
Abstract
Abstract
Ma, Lan, Ying Chen, Guoen Jin, Yingzhong Yang, Qin Ga, and Ri-Li Ge. Vascular endothelial growth factor as a prognostic parameter in subjects with “plateau red face.” High Alt Med Biol 16:147–153, 2015.—Some individuals living at high altitude on the Qinghai Plateau in China develop a red face called “ Plateau Red Face” (PRF). It is characterized by telangiectasia of the cheeks, which become a unique ruddy color. It is more common in young females than males, subjects who have polycythemia are more susceptible to PRF, and its pathogenesis is unknown. The aim of this study was to investigate associations between PRF and levels of vascular endothelial growth factor (VEGF).
Methods:
A total of 158 subjects (82 male and 76 female) residing at 4300 m and 140 subjects (73 male and 67 female) residing at 2260 m on the Qinghai Plateau, China, participated in this study. The determination and magnitude of PRF is evaluated by the dilation of veins on the face in the Qinghai chronic mountain sickness(CMS) score, established during the World Congress in 2004. Arterial O2 saturation (Sa
Results:
The occurrence of PRF was 32.9% (52/158) among subjects living at 4300 m and 15.7% (22/140) among those living at 2260 m. The levels of VEGF in PRF and non-PRF subjects were 399.9±115.6 pg/mL and 270.7±78.1 pg/mL, respectively (p<0.001) at 4300 m, and 244.4±109.0 pg/mL and 135.6±65.3 pg/mL, respectively (p<0.01) at 2260 m. However, comparing the levels of VEGF between the genders and ethnic groups at the same altitude, there were no significant differences between male and female both in Xining (p=0.12) and Maduo (p=0.18). There was also no significant difference between Tibetan and Han nationality in Xining (p=0.71), but In Maduo, the levels of VEGF in Han (351.70±122.62 pg/mL) were higher than that of Tibetan (300.20±102.89 pg/mL), and there was significant difference (p=0.01). Sa
Conclusion:
Chronic hypoxemia may stimulate overproduction of angiogenic cytokine (VEGF), and this peptide may lead to formation of abnormal new vessels and development of congestion in mucosa and conjunctiva. Thus, VEGF may, at least in part, serve as a marker of the pathophysiologic trigger for PRF.
Introduction
M
Most subjects with PRF are asymptomatic other than facial redness, and there are no effects limiting physical actively or daily life. However, subjects with an extremely high concentration of Hb often suffer severe hypoxemia and exhibit expanded telangiectasia. The causes of PRF are unknown, it is generally believed that exposure to high-altitude mutiple factors (West, 2012), such as hypoxia, cold temperatures, strong winds, and strong ultraviolet rays may lead to PRF due to dilation of the small blood vessels of the face (Penaloza and Arias-Stella, 2007). In this report, we hypothesize that vascular endothelial growth factor (VEGF), as a key mediator of angiogenesis (Tissot et al. 2005), may be associated with the formation of PRF. VEGF is essential for angiogenesis during embryonic development, wound healing, and tumor growth, and the expression of its gene is mainly stimulated by hypoxia through mediation of hypoxia-inducible factors (HIF). HIF-mediated gene expression might take place in the development of PRF as a result of severe high-altitude hypoxia. Based on these considerations, the hypothesis of the present study is that VEGF is associated with the development of PRF.
Materials and Methods
Subjects
A total of 158 subjects (mean age 42±13 years) residing at an altitude of 4300 m in Maduo, China, and 140 subjects (mean age 39±14 years) residing at 2260 m in Xining, China, participated in this study. Most of the subjects in Maduo are nomads and permanently live at altitudes of 4300–5000 m, while the Xining (2260 m) subjects were mostly Han Chinese (Table 1). The research protocol was approved by the human subject protection committee at the Medical College of Qinghai University. Informed consent was obtained from each subject.
Data expressed as mean±standard deviation unless otherwise specified; BMI, body-mass index; FEF25%-75%, mean forced expiratory flow during half of the forced vital capacity; FEV1%, percent of forced expiratory volume in 1 second; Hb, hemoglobin; HR, heart rate; mPAP, mean pulmonary arterial pressure; MVV, maximal voluntary volume; SaO2, oxygen saturation; VEGF; vascular endothelial growth factor.
Assessment of PRF
The presence of PRF was determined by the Qinghai chronic mountian sickness (CMS) score (León-Velarde et al., 2005). The magnitude of facial redness was determined by the examining physician (GRL) according to the ruddiness of the surface area and the dilation of veins of the cheeks, and graded as mild, moderate, or severe.
Measurements
Arterial O2 saturation (Sa
Blood sampling and assay
A 3 mL blood sample was drawn from the brachial vein of all participants (n=298), collected into a serum separator tube, and allowed to sit for 15 min at 4°C before centrifugation (3000 rpm for 10 min). Serum samples were stored in liquid nitrogen for analysis. Serum VEGF was measured with an enzyme linked immunosorbent assay (ELISA) kit (D&R system), which was described previously (Ge et al., 2011). This assay was calibrated against highly purified recombinant human VEGF 165. The measurable range of the VEGF assay was 31.2–2000 pg/mL.
Statistical analysis
All measurement data were normal distribution, and the data are expressed as mean±SD. All count data are expressed as percentage. Statistics were done using SPSS software (version 13.0; Chicago, IL). Comparison of various parameters between subject groups was made by Fisher protected least significant difference test at the 95% significant level. A Student's unpaired t-test was used in comparing PRF and non-PRF groups. All count data used Chi-square test. Linear regression analysis was used to assess the correlation between variables. Receiver operator characteristic (ROC) curves (Analyze-it; Leeds, UK) examined VEGF, Sa
Results
General characteristics
The clinical characteristics of subjects with and without RPF in Maduo and Xining are shown in Table 1. In Maduo, most subjects were Tibetan natives, only 40 subjects were Han Chinese. The rate of occurrence of PRF was 32.9% (52/158 at an altitude of 4300 m and 15.7% (22/140) at 2260 m. There was no significant difference in the rate of PRF between genders in both areas (Table 2). Severity of PRF in Maduo subjects: 15 of 52 subjects were mild, 21 moderate, and 16 severe. In Xining, 11 of 22 subjects were mild, 8 moderate, and 3 severe, and there were no significant differences at the two altitudes (p=0.15) (Table 3).
Symptoms
Most subjects with PRF were asymptomatic, but a few severe PRF subjects, specially Han Chinese in Maduo, showed clinical symptoms such as headache, breathlessness, fatigue, sleep disturbance, and cyanosis, whereas these were absent in the Xining group.
Variables between PRF and non-PRF
Table 1 showed that there were no significant differences in vital capacity, percentage of forced expiratory volume in 1 sec, mean forced expiratory flow during the first half of the forced vital capacity (25%–75%), or maximal voluntary ventilation values between the two groups at different altitudes, suggesting that subjects with and without PRF were absent of chronic obstructive pulmonary disease.
Sa
Multivariate regression analysis
Table 4 showed that several confounding factors, especially age, Hb, VEGF, and FEF25%–75% were related to the severity of PRF. The predictors of the severity of PRF included VEGF (β=0.642; p<0.0001), Hb (β=0.116; p=0.05), age (β=−0.310; p<0.0001), and FEF25%–75% (β=−0.118; p=0.035).
Biomarkers
Serum VEGF levels were significantly higher in the PRF group than in the non-PRF group (p<0.01), both in Maduo and Xining (Fig. 1). Comparing the serum VEGF levels between Tibetan and Han nationality at different altitudes, the results showed that the VEGF levels in Maduo were significant higher than in Xining, both Tibetan group and Han group (p<0.001), and it was higher in Han Chinese than Tibetan in Maduo (p<0.05), but there was no significant difference in Xining (p>0.05) (Fig. 2). We also compared the serum VEGF levels between male and female. The results showed that the VEGF levels in Maduo were significant higher than in Xining both in male and female (p<0.001), but there were no significant differences between male and female both in Maduo and Xining (p>0.05) (Fig. 3).

Concentrations of vascular endothelial growth factor (VEGF) in the subjects with or without plateau red face (PRF) at the altitude of 4300 m (Maduo) and 2260 m (Xining). The PRF group showed significantly higher levels of VEGF than did non-PRF group both in Maduo and Xining. The VEGF levels in Maduo were significantly higher than in Xining both the PRF group and non-PRF group. *p<0.001 compared with non-PRF at the same altitude, #p<0.001 compared with Maduo.
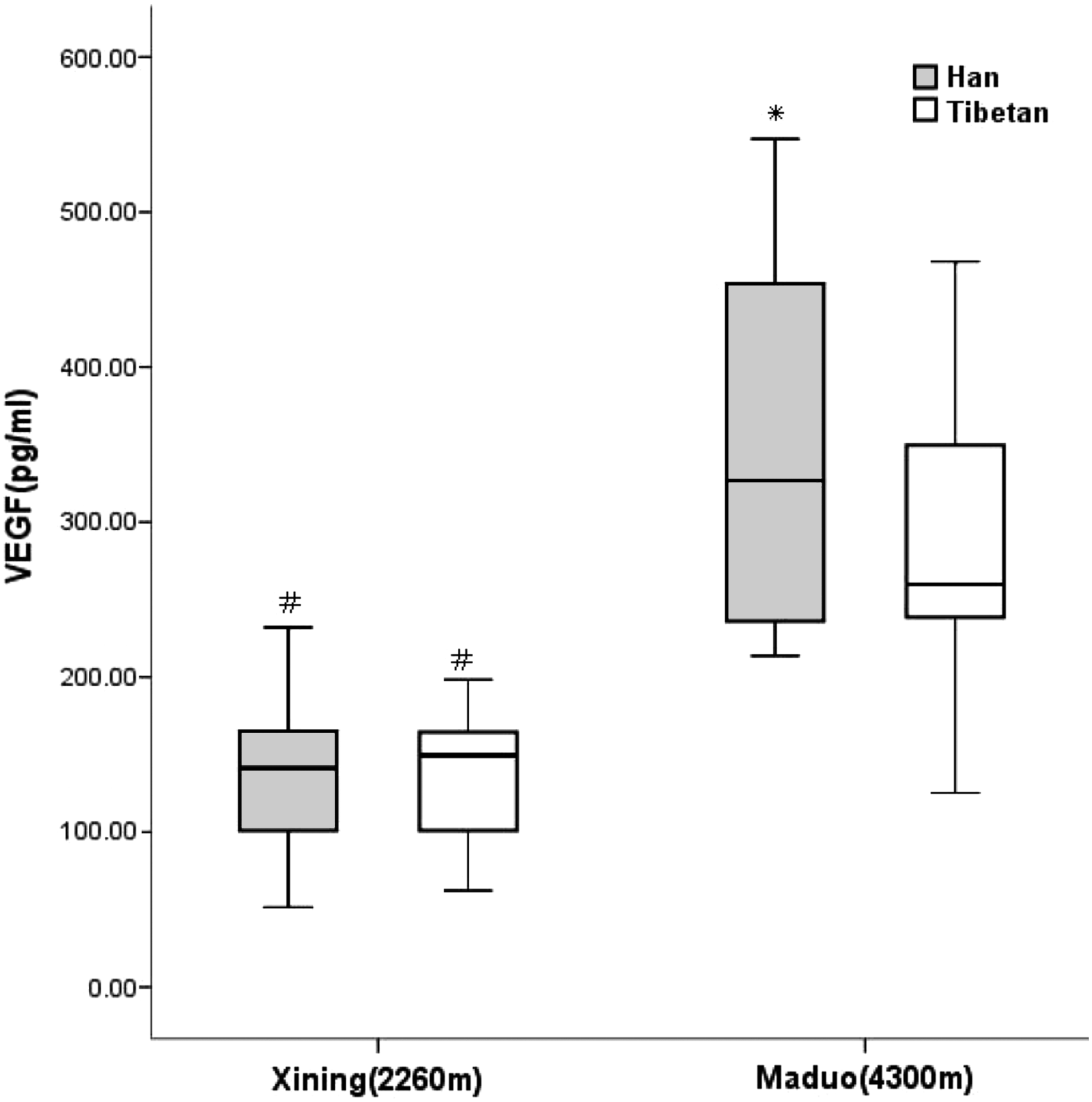
Concentrations of vascular endothelial growth factor (VEGF) in the Tibetan and Han Chinese at the altitude of 4300 m (Maduo) and 2260 m (Xining). The VEGF levels in Maduo were significantly higher than in Xining in both Tibetan group and Han group. The Han group showed significantly higher levels of VEGF than Tibetan group in Maduo, whereas no significant difference in Xining. *p<0.05 compared with Tibetan group, #p<0.001 compared with Maduo.
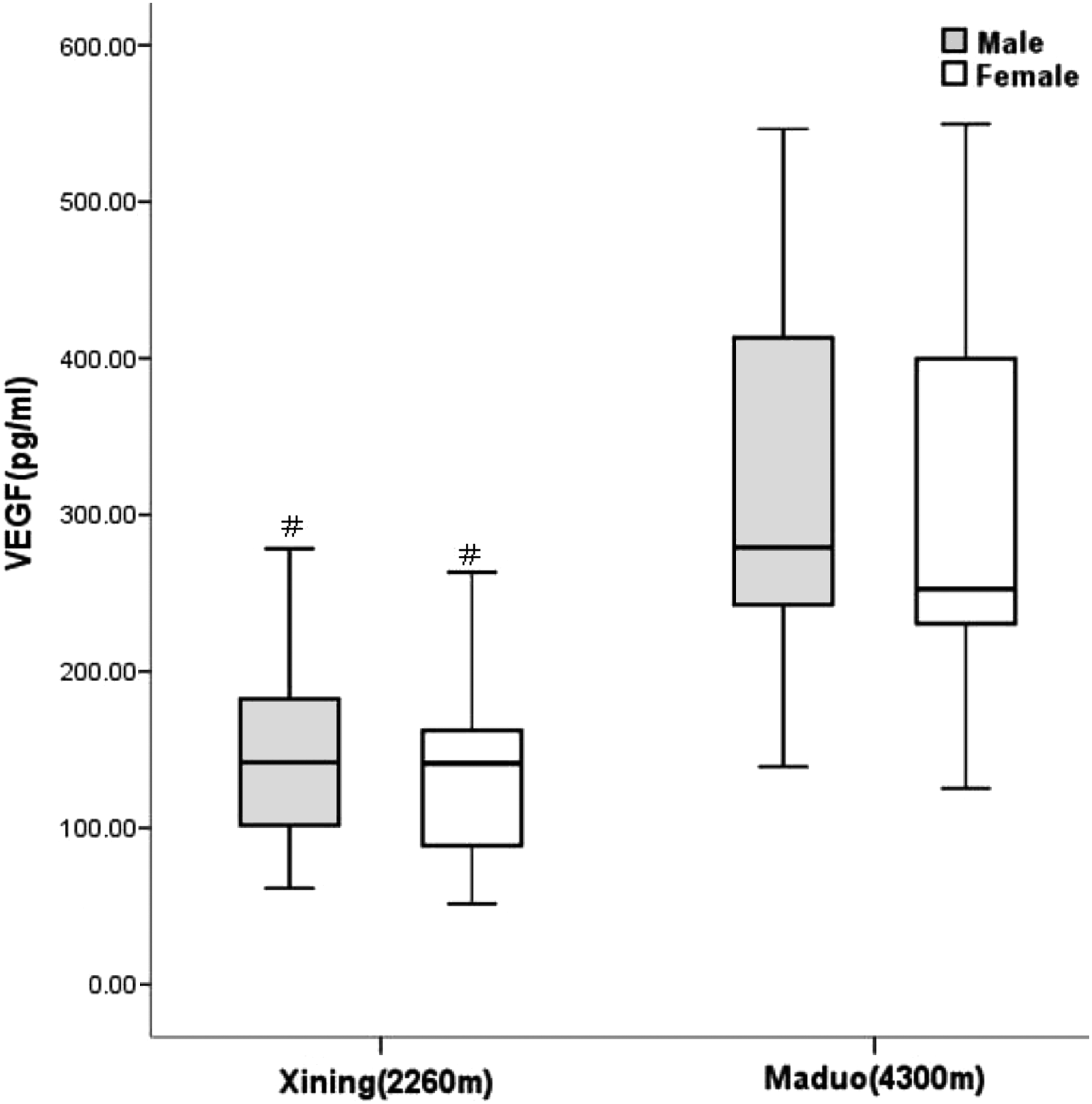
Concentrations of vascular endothelial growth factor (VEGF) in males and females at the altitude of 4300 m (Maduo) and 2260 m (Xining). The VEGF levels in Maduo were significantly higher than in Xining, both in males and females, but there were no significant differences between males and females in either Maduo or Xining. #p<0.001 compared with Maduo.
Correlations and ROC analyses
VEGF levels correlated positively with Hb levels both in Maduo and Xining (Figs. 4A and 5A), and negatively with Sa

Correlation of Hb

Correlation of Hb
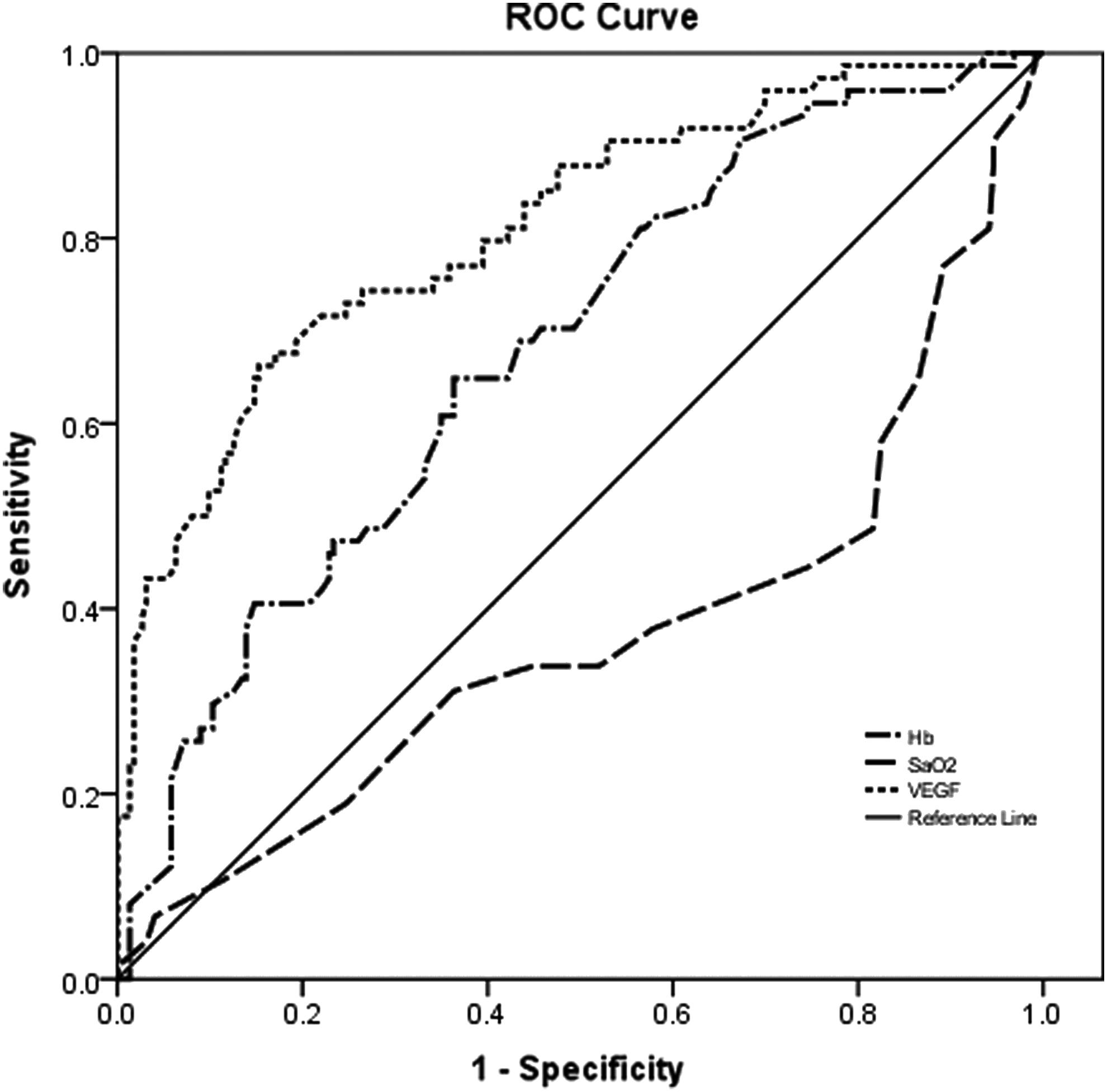
Receiver operator characteristic curves (depicting the balance of sensitivity and specificity) for VEGF, Sa
Discussion
The new findings of this study are that people living at high altitude may form a unique redness (telangiectasia) of the face, including the cheeks, ear edges, bridge of the nose, and conjunctivae, and those subjects with this ruddy facial color have significantly elevated VEGF levels that are proportionate to the severity of the red facial color. Our data suggest that a number of complex environmental stresses experienced at high altitudes, such as hypoxia, cold weather, and strong ultraviolet light, may lead to higher circulating concentrations of this important angiogenesis compound, which appears to induce the formation of abnormal, new blood vessels of the skin and mucosa, causing the red face and cheeks seen in some people living at high altitudes.
There are two major kinds of environmental stresses at high altitude for humans (Hultgren,1997). First, there are the alternating daily extremes of climate that often range from hot sun during the day to freezing nights. In addition, winds are often strong and humidity low, resulting in rapid dehydration. Second, the air pressure is low, which makes it more difficult for oxygen to enter the body, resulting in hypoxia. The climate of Maduo, when compared with Xining, is characterized not only by a lower air pressure (barometric pressure 440 mmHg), but also by a number of complex and interlinked environmental stressors (Ge et al., 1998). The mean annual ambient temperature is 0.2–2.5°C, with a minimal temperature of −35°C. We have frequently observed during physical examination that high altitude residents, particularly subjects with excessive polycythemia, exhibit the ruddy or erythemic facial color, which is called PRF in the Qinghai Plateau, China, and is more common in females (Fig. 7).

A 33-year-old Tibetan woman who has permanently lived at 4300 m, her face was erythremic colored, called “plateau red face.” Hemoglobin was 23 g/dL and VEGF was 530 pg/mL, with telangiectasia of the cheeks.
This ruddy color most commonly appears in the face and cheeks, but can also extend over the bridge of the nose, around the mouth, and to the conjunctivae. Most PRF subjects, especially Tibetan natives, are asymptotic, making it unlikely to be a sign of maladaptation to high altitude. On the contrary, it seems to be a positive adaptive response because the ruddiness is primarily due to increased blood flow near the skin surface, providing more oxygen to body tissues. In the present study, we found PRF in 32.9% of subjects living at an altitude of 4300 m and 15.7% of subjects at 2260 m, suggesting that the occurrence of PRF is closely related to the severity of hypoxic environmental stresses.
High altitude environmental stressors, particularly hypoxia, may lead to a decrease in Sa
VEGF is a 45-kD homodimeric glycoprotein stimulating normal and abnormal vessel growth, and is essential for neoangiogenesis during embryonic development, wound healing, and tumor growth (Okada et al., 2014). Expression of the VEGF gene is mainly stimulated by hypoxia through mediation of hypoxia-inducible factors (HIF), and is upregulated in vascular smooth muscle cells and endothelial cells under hypoxic conditions (Hubbell et al., 2012; Adeoye et al., 2013; Pichon et al., 2013). Studies (Walter et al., 2001; Hanaoka et al., 2003; Dorward et al., 2007) have shown that circulating VEGF levels may significantly increase when sea level residents acutely ascend to a high altitude, and overproduction of VEGF in the lung attenuates the development of hypoxic pulmonary hypertension due to the protection of an endothelium-dependent function (Partovian et al., 2000; Louzier et al., 2003; Wu et al., 2013).
We also reported previously that significant elevated serum VEGF has been shown in patients with chronic mountain sickness. In the present study, we found that mean levels of serum VEGF in the Maduo group (313.24 pg/mL) was significantly higher than that of the Xining group (152.75 pg/mL; p<0.001). Furthermore, the PRF groups both in Maduo and Xining had significantly higher levels of VEGF than those of non-PRF groups (Fig.1), which have associated lower levels of Sa
The pathophysiological consequences of increased VEGF production at high altitudes might contribute to new vessel formation, along with remodeling of pulmonary vessels, proliferation of vascular smooth muscle cells, and consequent loss of distal functional arteries; each of these changes is a potential contributor to the development of PRF. Regardless, how to cure PRF is difficult to answer. The cause of PRF appears to be increased blood circulation due to neoangiogenesis due to high-altitude environmental stressors, and there is no useful method of eliminating or ameliorating this at the present time. But from our study, we clearly recognized that the residents at high altitude could prevent or alleviate the incidence of the PRF by reduced sunlight exposure, greater use of face coverings, and change in altitude. Future studies should concern the multifactors, except high-altitude environment, which influence the incidence of PRF. How to prevent or reduce the incidence of PRF will also be key points in the study of the PRF, with experiments that intervene or perturb the proposed mechanisms, such as pharmacological interventions.
Conclusions
People living at an altitude of 4300 m on the Qinghai Plateau, China, have a higher proportion of red face and cheeks (PRF) than people living at lower altitudes. Those subjects with ruddy facial color have significantly higher levels of serum VEGF when compared to subjects without PRF. The elevation of VEGF was highly positively correlated with the severity of PRF. The mechanism that produces the PRF is not known; however, the environmental stresses of extreme high altitude, such as hypoxia and strong ultraviolet light may stimulate overexpression of VEGF, which perhaps can serve as a marker of PRF.
Footnotes
Acknowledgments
This project has been supported by the National Basic Research Program of China (Grant No.2012CB518200), the Program of International Science and Technology Cooperation of China (Grant No.2011DFA32720), the National Natural Science Foundation of China (Grant No.31160219), and Key Laboratory Special Development of Qinghai Province (Grant No. 2014-Z-Y-30 and 2014-Z-Y-07).
Author Disclosure Statement
No conflicting financial interests exist.