
Abstract
Abstract
Dehnert, Christoph, Derliz Mereles, Sebastian Greiner, Dagmar Albers, Fabian Scheurlen, Stefanie Zügel, Thomas Böhm, Peter Vock, Marco Maggiorini, Ekkehard Grünig, and Peter Bärtsch. Exaggerated hypoxic pulmonary vasoconstriction without susceptibility to high altitude pulmonary edema. High Alt Med Biol 16:11–17, 2015.—
Methods and Results:
We screened 421 healthy Caucasians naïve to high altitude for HPV using Doppler echocardiography for assessment of systolic PAP in normobaric hypoxia (PASPHx; P
Conclusion:
An exaggerated HPV cannot be considered a surrogate maker for HAPE-susceptibility although excessively elevated PAP is a hallmark in HAPE, while a normal HPV appears to protect from HAPE in this study.
Introduction
H
HAPE-susceptible individuals (HAPE-S) are characterized by an exaggerated HPV, which was demonstrated by catheterization (Hultgren et al., 1971; Fasules et al., 1985) or by Doppler echocardiography (Grünig et al., 2000a; Dehnert et al., 2005) during brief exposures to hypoxia not leading to pulmonary edema. These retrospective investigations performed by Doppler echocardiography showed that a cut off value of 40 mmHg for PASP after a 2-hour exposure to normobaric hypoxia corresponding to an altitude of 4500 m, and during exercise in normoxia separated HAPE-S from nonsusceptibles with almost no overlap (Grünig et al., 2000a; Dehnert et al., 2005). Recently, Grünig et al. (2009) reported that about 10% of a healthy Caucasian population has a PASP increase above 43 mmHg with an identical hypoxic exposure. Based on the above-mentioned data, we hypothesized that these individuals are susceptible to HAPE.
To test this hypothesis we screened Caucasians who had never been to high altitude before and ascended rapidly to 4559 m with individuals showing a pulmonary artery systolic pressure (PASP) in hypoxia clearly above 40 mmHg and matched controls with normal HPV. We postulated that 60%–70% of those with exaggerated HPV would develop HAPE, while HAPE would not occur among controls.
Methods
Study protocol and study population
The study was performed according to the Declaration of Helsinki and its current amendments. The study protocol was registered at ClinicalTrials.gov under the number NCT00559442 (http://clinicaltrials.gov/show/NCT00559442) and was approved by the Ethics Committee of the Medical Faculty of the University of Heidelberg, Germany. All subjects had given written informed consent prior to the study.
The first part of the study was a screening performed in Heidelberg, at an altitude of 100 m to identify subjects with increased PASP in normobaric hypoxia (FI
Subjects for the screening in Heidelberg were recruited by advertising in the local press, on our institutional home page, and in the journal and homepage of the German Alpine Club. From the applicants we recruited 421 healthy individuals between 18–55 years who had never slept above 3500 m, were not going to stay above 2000 m during the 4 weeks preceding the field study, and had no family history of pulmonary hypertension.
Screening for abnormal hypoxic pulmonary vasoconstriction (HPV)
Screening was performed in two adjacent, directly connected hypoxic rooms at an FI
This second examination in Heidelberg concurrently was used for assessment of baseline values in the subjects selected for the field study. At this examination PASP was also measured by echocardiography during exercise in normoxia, which was not part of the screening procedure. Additionally ECG, pulmonary function testing, and chest radiographs were performed.
33 of the 39 HPV+-subjects were able to take part in the altitude study leaving 24 places for control-subjects. Subjects characteristics are displayed in Table 1. A history of maternal preeclampsia (Jayet et al., 2010), perinatal hypoxemia (Sartori et al., 1999), and a family history of pulmonary hypertension (Grünig et al., 2000b) were excluded in all subjects.
Age, body weight, height, heart rate (HR), oxygen saturation (Sa
Altitude study
Groups of four including randomly HPV+- and control-subjects ascended within 22 hours from Alagna, Italy (1200 m) to the Margherita hut (4559 m) with one overnight stay at the Gnifetti hut (3611 m). The ascent was identical with that of previous studies (Oelz et al., 1989; Bärtsch et al., 1991; Scherrer et al., 1996; Maggiorini et al., 2001; 2006; Sartori et al., 2002; Swenson et al., 2002), except for a 1 hour longer hike on day one. Groups were lead by a mountain guide and accompanied by a physician or a senior medical student trained in altitude medicine.
At 4559 m, clinical examination, AMS scores, pulse oximetry (MasimoSet Radical, Masimo Corp., Irvine, CA, USA), capillary blood gas analysis (ABL5, Radiometer, Copenhagen, Denmark), and Doppler echocardiography were performed about 6 hours after arrival (M1) and in the following 2 mornings (M2 and M3). If signs of HAPE occurred, all these examinations were repeated and a chest x-ray was performed, followed by treatment with pulmonary vasodilators and oxygen. If no signs of HAPE had occurred during the 48-hour stay at 4559 m, the chest x-ray was performed immediately before descent. In cases of AMS, a symptomatic therapy with NSAIDs, and if necessary anti-emetics, was offered to the subjects. Five severe cases were treated with dexamethasone: one control subject after the measurements at M1and two subjects of each group after the measurements at M2.
Determination of pulmonary artery systolic pressure
Identical to previous studies PASP was determined with conventional echocardiographic equipment. During the screening study echocardiographic recordings were obtained with an Aloka SSD 2200 ultrasound machine (Aloka, Tokyo, Japan) and 2.5 MHz duplex transducer. Measurements during the second visit and at high altitude were obtained by a GE Vivid-i ultrasound machine (GE-Healthcare, Fairfield, CT, USA) and compatible duplex transducer (1,5–3,6 MHz; GE3S, GE-Healthcare).
Measurements at base line included a stress-Doppler-echocardiography on a bicycle ergometer, and data will be reported in a separate publication. For PASP determination, peak-flow velocities of tricuspid valve regurgitation jets were measured at the highest coherent boundary of the spectral wave using continuous-wave Doppler, guided by color-flow Doppler. Right atrial to right ventricular pressure gradient was calculated from a modified Bernoulli equation (Alleman et al., 2000). For calculation of PASP, 5 mmHg were added for the estimated right atrial pressure (Gurtner et al., 1975).
One experienced cardiac sonographer assessed all recordings. During the screening study a second experienced cardiac sonographer judged the validity of PASP values independently from printouts of at least three heart cycles immediately after the measurement. In case of disagreement measurements were repeated immediately. Values accepted at screening are means of at least three valid measurements. This procedure was also applied for PASP assessments during the second hypoxic exposure, since an instant decision regarding the inclusion in the altitude study, followed by further base line examinations, was necessary for logistic reasons. Additionally, all PASP measurements obtained at this second visit and throughout the altitude study were digitally recorded (EchoPAC, GE Healthcare) and evaluated offline in random order after the study by a third experienced sonographer blinded to clinical and experimental data. All values reported from baseline and altitude are means of three different heart cycles from the off-line evaluation. Agreement between the online and the off-line examiner was excellent as indicated by mean differences of only 2.5–2.8 mmHg with r2 values of 0.82–0.91 at the various time points of examination.
Diagnosis of HAPE
The diagnosis of HAPE was based on chest radiography, as previously described (Vock et al., 1989), using a transportable radiographic system (Siemens TRS, Siemens, Stockholm, Sweden) with a fixed target-to-film distance of 1.40 m at 95 kV and a tube current of 3–6 mAs. In two subjects, diagnosis of HAPE was made on the basis of clinical findings only, because in one case, HAPE developed already at the Gnifetti hut where no study equipment was available, and in the other case the x-ray machine was not operational due to a technical defect. In both cases the clinical signs were unambiguous. Chest x-rays were digitally recorded and analyzed after the study in random order by an experienced radiologist not involved in the field study and blinded to the clinical and experimental data identically to previous studies (Vock et al., 1989).
Statistics
The power analysis based on historical data (Bärtsch et al., 2002) indicated that 30 subjects with abnormal HPV are sufficient to show a 20% relative difference of the incidence to the historical controls with a statistical power of 0.80 at a level of significance of 0.05. Since the HAPE group consisted of only 4 subjects with several missing values in two of them, we did not include this group in the statistical analysis. Therefore, for comparison between HPV+-subjects without HAPE and control subjects, a two-way ANOVA was used, post hoc testing was performed using a paired t-test for the effect of time and an unpaired t-test for the effect of group. A p-value of 0.05 was considered significant. Statistical analyses were performed using the SigmaStat software–package (SPSS, Inc., Chicago, IL, USA).
Results
Prevalence of abnormal HPV at low altitude
Altogether 421 subjects (117 women) were included in the screening part of the study (Fig. 1). Four subjects refused to finish the 2-hour stay in the hypoxic room because they felt uncomfortable without specific symptoms. Data were not collected in these subjects. A reliable determination of PASP was not possible in 16 (3.8%) subjects due to insufficient tricuspid valve regurgitation jets. Distribution of PASP in all subjects is shown in Figure 2. PASP values above 40 mmHg were measured in 65 (15.6%) subjects, in 39 (9.4%) values were above 44 mmHg. The distribution of HPV was not different between gender (p=0.81) and there was no correlation with age (r2=0.059) or BMI (r2=0.013).

Flow chart of the screening for identification of subjects with an abnormal HPV and their incidence of HAPE. Out of 421 subjects screened, 39 were identified with a PASP ≥45 mmHg. 33 of them ascended to the Margherita hut; 3however, turned back for non-medical reasons, one further subject had to descend due to HAPE at 3611 m. From the remainder 29, 3 developed HAPE. Altogether 4 (13%) cases of HAPE occurred.
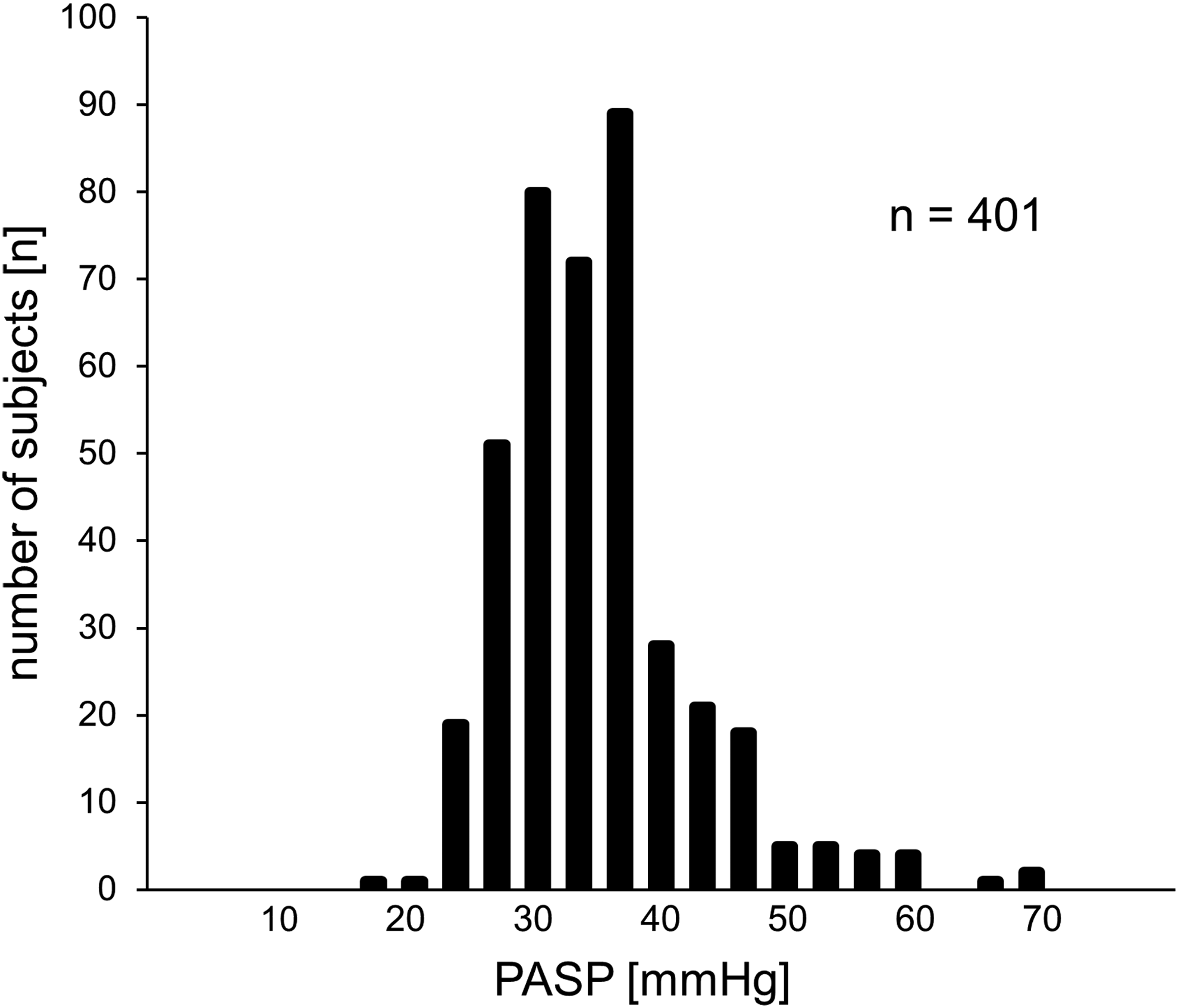
Distribution of PASP values from screening measurements grouped by 3 mmHg.
The difference of PASP between the first and the second measurement at low altitude in those 74 subjects who were considered eligible for participation in the altitude study was small (3.2±2.2, range 0–8 mmHg). Two values were below the cut-off in the HPV+-group. and three above the cut-off values in the control group in the second measurement, resulting in the exclusion of these individuals. The offline evaluation performed after termination of the altitude study confirmed these results with regard to the predefined cut-off values except for one control subject (PASP 41 mmHg) and five HPV+-subjects (PASP 44–42 mmHg).
High altitude study
Mean PASP values measured at high altitude did not differ significantly from those measured at low altitude in normobaric hypoxia (Table 2). The time course of individual values is shown in Figure 3. In those eight HPV+-subjects, in whom PASP was measured ≤44 mmHg at least once at 4559 m, the average PASP at high altitude was 43.0±5.8 mmHg. In the seven control subjects, in whom PASP was measured ≥38 mmHg at least one time at 4559 m, the average PASP at high altitude was 40.6±3.0 mmHg. In all other subjects, PASP stayed above (HPV+) or below (controls) the predefined cut-off values in all measurements at high altitude.
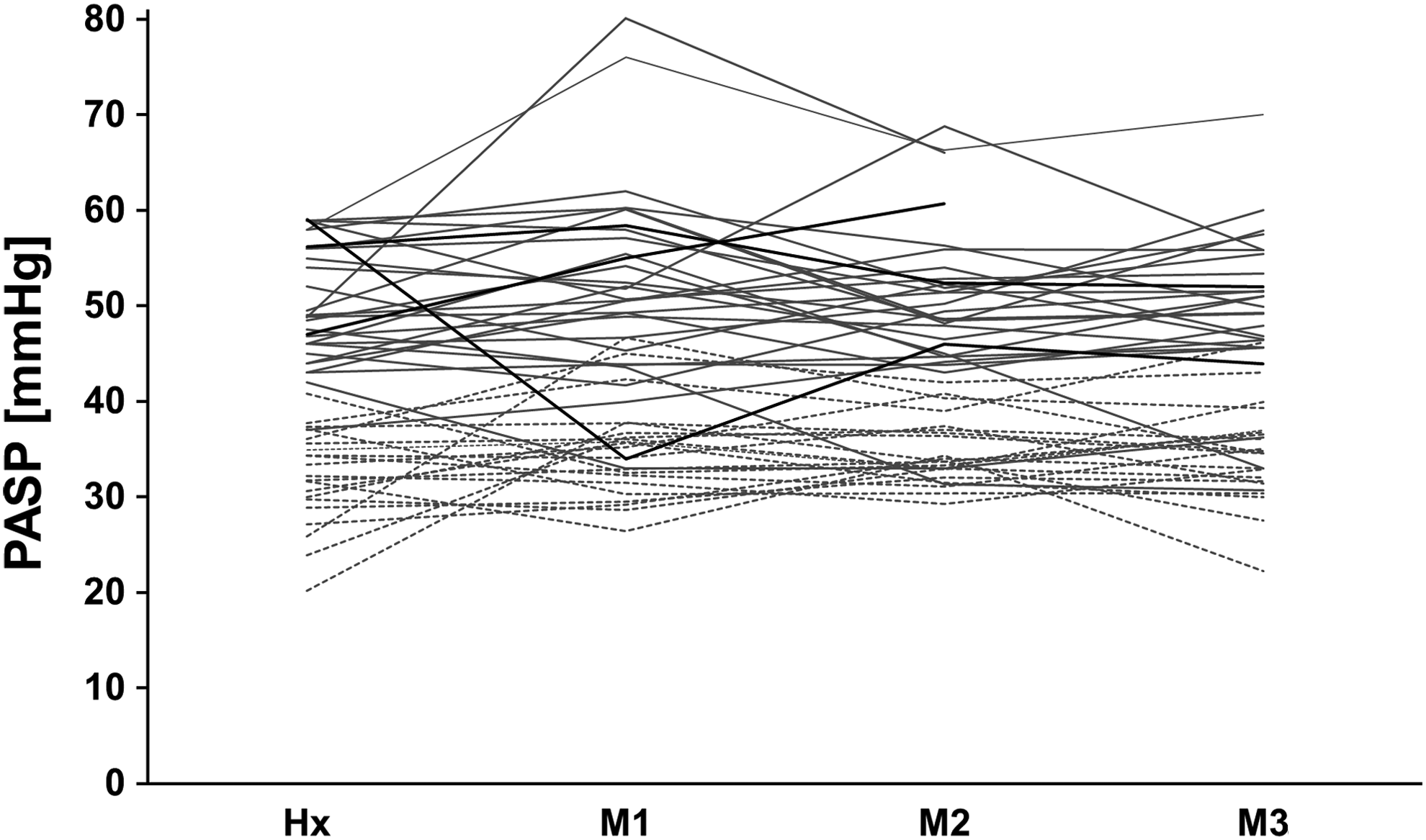
Individual course of systolic pulmonary artery pressures (PASP) measured after 2 hours exposure in normobaric hypoxia (Fi
Oxygen saturation (Sp
Values are based on three subjects except at Hx and M3. At Hx n=4 due to inclusion of the subject who developed HAPE already at 3611 m, at M3 n=2 due to drop out of the two subjects who developed HAPE before M3.
significant differences between groups, †significant difference to normobaric hypoxia and/or over time at altitude, respectively (one symbol p<0.05, two symbols p<0.01, three symbols p<0.001).
Altogether 24 control subjects and 33 HPV+ subjects were included in the field study (Fig. 1). Three subjects of the HPV+-group turned back during the ascent from Gnifetti hut to Margherita hut at an altitude of about 3900 m for non-medical reasons. In one subject of the HPV+-group, HAPE was diagnosed by the accompanying experienced senior physician already at the Gnifetti hut. Further examinations were not possible at this location and this subject had to descend. In three of the 29 subjects of the HPV+-group who stayed for 48 hours at 4559 m, HAPE was diagnosed clinically and could be confirmed by chest radiography in two cases. In the third case, radiographic documentation was not possible due to a temporary damage of the equipment. The clinical presentation with rales, dyspnea, and orthopnea, Pa
PASP was not different between the HPV+-subjects without and with HAPE, while Pa
Changes of blood pressure and heart rate were not different between groups. Systolic blood pressure at 4559 m increased maximally on M3 to 136±11 and 130±12 mmHg and resting heart rate increased maximally on M1 to 88±13 and 84±11 min−1 in HPV+ and controls, respectively. Diastolic blood pressure did not change significantly between low and high altitude.
No control subject developed clinical symptoms or signs of HAPE nor unequivocal radiographic evidence of pulmonary edema. Four HPV+- and five control subjects showed questionable interstitial edema in at least one quadrant of the lungs at the offline evaluation of the chest radiographs. None of these subjects had, however, clinical symptoms of HAPE or impaired gas exchange. Thus, applying the same criteria for the diagnosis of HAPE that were used in all previous studies (Vock et al., 1989), we calculated an incidence of HAPE 13% (4 out of 30) for individuals with PASP above 45 mmHg after breathing 12% O2 for 2 hours at low altitude, while the incidence is 0% when PASP with such testing was below 38 mmHg.
Discussion
An increased PASP above 45 mmHg in hypoxia equivalent to an altitude of 4500 m was associated with a HAPE-incidence of 13% only, whereas HAPE-S, characterized by a comparably increased HPV, had a 60%–70% recurrence rate in several previous studies (Bärtsch et al., 1991; Scherrer et al., 1996; Maggiorini et al., 2001; 2006; Sartori et al., 2002; Swenson et al., 2002) in the same location with identical ascent rates. These data indicate that factors in addition to an exaggerate increase of PAP are needed to produce HAPE. The study suggests furthermore that HAPE has a very low probability to occur after rapid ascent to 4559 m in non-acclimatized individuals when PASP at 12% oxygen is below 38 mmHg.
Measuring PAP after 2-hour exposure to normobaric hypoxia (FI
The HPV+-subjects selected for this study also show similar abnormally elevated PASP in response to exercise in normoxia (data will be reported separately) as it was found in HAPE-S in previous studies (Grünig et al., 2000a; Dehnert et al., 2005). Several investigations performed with HAPE-S at the same place with identical ascent rates have demonstrated the association of HAPE with abnormally high PASP and found a recurrence rate of 60%–70% (Bärtsch et al., 1991; Scherrer et al., 1996; Maggiorini et al., 2001; 2006; Sartori et al., 2002; Swenson et al., 2002). Despite an identical altitude exposure and despite using the same diagnostic criteria (Vock et al., 1989) as in the studies mentioned above, we found that only 13% of the individuals with an exaggerated HPV and none of the subjects with a normal HPV developed HAPE.
Our findings indicate that an exaggerated HPV cannot be considered a reliable maker of HAPE susceptibility and that it cannot be taken as a surrogate marker for predicting HAPE susceptibility in individuals with no previous altitude exposure (Bärtsch and Swenson, 2013). A “normal” HPV, however, appears to protect from HAPE in non-acclimatized mountaineers ascending rapidly to 4559 m. Given the low incidence of HAPE of about 6% among controls of previous studies in the same setting (Bärtsch et al., 2002), the number of subjects with normal HPV in the present study is, however, too small to draw a firm conclusion in this respect.
The absence of HAPE with normal HPV in this study, high PAP consistently found in HAPE-S, a recurrence rate of 60%–70% for HAPE-S under identical conditions, and preventing HAPE by lowering PAP all suggest that high PAP is a compulsory factor for developing HAPE. Thus, the low incidence of 13% HAPE in individuals with an exaggerated HPV in this study indicates that factors in addition to an exaggerated rise of PAP at high altitude are necessary for causing HAPE. This conclusion is also supported by the absence of HAPE after an identical ascent in a group of 10 young adults with a history of a transient postnatal hypoxic insult who had abnormally high PASP at 4559 m (Sartori et al., 1999). Our subjects had, however, no history of a perinatal hypoxic insult.
Based on mechanisms discussed in the pathophysiology of HAPE (Bärtsch et al., 2005; Swenson and Bärtsch, 2012), three additional mechanisms might contribute to HAPE susceptibility in addition to exaggerated HPV: 1) The degree of inhomogeneity of pulmonary vasoconstriction: The hypothesis of inhomogeneity of arteriolar vasoconstriction resulting in increased capillary pressure in areas with high blood flow had been suggested by Hultgren (1971) and was subsequently supported by lung perfusion studies by MRI in hypoxia (Hopkins et al., 2005; Dehnert et al., 2006). 2) Hypoxic venous constriction: This has been demonstrated in several animal studies and has been suggested to contribute to increasing pulmonary capillary pressure in men (Maggiorini et al., 2001). Maggiorini et al., using right heart catheterization at 4559 m, found elevated post capillary resistance only in HAPE-S with HAPE but not in HAPE-S without HAPE. 3) An impairment of alveolar fluid clearance: Sartori et al. (2002) presented indirect evidence for a role of deficient epithelia sodium channels in impaired alveolar fluid clearance in HAPE. In addition, we cannot exclude that repeated exposures to high altitude are needed to develop HAPE and that greater resistance of the alveolo-capillary barrier is present in those who did not develop HAPE despite exaggerated PASP. The lower Sa
Alternatively, HAPE susceptibility may be linked to particular mechanisms of an exaggerated HPV, since multiple pathways may contribute to such a response (Maggiorini et al., 2014). We can exclude left ventricular diastolic dysfunction as a contributor to elevated PASP because of normal systemic blood pressure and because echocardiographic parameters assessed by pulsed-wave Doppler and tissue Doppler imaging revealed no sings of diastolic dysfunction in any of the subjects (data not shown). We cannot exclude that erroneous or imprecise measurements overestimating PASP by echocardiography contributes to the low incidence of HAPE among HPV+-subjects. However, all measurements were checked offline by a second examiner blinded to the clinical data and agreement between the two examiners was excellent as reported in the method section.
Furthermore, estimation of PASP by echocardiography is easier to perform in hypoxia because of more pronounced tricuspid regurgitation jets with higher PASP. A previous study showed an excellent agreement between measurements of PASP by echocardiography and right heart catheter at the Margherita hut (Alleman et al., 2000). Finally, the fact that assessment of PASP by echocardiography on three occasions at 4559 m and after 2 hours of an equivalent–although normobaric–hypoxia yielded comparable results (Fig. 2) shows the consistency of the measurements performed in this study and indicates that PASP at high altitude can be predicted by measurement of HPV at comparable level of hypoxia at low altitude.
Under the very unlikely assumption that the six HPV+-subjects who did not participate, the three HPV+-subjects who did not reach the Margherita hut, and the two subjects of the HPV+-group who were treated with dexamethasone would all have developed HAPE, the incidence were still only 38% (15 of 39 subjects) which is slightly more than half the value expected. Thus we can exclude that a sampling error accounts for the negative result of this study with regard to HPV+ being a reliable indicator of susceptibility to HAPE.
Based on the observed incidence of HAPE, the positive predictive value for PASP >45 mmHg at an FI
Footnotes
Acknowledgments
The authors thank the study participants and mountain guides, the hut keepers, and the Sezione Varallo of the Club Alpino Italiano for providing an excellent research facility at the Capanna Regina Margherita and Capanna Gnifetti and Martina Haselmayr and Birgit Schneiders (Div of Sports Medicine, University Hospital, Heidelberg, Germany) for their assistance during the examinations and training, and Dipl. Ing. E. Menold (Div of Sports Medicine, University Hospital, Heidelberg, Germany) for technical support throughout the study.
Author Disclosure Statement
PB received lecture fees from Bayer Pharma AG, GlaxoSmithKline GmbH & Co. KG and MSD Sharp & Dohme GmbH, and financial support from the Linde Group for organizing a scientific meeting. All other authors have nothing to disclose.