
Abstract
Abstract
Lipman, Grant S., Nicholas C. Kanaan, Caleb Phillips, Dave Pomeranz, Patrick Cain, Kristin Fontes, Becky Higbee, Carolyn Meyer, Michael Shaheen, Sean Wentworth, and Diane Walsh. Study Looking at End Expiratory Pressure for Altitude Illness Decrease (SLEEP-AID). High Alt Med Biol 16:154–161, 2015.—Acute mountain sickness (AMS) affects 25%–70% of the tens of millions of high altitude travelers annually, with hypoxia and nocturnal desaturations as major contributing factors. This is the first double blind randomized placebo controlled trial to assess expiratory positive airway pressure (EPAP) for AMS prevention and nocturnal hypoxic events. Healthy adult participants trekking in the Khumbu region of the Himalayas were randomized to a single-use EPAP nasal strip, or a visually identical sham device (placebo) prior to first night sleeping between 4371–4530 m (14,340–14,800 ft). The primary outcome was AMS incidence, measured by Lake Louise Questionnaire (LLQ), with secondary outcomes of AMS severity (by LLQ) and physiologic sleep indices measured by continuous sleep monitor. Intent-to-treat analysis included 219 participants with comparable demographic characteristics, of which 115 received EPAP and 104 placebo. There was no decrease in AMS with EPAP intervention (14% EPAP vs. 17% placebo; p=0.65; risk difference
Introduction
A
The low barometric pressure at high altitude results in a lower partial pressure of oxygen leading to lower oxygen saturations. There appears to be a central role of hypoxemia causing AMS (Sutton et al., 1979; Bartsch et al.,1990; Roach et al., 1998; West, 2003), where the ability to compensate for hypoxia dictates subsequent altitude illness as well as mental and physical performance. Oxyhemoglobin saturation decreases during sleep at high altitude (Hultgren, 1997), and individuals who develop AMS consistently have lower nighttime oxygen saturations (Burgess et al., 2004; Erba et al., 2004). Sleep at high altitude has been found to be a more powerful instigator of desaturations then ambulation (Burgess et al., 2004), and nocturnal oxygen supplementation has been found to attenuate AMS and improve sleep quality (Luks et al., 1998; Barash et al., 2001).
Applied positive end-expiratory pressure (PEEP) increases airway and transpulmonary pressures, functional residual capacity, and arterial oxygenation (Duncan et al., 1986). Expiratory positive airway pressure (EPAP) applies constant positive pressure throughout the exhalation phase and is similar to PEEP, in that expiratory resistance is generated. Acute mountain sickness incidence and severity have been shown to decrease with both PEEP machine (Koch et al., 2008; Johnson et al., 2010; 2013) and EPAP-producing face mask with an expiratory valve (Savourey et al., 1998; Launay et al., 2004). However, current systems with face masks and valves are unwieldy, uncomfortable, and due to weight and space constraints are unlikely to be utilized by an expedition doctor, medic, or within the self-supported climber's first aid kit. The objective of this study was to examine whether a novel nasal EPAP device could decrease the incidence AMS, as well as improve AMS symptoms and sleep physiology metrics.
Materials and Methods
Study design and participants
This study was a double blind, randomized placebo controlled trial of Theravent™ (Ventus Pharmaceutical, San Jose, CA) nasal EPAP strip versus a visually identical ‘sham’ device for the prevention of acute mountain sickness and nocturnal hypoxia. The study was approved by Stanford University School of Medicine and University of Utah institutional review boards, the Nepal Health Research Council, and registered with ClinicalTrials.gov (NCT01842906).
Ascent to study enrollment sites
The approach to the study enrollment sites was a gradual ascent, with the majority of trekkers beginning after flying to the town of Lukla at 2860 m (9380 ft). Most trekkers took 5 days to ascend the 1670 m (5479 ft) to Dingboche 4530 m (14,800 ft) or Pheriche 4371 m (14,340 ft) (including an acclimatization day half way up in Namche Bazaar). The average daily altitude gain while hiking is 417 m (1368 ft), with the final 488 m (1601 ft) in the last day, reaching the enrollment site unacclimatized (Fig. 1).

Trekking ascent profile. *Study enrollment sites.
Selection of participants
The study was conducted from October through November 2013 in the Khumbu Himalaya. Trekkers who met inclusion criteria were recruited in Pheriche and Dingboche, and informed consent was obtained by the research staff. Participants were then randomized to the intervention group (EPAP device) or placebo (sham device). All participants were given self-reported questionnaires to complete the night of enrollment and upon awakening the following morning.
Eligible study participants included adults ages 18 to 65 who had not traveled above 4200 m (13,800 ft) in the preceding week and were spending their first night at the study enrollment altitude. Exclusion criteria included an inability to read the consent form in English, a diagnosis of AMS at time of enrollment, a previous diagnosis of obstructive sleep apnea, pregnancy or suspected pregnancy, and trekkers who had taken nonsteroidal anti-inflammatory drugs, acetazolamide, or corticosteroids in the 48 hours prior to study enrollment. Any potential participant with current symptoms of nasal congestion, rhinorrhea, sinusitis, upper respiratory infection, asthma, COPD exacerbation, pneumonia, bronchitis, or other disease of the respiratory tract were also excluded.
Intervention
Participants were randomized using computer-generated random sequence and given sealed numbered packages with their interventional device, Watch-PAT200™ continuous sleep monitor (Itamar Medical, Caesarea, Israel), questionnaires, and instructions. The randomization code was unavailable to administrators or participants. The sham device was prepared by manual removal of the device's interior gill-like strips that deliver 5 cm H2O of resistance to expired nasal airflow (Doshi, 2012; personal communication), maintaining an externally identical appearance to the functional EPAP device. Theravent™ (Fig. 2) is FDA cleared for nocturnal use for snoring prevention (Doshi and Westbrook, 2012) but not AMS prevention, thus an investigational device waiver was obtained.
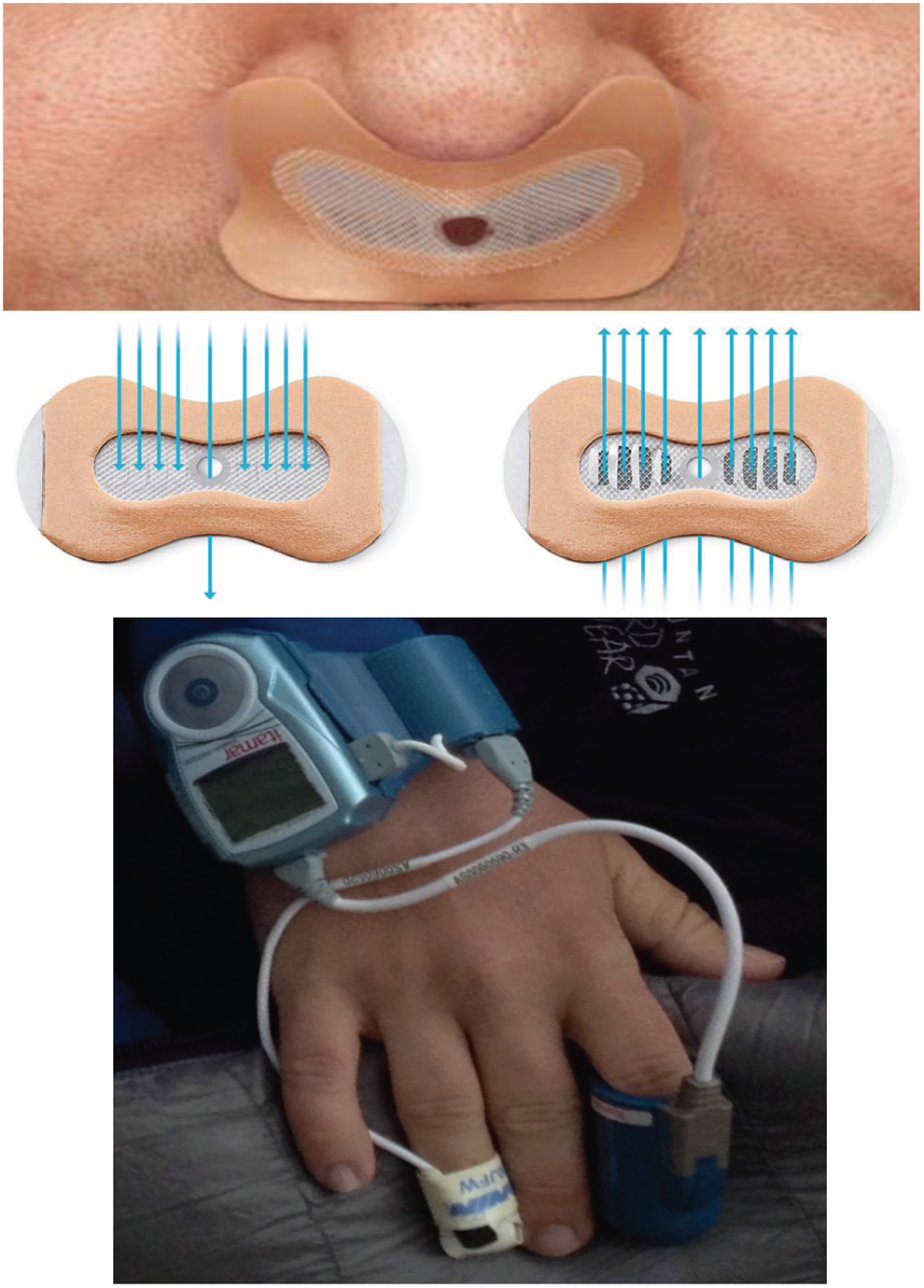
Above: Theravent™ nasal EPAP device. Arrows denote directional air-flow on expiration and inspiration, respectively, EPAP, expiratory positive airway pressure. Below: Watch-PAT200™
Measurement methods
The primary outcome was incidence of acute mountain sickness the morning after enrollment as calculated by the Lake Louise Questionnaire (LLQ) score, a widely used and validated questionnaire used for the quantification of AMS. A diagnosis of AMS requires a score of 3 or greater with the mandatory presence of headache and at least one of the following symptoms: dizziness or lightheadedness, fatigue, GI symptoms (nausea/vomiting), or difficulty sleeping (Roach et al., 1993). Participants were self-evaluated the evening of arrival to the study altitude, and again the following morning after the overnight intervention. The LLQ score for the morning after was used for scoring irrespective of an AMS diagnosis.
Secondary outcome measures included AMS severity by LLQ and objective sleep metric variables: number of desaturations, number of awakenings, average peripheral oxygen saturation (Sp
Watch-PAT200
The Watch-Pat200 is an FDA approved device that replaces a dedicated sleep laboratory with a small, lightweight, comfortable, and portable watch that can be used in a hiker's normal sleeping environment (Fig. 2). It performs physiologic sleep monitoring by gathering sleep data using a pulse oximeter, decibel meter, positional gyroscope, and finger plethysmograph—which computes peripheral arterial tonometry (PAT). This device analyzes continuous oxygen saturation, oxygen desaturation events, pulse, sleep time, and stages (awake, light, deep, and REM sleep) (Herscovici et al., 2007; Bresler et al., 2008). The PAT detects transient vasoconstriction and tachycardic events that correlate pulsatile finger blood flow patterns with standard apnea-hypopnea scoring (Schnall et al., 1999; Lavie et al. 2000; Pillar et al., 2002) to analyze sleep architecture and accurately diagnose sleep conditions (Lavie et al., 2000; Dvir et al., 2002; Penzel et al., 2004).
The Watch-PAT200 was worn while sleeping with four sensors attached: PAT finger probe, peripheral blood oxygenation (Sp
Each morning the devices were collected from participants, and their data extracted and saved to hard drive on a password-protected laptop running Windows XP (Redmond, WA) using Itamar zzzPat software for analysis. The zzzPat software automatically excluded erroneous measurements and identified device and sensor errors; researchers also manually catalogued any device errors or hardware failures. The raw sensor data was copied, each Watch-PAT200 device's memory cleared, and then re-configured for the subsequent study participant.
Primary data analysis
Trekker's AMS incidence at the enrollment sites range from 25% to 38% (Fagenholz et al., 2009; Cushing et al., 2013). For our power analysis, incidence was estimated to be 30%. To achieve 80% power (alpha=0.05) two-tailed test, a sample size of 124 (62 in each arm) would detect a significant difference, defined a priori as a reduction in acute mountain sickness by 20%. Intent-to-treat analyses of univariate comparisons (Pearson chi-square, Fisher's exact tests, t-tests, Wilcoxon rank sum test), and logistic regression were used to examine multivariate risk factors for binary outcomes. P values<0.05 were considered significant and 95% confidence intervals used. All analyses were conducted using computerized software (R 3.1.0 software; Vienna, Austria).
Results
A total 223 participants were enrolled (4 were excluded by criteria) and randomized (Fig. 3), with similar baseline demographics in both groups (Table 1). We performed a modified intention-to-treat approach, where all randomly assigned study participants were analyzed except those not fulfilling inclusion criteria and those who never received the intervention (Fergusson et al., 2002). Additional analyses were performed in the proper use population, defined as those who wore the nasal strip the entire night as a dichotomous outcome—as there were a substantial portion of participants who removed, lost, or had failure of the nasal strip during the night.

Participant flow chart. AMS, acute mountain sickness; EPAP, end expiratory airway pressure; ITT, intent-to-treat.
EPAP, expiratory positive airway pressure.
Of the 219 enrolled, 33 participants used the EPAP device without the Watch-PAT200. These individuals completed symptom questionnaires included in primary and secondary outcome analyses, but did not participate in sleep monitoring. Of the 186 sleep studies, 35 (19%) contained some form of unrecoverable device error. These errors stemmed from issues with disposable sensors and their connections, and in some cases may have been exacerbated by cold sleeping conditions. An additional 23 (12%) measurements were excluded due to unrecoverable human error (e.g., sensor misapplication, premature device removal, or device not turned on). In nine of the incomplete studies due to device or human error, the PAT probe failed to collect data, while the Sp
Primary outcome
The incidence of acute mountain sickness was found to be similar in both the intent-to-treat analysis (14% EPAP vs. 17% placebo, p=0.65; risk difference -3.15%, 95% CI
Secondary outcomes
The mean LLQ scores were not significantly different between the two groups (1.54 EPAP vs. 1.87 placebo, p=0.17). Intent-to-treat analysis showed participants using the EPAP device demonstrated significant decreases in the LLQ subgroup symptoms of headache and dizziness, in both incidence and average score of severity (Table 2). The proper use cohort showed a difference in dizziness alone (data not shown).
AMS, acute mountain sickness; EPAP, expiratory positive airway pressure; IQR, inter-quartile range; LLQ, Lake Louise Questionnaire.
p<0.05. Results are using a two-sample chi-squared test for equality of proportions.
Numbers in bold indicate significant values.
Intent-to-treat analysis found that sleeping with the EPAP device provided statistically significant improvements in several objective sleep metric variables including: average nocturnal oxygenation and percentage of time sleeping below 80% Sp
EPAP, expiratory positive airway pressure; LLQ, Lake Louise Questionnaire; REM, rapid eye movement; SD, standard deviation; SpO2, peripheral oxygen saturation.
results are presented as Median and 1st/3rd inter-quartile range as nonparametric distribution and analyzed by Wilcoxon rank sum test, all other results by t-test, *p<0.05.
Numbers in bold indicate significant values.
Discussion
This was the first double-blind randomized placebo controlled trial to examine expiratory positive airway pressure for prevention of AMS. The intervention was not found to be protective against the development of acute mountain sickness incidence or overall severity. However, those randomized to the EPAP device found significant decreases in both incidence and severity of the AMS subgroup symptoms of headache and dizziness. Headache is a defining characteristic of AMS and overwhelmingly the most common complaint at high altitude (Burtscher et al., 1998; 2011; Hackett and Roach, 2001). High altitude headache is an important health problem in those who travel to high altitude (Burtscher et al., 2011), and the benefit of its prevention should not be underestimated. This headache has been described not only as the predominant symptom in the context of AMS, but also as an isolated occurrence solely due to hypoxia (Serrano-Duenas, 2007). It is reasonable that prevention of nocturnal hypoxia may have led to the prevention of high altitude headache upon awakening.
The EPAP group demonstrated an improvement in sleeping Sp
Sleep at high altitude is affected by periodic breathing. First described in 1898 (Di Giulio and West, 2013), this central form of sleep apnea (CSA) occurs due to a respiratory feedback loop of hypobaric hypoxia induced hyperventilation that alternates with hypocarbia-induced inhibition of the ventilatory drive—and subsequent apneic events. The hypothesis that CSA induced nocturnal hypoxia is a major factor in development of AMS has been debated by some (Eichenberger et al., 1996), but seems biologically intuitive that more frequent hypoxic events and a decreased average nocturnal Sp
The nasal EPAP device was found to significantly improve the average nocturnal peripheral saturation above 80%, as well as substantially decrease the percentage of sleep time below 80% Sp
The sensation of poor sleep at altitude was frequently observed in both groups, with similar numbers of nocturnal awakenings. The observed 66% of overall sleep impairment was similar to prior high altitude sleep studies, where 32%–60% of subjects reported disturbed sleep (Jafarian et al., 2008). Sleep disturbances at high altitude are frequent, and sleep quality has been shown to have the weakest correlation with other AMS symptoms (Macinnis et al., 2013). While sleep time was significantly decreased in the EPAP group, it was difficult to determine if this was due to the discomfort of increased work of breathing with expiratory resistance. Altitude-associated changes in sleep architecture include decreased time spent in the slow wave/deep stages (III and IV) with an increase in the lighter (I and II) sleep stages (Goldenberg et al., 1988; Anholm et al., 1992; Johnson et al., 2010) as well as decreased duration of rapid eye movement (REM) sleep by as much as 50% (Anholm et al., 1992; Mizuno et al., 1993; Wickramasinghe and Anholm, 1999). The EPAP group showed a significant decreases in sleep latency. The improved oxygen saturation may have contributed to a more rapid time to sleep. We found a positive correlation between the percentage of time in deep sleep and average Sp
The studied EPAP device is inexpensive, portable, and convenient—a marked departure from the cumbersome EPAP and electricity dependent PEEP devices that have been examined as nonpharmacologic alternatives for AMS prevention. Nasal EPAP is also more logistically feasible for prevention of nocturnal hypoxia than dead space masks, which have shown to decrease central apnea but not AMS (Patz et al., 2013). The challenge of implementation of the studied device was the level of user discomfort. For some participants, sleeping in the cold environment of high altitude led to an uncomfortable amount of condensation within the nasal cavities. While it may be implied that the expiratory resistance of the EPAP device may have led to greater discomfort, subsequent noncompliance, there was no statistically significant difference in the rate of noncompliance or sleep quality between the two groups.
The observed low incidence of acute mountain sickness was approximately half the rate as previously reported at the same locations (Fagenholz et al., 2009; Cushing et al., 2013). The decrease of AMS at the study enrollment sights followed a similar historical trend recently reported from Manang, Nepal (McDevitt et al., 2014). Re-calculating a power analysis with an effect size of 10% reduction of disease using our observed incidence of AMS would have result in a study enrollment goal of 368 participants, which was potentially unfeasible. Although we exceeded our power analysis of 124 by 95 randomized participants, we may not have been able to find efficacy of the intervention due to the previously undocumented low incidence of disease at our enrollment sites. This decrease in AMS incidence could have been attributed to increased educational efforts, more conservative ascent profiles, increased use of acclimatization medications, or better recognition and treatment of AMS symptoms prior to further ascent.
Although there appeared to be substantial benefits to the nasal EPAP device, there was some difficulty in correct usage, as only 54% indicated they used the strip continuously throughout the night. The most common reported reasons for noncompliance were: discomfort with the strip over the nares, feeling of breathlessness, condensation buildup inside the nasal strip, feeling of dry mouth or mouth-breathing, or failure of the strip adhesive. Implementation of the EPAP device to the high altitude milieu may require low altitude practice and familiarity prior to adoption and utilization that may potentially improve compliance and benefit.
On account of the high numbers of partial or noncompliance, we analyzed the data in two ways: proper use and intent-to-treat analysis. Thus we could address any differences in trends that were noted between groups and be as concise as possible with data interpretation. We considered noncompliance as a dichotomous outcome, as we were unable to quantify the amount of partial use. Therefore, the intent-to-treat analysis is likely most reflective of the actual affect of the nasal EPAP device, as it included a fair amount of partial implementation that may have conferred physiologic benefit.
While some study participants may have been able to determine their randomization group by inspecting the device closely, this bias is unlikely to have occurred as 54% of participants correctly guessed their intervention group the following morning.
Conclusion
This randomized placebo controlled trial found that an inexpensive and disposable nasal EPAP device did not prevent acute mountain sickness, but did decrease the incidence and severity of headache and dizziness while improving nocturnal oxygen saturation and limiting the percentage of desaturations. Further studies of nocturnal EPAP devices are warranted to further explore this adjunct for potential AMS prevention.
Footnotes
Acknowledgments
The authors graciously acknowledge Drs. Buddha Basnyat and Ken Zafren for their assistance with the Nepali Health Research Council and on-site implementation, the Himalayan Rescue Association for their encouragement of scientific endeavors, the Wilderness Medical Society for their Research Grant, Itamar Medical and Ventus Medical for material support, and the trekkers, as without them the study would not have been possible.
Author Disclosure Statement
No conflicting financial interests exist.