Fig. 2C and D), were also determined. As shown in Figure 2A, VSL, VCL, and VAP at M12 were significantly lower than those at M0 and M6 (p<0.05). However, compared with those at M12, VSL, VCL and VAP at M18 were significantly higher (p<0.05). These data indicate that sperm velocities are impaired during exposure to hypoxia at high altitude and are recovered after exposure.
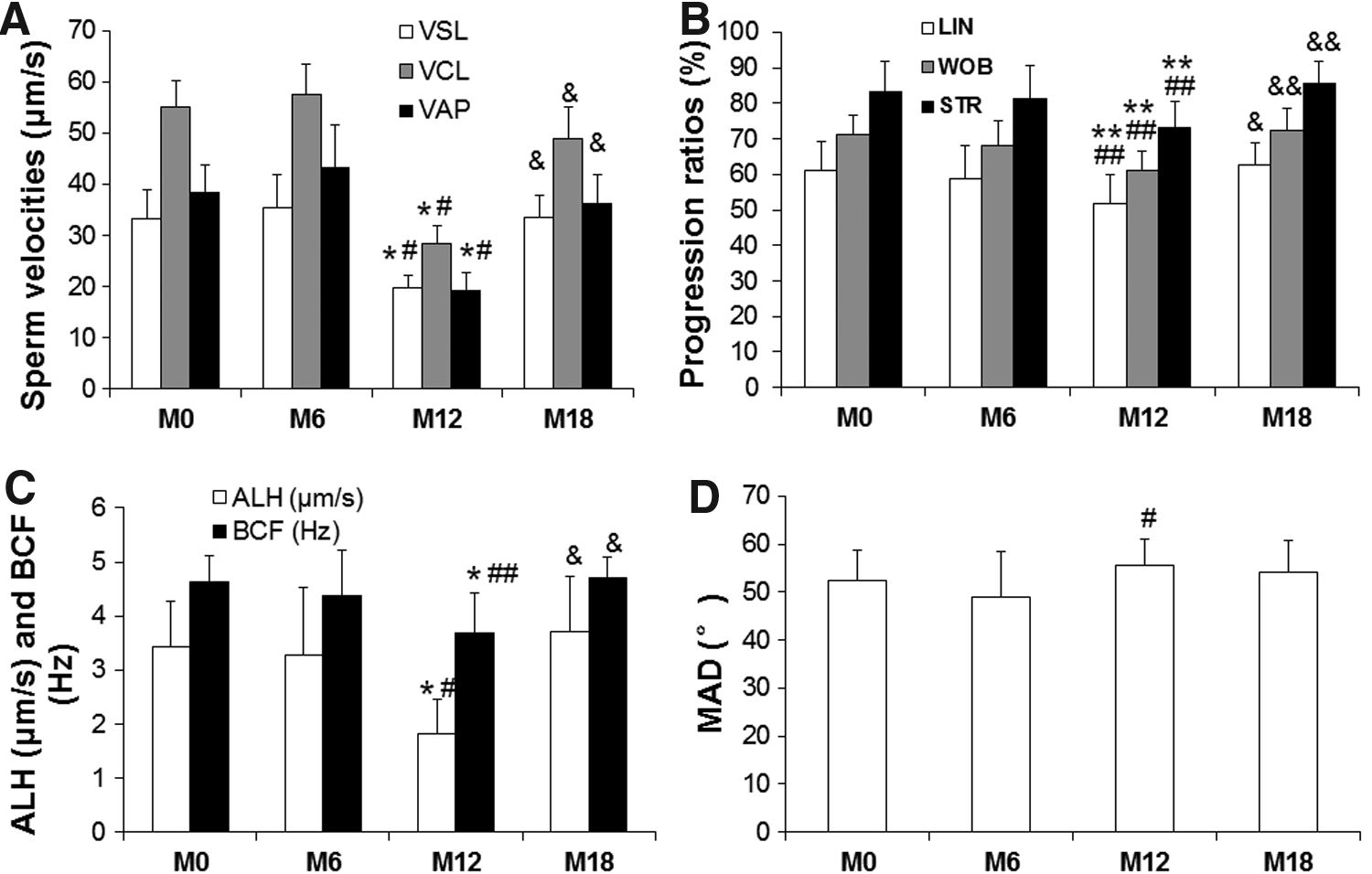
Sperm motility characteristics before, during, and after exposure to hypoxia at high altitude. The sperm movement properties of velocities (including VSL, VCL, and VAP)
As shown in Figure 2B, compared with those at M0 and M6, LIN, WOB and STR at M12 were significantly lower (p<0.05). However, at M18, LIN, WOB and STR were significantly higher than those at M12 (p<0.05), suggesting that progression ratios are recovered after exposure. Similarly, ALH and BCF at M12 were significantly lower than those at M0 and M6 (p<0.05), and were significantly lower than those at M18 (p<0.05) (Fig. 2C). As shown in Fig. 2D, MAD at M12 was significantly higher than those at M6 (p<0.05). This result also suggests that recovery in lateral head displacements is also observed after exposure. These results showed that the hypoxic environment at high altitude impaired the semen quality. However, at M18, this impairment on semen quality was recovered, suggesting that the effects of hypoxia at high altitude on semen quality are reversible.
Reproductive hormone levels before, during, and after exposure to hypoxia at high altitude
To further investigate the effects of hypoxic environment at high altitude on the levels of reproductive hormones in men, ELISA was performed to detect the serum levels of FSH, LH, PRL, and testosterone at indicated time points. As shown in Figure 3A, compared with that at M0, the serum FSH level was significantly increased at M6 (p<0.05). However, the serum FSH level at M12 was significantly decreased than those at M0 and at M6 (p<0.05). At M18, the serum FSH level was significantly decreased than that at M6 (p<0.05), but was significantly increased than that at M12 (p<0.05). At M6, the serum levels of LH (Fig. 3B), PRL (Fig. 3C), and testosterone (Fig. 3D) were significantly decreased than those at M0 (p<0.05).
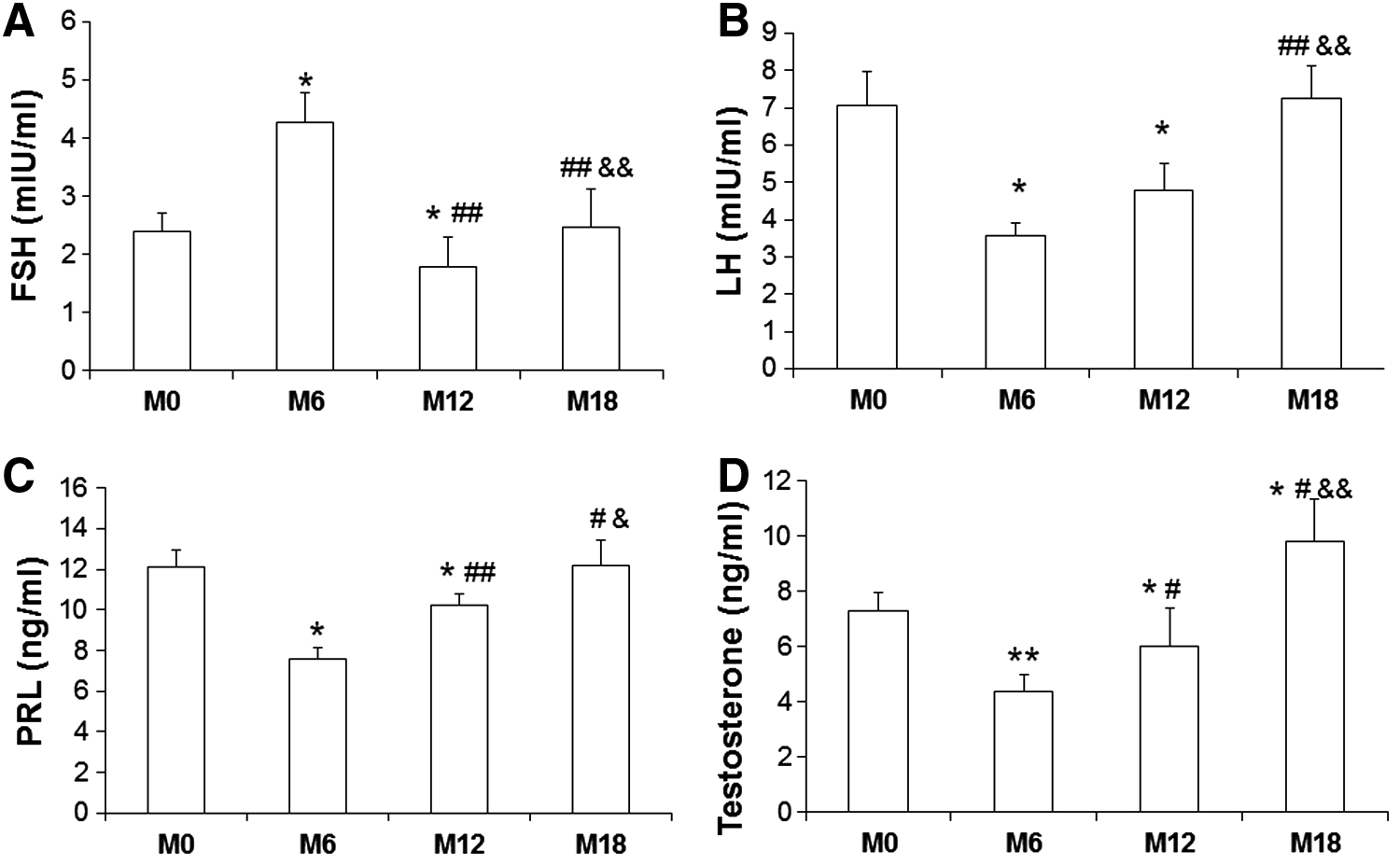
Reproductive hormone levels before, during, and after exposure to hypoxia at high altitude. The serum levels of FSH
At M12, the serum levels of LH, PRL, and testosterone were still significantly decreased than those at M0 (p<0.05). However, the serum levels of PRL and testosterone at M12 were significantly increased than those at M6 (p<0.05). At M18, the serum levels of LH, PRL, and testosterone were significantly increased than those at M6 and M12 (p<0.05). Interestingly, testosterone level at M18 was significantly increased than that at M0 (p<0.05). Collectively, the serum level of FSH was increased in hypoxic environment, but gradually decreased to normal level after exposure. The serum levels of LH, PRL, and testosterone were decreased during hypoxia exposure and gradually increased after exposure. These results indicate that the effects of hypoxia at high altitude on the levels of serum reproductive hormone are reversible.
Discussion
It is reported that hypoxia at high altitude is more likely to induce negative effects on male fertility in individuals living at sea level, compared to those living at higher altitudes for many generations (Verratti et al., 2008). For those living at higher altitudes for many generations, hypoxia at high altitude has little effect on their reproductive status and pregnancy status. This might be attributed to genetic adaption to high altitude (Abelson et al., 1974; Moore, 2001; Huerta-Sánchez et al., 2014). Pelliccione et al. (2011) reported that physical exercise at high altitude (5900 m) was associated with a testicular dysfunction. However, after a long recovery and adaptation in lower altitude areas, the semen quality could be gradually restored to the baseline level (Wan et al., 2012).
In our study, it was revealed that male adults had significantly decreased total sperm count, sperm density, motility, survival rate, and significantly prolonged liquefaction time, after 6 months of hypoxia exposure (M6). After 12 months of hypoxia exposure (M12), the sperm motility and survival rate were further reduced, whereas the total sperm count and sperm density began to recover. At 6 months after exposure (M18), all indicators returned to levels that were comparable to those at 1 month before exposure (M0).
Characteristics of sperm motility, including sperm velocities (VSA, VCL, and VAP), progression ratios (LIN, WOB, and STR), and lateral head displacements (ALH and BCF), were significantly decreased at 12 month of exposure (M12) whereas gradually increased at 6 month after exposure (M18). Our results were consistent with previous study (Wan et al., 2012), suggesting that high altitude hypoxia does exert adverse effects on male semen quality and that these adverse effects are reversible.
At high altitudes, hypoxia causes reduces in oxygen carried by hemoglobin, thus affecting many oxygen-dependent metabolic processes throughout the organism. Thus, the possible mechanisms underlying decreased sperm production and motility may be testicular ischemia and impaired seminiferous epithelium cells, which are caused by the increased blood viscosity and the poor venous return under chronic high altitude hypoxia (Saxena, 1995; Verratti et al., 2008). However, the specific mechanisms underlying the reversible effects of high altitude hypoxia on semen quality in this study still need further investigation.
Reproductive hormones play regulatory roles in human growth, development, reproduction, and aging, in addition to their sexual functions. Reproductive hormones can also regulate semen production. For example, PRL can promote the growth of seminal vesicles in male (Nevalainen et al., 1997). FSH promotes spermatogenesis (Kumar et al., 2003). The imbalance of reproductive hormones could lead to a series of target organ responses (Lue et al., 2013; Rey et al., 2013; Ribeiro et al., 2013; Szafarowska et al., 2013).
Under normal conditions, there are positive and negative feedbacks in the hypothalamus–pituitary–testicular axis, maintaining the efficiency of hormone regulations, and any factor disturbing the reproductive hormone balance may affect the male fertility (Moss et al., 2013). In our study, higher FSH levels and lower LH, PRL, and testosterone levels in serum were observed after 6 months of exposure (M6). After 12 months of exposure (M12), the serum FSH level was decreased, whereas serum LH, PRL, and testosterone levels were increased, suggesting that the effects of hypoxia at high altitude began to alleviate at 12 month of exposure (M12). In addition, the serum levels of FSH, LH, and PRL at 6 month after exposure (M18) were comparable to those before exposure.
Our findings suggest that the effects of hypoxia at high altitude on reproductive hormone levels are also reversible. Although both LH and FSH are stimulated by hypothalamic gonadotropin-releasing hormone, they have specific secretion types involving other regulatory hormones from pituitary, which would contribute to their different response patterns in high altitude-related hypoxic environment.
Testosterone is synthesized by a series of combined action of enzymes and cholesterols, in mitochondria and endoplasmic reticulum in Leydig cells, which is actually regulated by LH. High altitude hypoxia-induced LH and testosterone declines would probably be due to the decreased mitochondrial steroid dehydrogenase activity in acute and chronic hypoxia. Furthermore, changes in reproductive hormone levels under high altitude hypoxia may be also induced by changed levels of corticoids and epinephrine (Richalet et al., 2010).
Interestingly, the serum testosterone level at 6 month after exposure (M18) was still significantly higher than that before exposure (M0). We suppose that this may be a rebound effect. On the other hand, this also may be caused by the characteristics of subjects enrolled in this study. The subjects were soldiers and after the service at high altitude, they still underwent intense military training. Training and exercise can cause changes in the function of pituitary–testicular axis and stimulate the Leydig cells to produce testosterone, resulting in increased testosterone level in the serum. One study has shown that testosterone increase during exercise and moderate-intensity training is conducive to protein synthesis, which is needed during exercise (Métivier, 1985).
In conclusion, our study indicates that high altitude hypoxia has adverse effects on the semen quality and the reproductive hormone levels in the serum and that these adverse effects are reversible. Our findings may provide experimental evidence for understanding and further for treatment of male infertility under high altitude hypoxia in human.
Footnotes
Acknowledgments
This work was supported by the grants of the 11th Five Year Key Programs for Science and Technology Development of Chinese PLA (NO: 08G013) and the 11th Five Year Mandatory Programs for Science and Technology Development of Lanzhou Military Command of Chinese PLA (NO: LXH-2008031).
Author Disclosure Statement
All authors declare no competing financial interests.