
Abstract
Abstract
Li, Suzhi, Yuliang, Wang, Xuewen Huang, Jingxin Cao, and Dingzhou Yang. Diffuse alveolar hemorrhage from systemic lupus erythematosus misdiagnosed as high altitude pulmonary edema. High Alt Med Biol 16:67–70, 2015.—A 26-year-old woman presented with dyspnea and dry cough soon after arriving on the Qinghai-Tibet Plateau (3650 m). Chest radiograph showed diffuse patchy infiltrates. The initial diagnosis was high altitude pulmonary edema (HAPE). However, the patient had no sputum or moist rales, and supplemental oxygen and intravenous aminophylline produced no improvement. Chest HRCT revealed symmetric and diffuse ground glass opacities. Further examination found anemia, leukopenia, urine abnormalities, and increased erythrocyte sedimentation rate. Antibodies for ds-DNA and ANA were positive. Hemoptysis and arthralgia developed after a few days. Finally the patient was diagnosed with diffuse alveolar hemorrhage secondary to systemic lupus erythemetosus.
Conclusion:
When considering a diagnosis of HAPE, careful attention to physical signs, and a clinical course that is atypical for HAPE should prompt evaluation for other disease processes; HRCT can be useful in this setting.
Introduction
H
This study was conducted in accordance with the amended Institutional Review Board (IRB) Approval/Helsinki Declaration. The Ethics Committee of Xizang Military District approved the protocol, approval number KY201409. Written informed consent was obtained from patient's relatives.
Case report
A 26-year-old woman came to Lhasa (altitude 3650 m) from sea level by air in April 2014. She was initially asymptomatic. After 3 days, however, she developed fever, dyspnea, and nonproductive cough. She was diagnosed with “acute high altitude reaction” and received intravenous aminophylline and oxygen. Dyspnea worsened over the next 2 days, and a chest radiograph showed diffused patchy infiltrates (Fig. 1). The patient was sent to our hospital, where she was diagnosed with HAPE and sent to the high altitude disease department at once.

X-ray chest film shows multiple diffused patch shadows (arrows), particularly in perihelar area.
Examination on admission revealed: body temperature 39.5°C, pulse rate 130 beats per minute, blood pressure 105/75 mmHg, obvious cyanosis, coarse breath sounds, and no obvious dry or moist rales. Laboratory studies showed: WBC 3.05×109/L, RBC 2.30×1012/L, Hb 82 g/L, ESR 95 mm/h, urine protein (+), and urine erythrocytes (+). Arterial blood gas analysis (on room air at 3650 m.) was: pH 7.35, P
High-resolution computerized tomography (HRCT) of the chest revealed diffuse ground glass opacities, mediastinal lymphadenopathy, and pleural effusion (Fig. 2). Serum antinuclear antibody (ANA) and anti-ds DNA antibody were positive. Sputum was negative for tubercle bacillus, bacteria, and fungi. Cardiac and abdominal ultrasounds were normal. Electrocardiogram showed only nodal tachycardia.
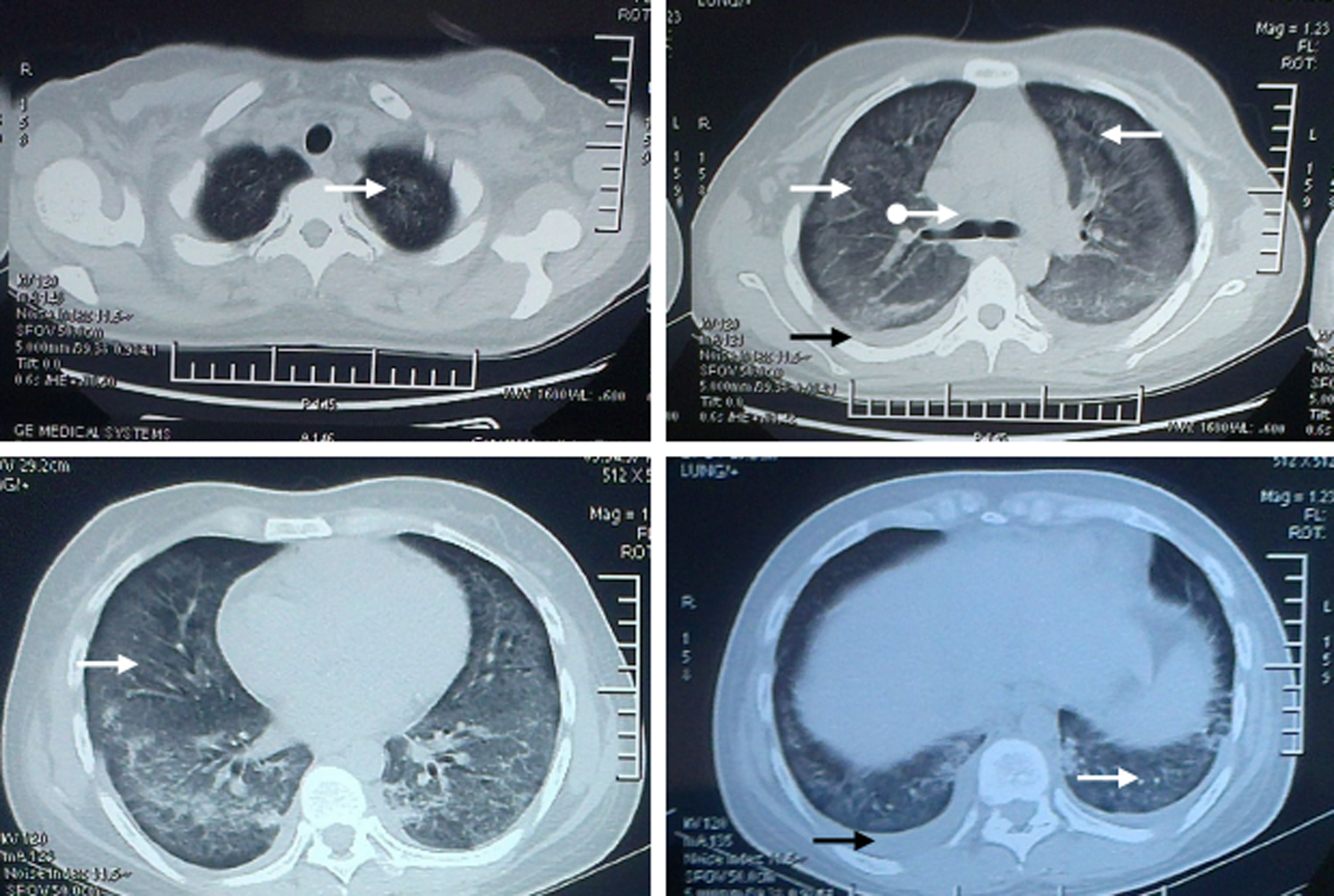
Chest HRCT image shows symmetric and diffused ground glass shadows (white arrows), multiple mediastina lymphadenectasis (white arrows with round tail), and bilateral small amounts of pleural effusion (black arrows).
Systemic lupus erythematosus (SLE) was considered, since the patient was a young female with positive ANA and anti-ds DNA antibodies, anemia, proteinuria and hematuria, leukopenia, and unexplained diffuse pulmonary infiltrates. The patient received intravenous methylprednisolone 400 mg a day. Her body temperature dropped to normal 2 days after administration, and dyspnea was relieved dramatically at the same time. The patient was then transferred by train to sea level for further treatment.
Follow up
Two days after return to sea level, the patient again developed high fever and dyspnea, along with diffuse arthralgia. Hemoptysis ensued, with daily hemoptysis volume of 800–1000 mL. The patient was diagnosed with diffuse alveolar hemorrhage (DAH), and then received cyclophosphamide in addition to methylprednisolone. However, her condition deteriorated and she died of respiratory failure in 3 days.
Discussion
In this case, a young woman developed respiratory distress within days of arrival to high altitude. Her clinical manifestations, hypoxemia, and chest x-ray seemed to match HAPE. However, her minimal dry cough and absence of moist rales were not in accordance with HAPE nor with the extensive findings on chest imaging. Further, she did not respond to the usual therapy for HAPE. She ultimately expired from diffuse alveolar hemorrhage due to SLE.
HAPE may present with no or minimal nonproductive cough at an early stage (Eldridge et al., 2006; Zheng et al., 2010), but with progression of the illness to the point of severe hypoxemia and respiratory distress, cough and expectoration would be expected, and the characteristics of sputum would evolve from scant yellow or white sputum to copious pink frothy sputum. Moist rales would increase at the same time. These changes are due to increasing exudation in pulmonary alveoli (Li et al., 1995; Maggiorini, 2006; Schoene, 2008; Paralikar, 2012; Swenson and Bartsch, 2012; Bhagi et al., 2014). In this case, the minimal dry cough, absence of moist rales, and extensive disease on HRCT could not be easily explained by HAPE.
Other diseases can certainly present similarly to HAPE. Chen Shixun reported a tuberculosis case misdiagnosed as HAPE. The patient, recently arrived to high altitude, presented with a nonproductive cough, and chest CT displayed multiple lobular infiltrates (Chen, 2003). Patients with pulmonary embolism (PE) present with obvious dyspnea and sometimes multiple infiltrates on chest radiography, and PE may be misdiagnosed as HAPE. However, the majority of the PE cases misdiagnosed as HAPE show dry cough and small amount of moist rales (Shlim and Papenfus, 1995; Khan et al., 2003). Plague might mimic HAPE by presenting with chest tightness, frothy bloody sputum, and extensive infiltrates on chest x-ray. Like PE, few scattered rales can be heard in plague patients especially at the early stage (Zhang et al., 2011). Discrepancy between symptoms, physical exam, and imaging findings should raise the suspicion for other diseases than HAPE.
The presence of a high fever as in this patient is also unusual in HAPE. Some literature does not list fever as a typical sign of HAPE (Schoene, 2008; Fiore et al., 2010), while other reports indicate fever may accompany HAPE and that its presence does not mean infection (Taylor, 2011). Mou Xinbing found HAPE patients had higher body temperature and increased plasma CRP, together with large amounts of protein, erythrocytes, and inflammatory cells in bronchoalveolar lavage fluid. He considered fever might be a manifestation of nonseptic inflammation (Mou et al., 2002; Cao et al., 2003). HAPE usually presents with transient and low-grade fever (Mou et al., 2002; Cao et al., 2003), while persistent high fever should be considered due to other diseases or to concomitant infection. In our patient, lack of purulent sputum, a low WBC, and negative sputum studies ruled out infection, and contributed to looking for other processes.
HAPE is caused by inhomogeneous pulmonary hypertension and vascular endothelial leakage; pulmonary imaging generally shows asymmetric patchy airspace consolidation (Wang et al., 2004). However, these findings are not specific to HAPE, and thus chest x-ray must be interpreted in relation to other clinical factors. In this case, the chest x-ray was consistent with HAPE, (Gluecker et al., 1999) but some clinical factors were not, and HRCT showed marked decrease of lung radiolucency and diffuse symmetrical ground glass shadows. Compared with HAPE, the HRCT finding was more consistent with the diffuse pulmonary alveolar exudation of connective tissue disease (Lara and Schwarz, 2010; Vij and Strek, 2013). HRCT can more clearly define pulmonary processes than ordinary chest film (Gluecker et al., 1999), so it is frequently used in the differential diagnosis of HAPE when there is consideration of other diseases. (Chen, 2003; Khan et al., 2003; Zhang et al., 2011). We suggest that HRCT should be considered in HAPE earlier when diagnosis is in doubt.
In our patient, mediastinal lymphadenopathy was also atypical and suggested an inflammatory, malignant, or immune disease. In addition, only rarely do HAPE patients develop pleural effusions. (Vock et al., 1991; Wang et al., 2004; Zhang et al., 2011). Thus, both of these findings indicated the possibility of another disease than HAPE.
Finally, the clinical course of our patient was not consistent with HAPE. After administration of aminophylline and oxygen in Lhasa (3650 m), the majority of HAPE patients has immediate improvement and totally recover in about 40 hours (Mou et al., 2003; Li et al., 2010). In this case, the patient had no response to aminophylline, but a good response to administration of methylprednisolone. Steroids are not helpful in HAPE. In a retrospective series of 2016 patients with HAPE (Mou et al., 2003), the dexamethasone group had nearly double the time for recovery compared to the aminophylline group, indicating that glucocorticoids were not ideal for treatment of HAPE. Thus, our patient's clinical course was atypical for HAPE and the strongest clinical indication to consider other diseases.
Could our patient's exacerbation and complications of SLE have been triggered by going to high altitude? We do not know. Hypoxia may induce immune system changes, including abnormal macrophage migration (Bosco et al., 2008) and decreased MHC-II-dependent antigen presenting ability (Moslehi and Libby, 2012). Theoretically, hypoxia could influence progression of SLE, but there has been no research on this issue. For complications of SLE, it is well known that the chronic hypoxia due to damage of the kidney small vascular bed may induce chronic kidney failure (Fine and Norman, 2008; Ma et al., 2012), but whether the hypoxic environment of the plateau can affect lupus nephritis, and with a short exposure is still unknown. Also, whether this patient had pre-existing pulmonary hypertension that might have aggravated pulmonary vascular leak and hemorrhage is unknown. Her normal echocardiography, however, speaks against this possibility.
Conclusion
A confident diagnosis of HAPE requires integrated medical history, clinical symptoms, physical signs, x-ray findings, and clinical course. Atypical elements, especially lack of response to the usual therapy, should prompt an evaluation for other diseases. Chest CT can be most helpful in this regard.
Footnotes
Acknowledgments
Funding; The essay has not been funded by any foundation.
The essay has not been published or presented in any prior meetings.
Author Disclosure Statement
Authors Wang Yu Liang, Li Su zhi, Huang Xue Wen, Cao Jing Xin and Yang Ding Zhou have reported that no potential conflicts of interest exist with any companies/organizations whose products or services may be discussed in this article.