
Abstract
Abstract
Lochner, Piergiorgio, Marika Falla, Francesco Brigo, Michael Pohl, and Giacomo Strapazzon. Ultrasonography of the optic nerve sheath diameter for diagnosis and monitoring of acute mountain sickness: A systematic review. High Alt Med Biol. 16:195–203, 2015.—
Methods:
Systematic search of MEDLINE (through Pubmed; from 1966 to 14 October 2014), Cochrane Central Register of Controlled Trials (CENTRAL), and EMBASE databases.
Results:
Six studies with 436 subjects (139 women, 297 men; 406 mostly Caucasian; 30 Nepalese) were included. A marked variability in ONSD was found across studies both at baseline and at high altitude.
Conclusion:
The variability in ONSD across the included studies and within each study limit the utility of ONSD measurement in the diagnosis of AMS. ONSD measurements might be useful from a population perspective, but the accuracy of optic nerve ultrasonography for single subjects and single point-in-time assessment for diagnosing AMS is questionable due to high individual variability in ONSD.
Introduction
L
The proposed mechanisms underlying the pathophysiology of AMS—vasogenic vs. cytotoxic cerebral edema, increased cerebral inflow vs. decreased outflow, and impaired integrity of the blood–brain barrier due to vascular endothelial growth factor or reactive oxygen species—are still debated. Most of the gold standard techniques to investigate central nervous system (CNS) changes at high altitude cannot be performed in the field for practical issues, for example, invasive intracranial pressure (ICP) monitoring (via an intraventricular or intraparenchymal catheter with a microtransducer system), computed tomography (CT), or magnetic resonance imaging (MRI). This limitation makes it difficult to investigate the pathophysiology of AMS.
Currently the diagnosis of AMS relies exclusively on subjective reporting of symptoms by the patients (i.e., the Lake Louise Score, LLS) (Bartsch and Swenson, 2013), and does not require any additional neuroimaging technique either in the field or in the hospital to support the diagnosis. A neuroimaging technique able to provide objective measurements at high altitude would enable the collection of empirical data that could be used to refine the LLS or elucidate the pathophysiology of AMS.
Portable ultrasound devices allow noninvasive evaluation of many physiologic parameters of interest during high altitude research (Fagenholz et al., 2012). Ultrasonography of the optic nerve sheath diameter (ONSD) is not only a reliable tool for diagnosis of increased intracranial pressure (ICP) in hospitalized neurocritical patients (Rajajee et al., 2012), but is a promising tool for diagnosis and monitoring of AMS (Sutherland et al., 2008; Fagenholz et al., 2009; Strapazzon et al., 2014). The first studies by Fagenholz et al. (2007; 2009) were pivotal for research on CNS changes at high altitude. Though recent reviews have discussed the pathophysiological changes in the CNS after exposure to hypobaric and normobaric hypoxia (Willmann et al., 2014; Wilson et al., 2014), none have systematically discussed the pathophysiological and clinical significance of increased ONSD.
The aim of this review was to elucidate whether 1. measurements of ONSD could shed light on the pathophysiology of AMS, and 2. ultrasonography of the ONSD could support the diagnosis of AMS. Specifically, we aimed to evaluate the magnitude of changes in ONSD after high altitude exposure and to correlate these changes with AMS.
Technical and safety issues of ONSD ultrasonography
Ultrasonography of the ONSD can be easily performed in B-mode using several ultrasound systems equipped with high-frequency linear probes with ≥7.5 MHz and lateral spatial resolution <0.4 mm. All parameters should be adjusted to achieve the best image quality, including time gain compensation, gray scale, depth, and gain. High mechanical and thermal indexes can damage sensitive structures such as the lens, retina, and vitreous body through formation of gas bubbles due to high negative pressure and heating of tissue; thus, they should be reduced to 0.23 (mechanical index) and 0.0 (thermal index). The settings should be in accordance with the “as low as reasonably achievable” (ALARA) principle and the time of the examination should be kept as short as possible (i.e., between 3 and 5 minutes) (Barnett et al., 2000; Fagenholz et al., 2012).
The examination is usually performed through a transorbital approach with the subject in supine position and the upper part of the body and head elevated about 20–30° to avoid pressure on the eye. A thick layer of gel is applied on the upper closed eyelid and the transducer is positioned on the temporal side. The patient is asked to look straight forward with the eye closed to reduce eye movements and to obtain better delineation of the anatomical landmarks (i.e., the optic nerve and the lens) (Helmke and Hansen, 1996a; Bauerle et al., 2012; 2013).
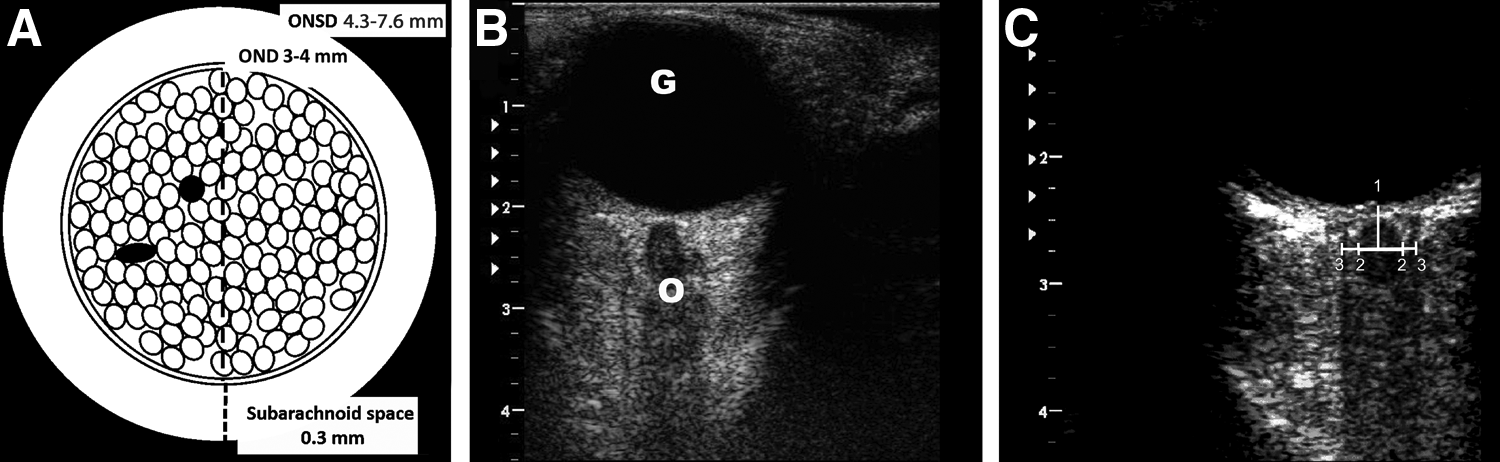
The globe is the main structure and its appearance is homogeneously anechoic, whereas the lens is a small hyperechoic line that divides the globe into the anterior and posterior chambers. The anterior part of the optic nerve can be seen posterior to the globe using an axial plane (Fig. 1). Hypoechogenic optic nerve fibers are surrounded by the echogenic pia mater; the subarachnoid space appears hypoechogenic and is surrounded by the hyperechogenic dura mater (Fig. 1). ONSD should be measured 3 mm behind the globe in each eye (Hansen and Helmke, 1996; Helmke and Hansen, 1996a; 1996b), perpendicularly to the optic nerve axis (Fig. 1). The optic nerve diameter is the distance inside the pia mater; ONSD is the distance inside the dura mater (Fig. 1). Shadowing artifact caused by the lens, optic disc, lamina cribrosa, or poor technique may significantly alter measurements of the ONSD (Copetti and Cattarossi, 2009). Thus, it is mandatory to standardize the examination technique (Ballantyne et al., 2002) and an average of three measurements should be obtained to reduce intra-observer variability (Bauerle et al., 2012; 2013).
In 40 healthy Caucasian subjects, mean ONSD was 5.4±0.6 mm with high inter-individual variation (from 4.3 to 7.6 mm) (Bauerle et al., 2012); acceptable agreement was found between ONSD measured by means of ultrasound and MRI (mean difference <5%), with good inter- and intra-observer reliability (Bauerle et al., 2013).
Material and Methods
This systematic review followed the structured guideline PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) (Moher et al., 2009). An extensive literature search was performed using electronic databases and manual searching. The MEDLINE (through Pubmed; from 1966 to 14 October 2014), Cochrane Central Register of Controlled Trials (CENTRAL), and EMBASE databases were searched. No language restrictions were applied. We used the following search strategy: (“altitude sickness”[MeSH Terms] OR “altitude sickness”[All Fields] OR “altitude illness”[All Fields] OR (“altitude”[All Fields] AND “sickness”[All Fields]) OR (“altitude”[All Fields] AND “illness”[All Fields]) OR (“mountain”[All Fields] AND “sickness”[All Fields]) OR “mountain sickness”[All Fields]) AND (“ultrasonography”[All Fields] OR “ultrasonography”[MeSH Terms] OR “ultrasonography”[Subheading] OR “ultrasound”[All Fields] OR “ultrasonics”[MeSH Terms] OR “ultrasonics” [All Fields] OR “ONSD” [All Fields] OR “optic nerve”[All Fields] OR “intracranial pressure”[All Fields] OR ultrasonogr* OR ultraso* OR “intracranial hypertension” OR “cerebral hypertension” OR “Intracranial Hypertension”[Mesh]).
We included studies performed on adults (subjects aged ≥18 years) and reporting ultrasonographic data for ONSD in patients with AMS compared with subjects without AMS, or studies reporting ONSD both at baseline (before ascent) and after exposure to high altitude in subjects with/without AMS. Only full-length published articles (not personal communications or abstracts) were considered eligible for inclusion. Two authors (PL, MP) independently screened all titles and abstracts identified by the searches to assess eligibility. Following screening, we manually reviewed the articles for potentially eligible citations for inclusion. We reviewed the reference lists of the articles retrieved by the electronic searches to check for other relevant reports not indexed in the electronic databases.
Selected articles were assessed by the same two authors (PL, MP) and the following data were independently extracted and cross-checked: author, sample size (and number of subjects with/without AMS), sex, inclusion criteria and definition of AMS, other altitude illnesses, study design, ascent time, exercise during ascent, altitude and time interval of ONSD measurements, characteristics of the ultrasound device, image acquisition technique, number of investigators involved in performing ultrasonography, blinding to AMS diagnosis, inter-observer and intra-agreement (if assessed), and ONSD at baseline and at high altitude in subjects with and without AMS.
To compare results across studies, ONSD values (mean, standard deviation, range, 95% confidence intervals [CI]) measured at approximately 24 hours and at around 4000 m altitude were extracted. Considering that eligible studies were not designed as diagnostic accuracy studies, we did not use the standardized tool QUADAS (Quality Assessment of Diagnostic Accuracy Studies) (Whiting et al., 2011) to evaluate their methodological quality, but assessed it narratively. In case of disagreement, the two authors reached a consensus through discussion or by consulting a third author (FB).
We calculated the 95% CI for ONSD measured at baseline and in patients with/without AMS for studies not reporting this information. 95% CI were calculated from range values using the d2 (distribution of Average Range) table (Ramírez et al., 2012). We combined ONSD measures from each study to obtain summary estimates in a meta-analysis (if methodologically appropriate).
Results
The initial search retrieved 196 articles. After removing duplicates and reading abstracts and titles, 17 articles were selected for full reading. Six articles (including one study conducted in subjects with high altitude headache; Lawley et al., 2012) were included (Fagenholz et al. 2007; 2009; Sutherland et al., 2008; Lawley et al., 2012; Keyes et al., 2013; Strapazzon et al., 2014) (Fig. 2). A list of the 11 excluded articles is reported as supplementary material in Appendix 1 (supplementary material is available online at www.liebertpub.com/ham). The characteristics of the six eligible studies are summarized in Table 1. The studies differed in ascent time, confounding factors (e.g., exercise), altitude, and interval measurement. This marked clinical and methodological heterogeneity across studies and the lack of single patient information limited the possibility to make a meta-analysis. Hence, we summarized results narratively.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) for reference searches.
AMS, acute mountain sickness; h, hour; HACE, high altitude cerebral edema; HAH, high altitude headache; HAPE, high altitude pulmonary edema; LLS, Lake Louise Score; m, meter; Mhz, megahertz; US, ultrasound; mm, millimeter; NA, not available; ONSD, optic nerve sheath diameter; SD, standard deviation; US, ultrasonography.
The study conducted by Lawley et al., (2012) was a randomized controlled trial assessing the effect of acetazolamide on ONSD in subjects with high altitude headache (in this trial ONSD was assessed longitudinally).
The studies were published between 2007 and 2014 and included a total of 436 subjects (139 women, 297 men; 406 mostly Caucasian; 30 Nepalese). Of note, data from 324 of the 436 subjects were derived from two large cross-sectional studies conducted by the same group of authors (Fagenholz et al., 2007; 2009). Three studies were longitudinal (Sutherland et al., 2008; Keyes et al., 2013; Strapazzon et al., 2014), one study was cross-sectional (Fagenholz et al., 2007), one study was both longitudinal and cross-sectional (Fagenholz et al., 2009), and one study was a randomized controlled trial assessing the effect of acetazolamide on ONSD in subjects with high altitude headache (in this trial ONSD was assessed longitudinally) (Lawley et al., 2012).
109 (25%) of 436 subjects had AMS defined as LLS ≥3, and four studies included patients with other high altitude illnesses (i.e., high altitude cerebral edema, high altitude headache, and high altitude pulmonary edema) (Fagenholz et al., 2007; Sutherland, 2008; Lawley et al., 2012; Strapazzon et al., 2014).
Ultrasonography of ONSD was examined by the same investigator in all studies with the exception of two (Fagenholz et al., 2009; Keyes et al., 2013). Subjects were examined in a supine position obtaining an axial plane showing the optic nerve in its longitudinal course with two main different approaches: positioning the linear transducer either (i) over the temporal upper eyelid (Lawley et al., 2012; Strapazzon et al., 2014) or (ii) transverse over the eye (Fagenholz et al., 2007; 2009; Sutherland et al., 2008; Keyes et al., 2013), and further specifying the visualization of the posterior lens (Sutherland et al., 2008; Keyes et al., 2013). The measurements were taken 3 mm behind the globe in all studies, but the criteria to define ONSD were not clearly defined.
One study did not report whether ultrasound investigators were blind to the clinical diagnosis of AMS (Lawley et al., 2012). The inter-observer agreement was reported in three studies (Fagenholz et al., 2007; 2009; Strapazzon et al., 2014) and the intra-observer agreement in one (Lawley et al., 2012).
Baseline measurements differed mainly in relation to the image acquisition technique: transducer positioned transverse over the eye (Sutherland et al., 2008; Keyes et al., 2013) or over the temporal upper eyelid (Lawley et al., 2012; Strapazzon et al., 2014). Baseline ONSD showed high inter-individual variability in all studies. Baseline ONSD values were not available for the two cross-sectional studies (Fagenholz et al., 2007; 2009).
Subjects had rapid, acute exposure to high altitude in three studies (Lawley et al., 2012; Keyes et al., 2013; Strapazzon et al., 2014) and gradual ascent (trekking) in three studies (Fagenholz et al., 2007; 2009; Sutherland et al., 2008). ONSD was measured at constant altitude in four studies (Fagenholz et al., 2007; 2009; Lawley et al., 2012; Strapazzon et al., 2014) and at progressively increasing altitude in two studies (Sutherland et al., 2008; Keyes et al., 2013). The time interval between ONSD measurement and altitude exposure was not reported in two studies (Fagenholz et al., 2007; 2009). Increased ONSD was associated with progressively increasing altitude (Sutherland et al., 2008).
ONSD increased rapidly after exposure to altitude (after 3 hours) in all participants in two longitudinal studies in which subjects were exposed to a constant altitude and did not perform exercise (Table 2) (Lawley et al., 2012; Strapazzon et al., 2014). ONSD progressively increased up to 24 hours (Lawley et al., 2012; Strapazzon et al., 2014) and remained enlarged between 72 hours and 8 days after exposure to altitude (Strapazzon et al., 2014). Increased ONSD correlated with decreased peripheral oxygen saturation in two longitudinal studies (32 subjects) (Sutherland et al., 2008; Strapazzon et al. 2014), but not in a larger one (57 subjects) (Keyes et al., 2013).
AMS, acute mountain sickness; CI: confidence intervals; h, hour; m, meter; mm, millimeter; NA, not available; NS, not statistically significant; ONSD, optic nerve sheath diameter; SD, standard deviation; US, ultrasound.
Data on ONSD values of subjects with and without AMS were provided by authors.
Normal values of ONSD in healthy subjects obtained in a hospital study (mean±SD): 5.4±0.6 mm (Bäuerle et al., 2012).
An increase in ONSD at high altitude compared to baseline was not consistently found across studies (Sutherland et al., 2008; Keyes et al., 2013), although ONSD measured at approximately 4000 m were higher among subjects with AMS compared with subjects without AMS (Fagenholz, 2007; Fagenholz, 2009; Keyes, 2013; Strapazzon et al., 2014). However, ONSD measured at baseline and at an altitude of approximately 4000 m showed a marked variability across different studies (Sutherland et al., 2008; Keyes et al., 2013; Lawley et al., 2012; Strapazzon et al., 2014), often with overlapping 95% CI (Table 2).
In some studies increased ONSD was associated both with the development of AMS (Strapazzon et al., 2014) and AMS severity assessed by LLS (Sutherland et al., 2008; Fagenholz et al., 2009).
ONSD was strongly associated with headache in a large (n=287) cross-sectional study (Fagenholz et al., 2009). No association was found between ONSD and high altitude headache in a much smaller longitudinal study specifically designed to assess this aspect (n=23) (Lawley et al., 2012).
Discussion
The available data in the literature show that ONSD ultrasonography can be easily performed to evaluate patients with suspected AMS. However, the marked variability in ONSD across the included studies and within each study greatly limit the diagnostic utility of ONSD measurement. An increase in ONSD at high altitude compared to baseline was not consistently found across studies, although ONSD measured at approximately 4000 m seem to be higher among subjects with AMS.
Results of the included studies provide insights into the pathophysiology of AMS. Data from two large cross-sectional studies show that ONSD values correlate with the presence and severity of AMS, suggesting that an underlying increase in ICP may have a role in the pathogenesis of this disorder (Fagenholz et al., 2007; 2009). Interestingly, the increase in ONSD seems to occur irrespective of exercise (Lawley et al., 2012; Strapazzon et al., 2014) and ONSD changes seem to follow a different time course in patients who later develop AMS compared with the subjects who did not develop AMS (Strapazzon et al., 2014).
Furthermore, one recent study shows that changes in ONSD are detectable early and associated with later development of AMS (Strapazzon et al., 2014); in this study the changes in ONSD were related to exposure to hypobaric hypoxia and to clinical symptoms. However, the pathophysiological basis of this increase in ONSD during exposure to hypobaric hypoxia is not yet fully understood.
Increased intracranial pressure and the pathophysiology of AMS
The role of brain volume and ICP in causing symptoms of AMS is still unclear. Neuroimaging techniques showed that hypoxia may increase cerebral arterial blood flow and venous volume, leading to increased ICP and AMS symptoms due to lower ability to cope with an increase in brain volume (Lawley et al., 2014; Wilson et al., 2014). Using a MRI technique, Lawley et al. (Lawley et al., 2014) showed that gray matter volume and, by extension, brain volume, increased after 10 hours in normobaric hypoxia, thus reducing intracranial compliance. This finding supports the hypothesis that a relative increase in ICP also within the normal range may be responsible for AMS. Invasive ICP monitoring at high altitude has been performed only in a few studies with small sample size and different design and methodology. A rise in lumbar cerebral spinal fluid (CSF) pressure was observed after acute exposure to hypobaric hypoxia (Schaltenbrand, 1933; Singh et al., 1969; Hartig and Hackett, 1992) but not after more gradual ascent (Hartig and Hackett, 1992) or in normobaric hypoxia (Bartsch et al., 2004). Similar results were obtained by the only case-series that telemetrically monitored ICP (Wilson and Milledge, 2008).
Overall, a physiological predisposition (i.e., individual ability to maintain oxygen saturation at altitude, especially during exercise) and/or inter-individual variations in neuroaxis compliance—the brain volume compared to skull volume or spinal cord volume compared to spinal canal (tight-fit hypothesis)—may lead to different AMS susceptibility, explaining why some individuals develop symptoms and others do not.
One study showed differences in ONSD at baseline between patients who later developed AMS and subjects who did not (Strapazzon et al., 2014). This finding highlights the importance of investigating factors affecting ONSD in subjects already at sea level (e.g., factors related to anthropometrics such as brain-to-intracranial space ratio, race and gender, as well as individual characteristics such as genetic predisposition to different pathophysiological mechanisms of AMS). ONSD changed differently in the two groups after altitude exposure, independently of baseline differences (Strapazzon et al., 2014). This difference in ONSD increase after exposure (but also the difference of baseline values between the two groups) might be explained by the tight-fit hypothesis (Ross, 1985; Wilson et al., 2009).
An experimental study investigating ICP with MRI changes in 13 subjects developing mild and moderate AMS (Lawley et al., 2014) provided strong evidence to support the hypothesis that the “random” nature of AMS symptoms is explained by a variable intracranial pressure response to hypoxia. Results of this study suggest that “normobaric hypoxia causes an increase in brain volume that leads to reduced intracranial compliance” (Lawley et al., 2014). Consequently, ICP is elevated in individuals who develop AMS symptoms.
ONSD changes at altitude from an anatomical and technical perspective
Several studies using optic nerve ultrasonography showed increased ONSD in patients with increased ICP due to severe brain injury (Geeraerts et al., 2007; Soldatos et al., 2008), intracranial bleeding (Moretti et al., 2009), or idiopathic intracranial hypertension (Bauerle and Nedelmann, 2011). Moreover, enlargement of the ONSD has been demonstrated in patients with increased ICP in hyperacute (within 6 hours of symptom onset) (Skoloudik et al., 2011), acute (within 48 hours of symptom onset) (Moretti et al., 2009), and subsequent stages (Lochner et al., 2014) of intracranial hemorrhage. Experimental studies showed that variation in ONSD was detectable within minutes of increases in ICP (Helmke and Hansen, 1996b). These observations are explained by the anatomy of optic nerve (the continuity of the meninges and the subarachnoid space surrounding the optic nerve). However, some studies report smaller ONSD values at altitude than in hospitalized patients with increased ICP (Sutherland et al., 2008; Keyes et al., 2013). Differences in parameters such as the interpretation of the anatomy of the optic nerve, the ultrasound equipment, and the time of image acquisition could partially explain these discrepancies.
Only two studies included in this review (Lawley et al., 2012; Strapazzon et al., 2014) reported baseline ONSD comparable to those of healthy Caucasian subjects validated with MRI (Bauerle et al., 2013). It is fundamental to define the optic nerve and the optic nerve sheath correctly on ultrasound images to avoid different interpretations of the anatomy. Interestingly, the studies reporting smaller ONSD values (Sutherland et al., 2008; Keyes et al., 2013) used a slightly different technique (i.e., transducer transverse over the eye with the ultrasonographic beam passing through the posterior lens), suggesting that the different eye position could have affected data acquisition (Copetti and Cattarossi, 2009). Nevertheless, relative changes can be reported regardless of technique as long as the technique is consistent.
One study showed that increases in ONSD were in the range of 10%–30% in mild to moderate AMS (Strapazzon et al., 2014); changes in ONSD were small and in the same range of the transceiver resolution (0.1 mm), indicating that the error of the transducer may be the same magnitude as changes in ONSD. Clinicians and researchers should be aware of this potential problem of sensitivity, despite that the portable devices used in recent studies show high resolution images with acceptable inter- and intra-observer reliability.
The pathophysiology of alterations in ONSD is still unclear. Even in healthy normal subjects, there is high inter-individual variability in ONSD values (4.3–7.6 mm) (Bäuerle et al., 2012) that overlaps the ONSD values described in patients with increased ICP (>20 mmHg) in other studies (Rajajee et al., 2012). In critical care patients, the optimal cut-off of ONSD associated with elevated ICP (>20 mmHg) and the influence of acute fluctuations in ICP is still a matter of debate (Rajajee et al., 2012). Although an increase in ONSD could reflect an overall increase in ICP, concrete conclusions cannot be made. The studies assessing ONSD included in this review showed high inter-study variability already at baseline. Moreover, the studies investigating changes in ONSD longitudinally had small sample size and thus risk underpowered results. Additional studies performed under controlled conditions (e.g., hypo-/normobaric hypoxic chamber) would provide useful data to understand the pathophysiological mechanisms underlying alterations in ONSD in subjects exposed to altitude.
Optic nerve sheath diameter ultrasonography and AMS: implication for clinical decision-making
In-field diagnosis of AMS is based exclusively on an international consensus of subjective, nonspecific, equally-weighted symptoms (i.e., headache, sleep disturbance, fatigue, and dizziness) (Bartsch and Swenson, 2013). Three distinct patterns of symptoms were consistently identified in a recent study (Hall et al., 2014), supporting different pathophysiological mechanisms of AMS following acute ascent to high altitude. One hypothesis is that the different results between studies of ONSD after exposure to hypobaric hypoxia (Lawley et al., 2012; Keyes et al., 2013; Strapazzon et al., 2014) could be due to different pathophysiological mechanisms of AMS.
One study found that ONSD had a positive independent association with four of eight LLS components: headache, dizziness, sleep disturbance, and ataxia (Fagenholz et al., 2009). Future studies may further try to correlate ONSD values with single components of the LLS; this would help to elucidate the complex pathophysiology of AMS and provide more objective support for diagnosis of AMS.
ONSD values should be measured both at baseline and after reaching altitude. A recent study showed that patients who later developed AMS had a more pronounced increase in ONSD, which preceded the diagnosis of AMS symptoms by approximately 15 hours (Strapazzon et al., 2014).
Recent data report a correlation between ONSD and the severity of AMS in a population of 500 subjects acutely exposed to hypobaric hypoxia, suggesting that ONSD might be helpful to predict the progression from AMS to high altitude cerebral edema (Yanamandra et al., 2014), as suggested by previous data (Fagenholz et al., 2009). Thus, ONSD could have clinical utility for early diagnosis and thus inform decisions about therapy and/or evacuation from remote areas. Finally, repeated ONSD measurements may be useful for monitoring the efficacy of the therapeutic interventions; previous studies reported decreases in ONSD after different therapies and disappearance of clinical symptoms (Fagenholz et al., 2007; Keyes et al., 2013).
Conclusions
The degree and rate of increase in ONSD at altitude differs considerably across studies and, interestingly, ONSD values in some of the studies included in the present review are within the range of normal (Keyes et al., 2013). Furthermore, it is possible that the magnitude of increase in ONSD is within the magnitude of error of the transducer (Keyes et al., 2013). The variability in ONSD across the included studies and within each study greatly limit the diagnostic utility of these measurements. ONSD measurements might be useful from a population perspective, but the reliability and accuracy of optic nerve ultrasonography for single subjects and single point-in-time assessment for diagnosing AMS seems more questionable due to high individual variability of ONSD.
Longitudinal studies on a larger cohort, at a range of altitudes and with baseline neuroimaging techniques (e.g., MRI) and evaluation of inter- and intra-observer reproducibility are required to further understand the clinical significance of increased ONSD during exposure to hypobaric hypoxia. However, both technological advances in smaller and portable ultrasound devices (capable of operating for several hours on low-weight rechargeable batteries), as well as the technique itself (nonionizing, repeatable, simple, and fast) are promising reasons to further explore the application of ultrasonography in the field.
Footnotes
Author Disclosure Statement
None of the authors have any conflicting financial interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.