
Abstract
Abstract
Parati, Gianfranco, Juan Eugenio Ochoa, Camilla Torlasco, Paolo Salvi, Carolina Lombardi, and Grzegorz Bilo. Aging, high altitude, and blood pressure: A complex relationship. High Alt Biol Med 16:97–109, 2015.—Both aging and high altitude exposure may induce important changes in BP regulation, leading to significant increases in BP levels. By inducing atherosclerotic changes, stiffening of large arteries, renal dysfunction, and arterial baroreflex impairment, advancing age may induce progressive increases in systolic BP levels, promoting development and progression of arterial hypertension. It is also known, although mainly from studies in young or middle-aged subjects, that exposure to high altitude may influence different mechanisms involved in BP regulation (i.e., neural central and reflex control of sympathetic activity), leading to important increases in BP levels. The evidence is less clear, however, on whether and to what extent advancing age may influence the BP response to acute or chronic high altitude exposure. This is a question not only of scientific interest but also of practical relevance given the consistent number of elderly individuals who are exposed for short time periods (either for leisure or work) or live permanently at high altitude, in whom arterial hypertension is frequently observed. This article will review the evidence available on the relationship between aging and blood pressure levels at high altitude, the pathophysiological mechanisms behind this complex association, as well as some questions of practical interest regarding antihypertensive treatment in elderly subjects, and the effects of antihypertensive drugs on blood pressure response during high altitude exposure.
Introduction
E
Little is known, however, regarding the changes in BP levels under the combined influence of advancing age and acute or chronic exposure to high altitude. This issue is relevant because: 1) nowadays many elderly individuals maintain active lifestyle and may be acutely exposed to high altitude (e.g., when skiing or hiking); 2) there are large populations living at high altitude in Africa, Asia, and South America, including a consistent proportion of the elderly, where arterial hypertension is by no means a rare condition.
The present article is aimed at reviewing the evidence addressing the complex relationship between aging and blood pressure levels at high altitude, with particular attention to some of the pathophysiological mechanisms underlying this complex association (i.e., aging-related changes in large arteries and neurohormonal regulations). In the last part of the article, some questions of practical interest regarding antihypertensive treatment in elderly subjects and the problem of how antihypertensive treatment modifies the blood pressure response to high altitude exposure will be addressed.
Blood Pressure Changes with Aging
Consistent evidence indicates that aging is associated with a progressive increase in BP levels (Lewington et al., 2002) and arterial hypertension is very common in the elderly, being present in the vast majority of individuals who reach 90 years of age (Levy et al., 1996). Aging-related changes in arterial properties are among the major mechanisms responsible for this relationship. The arterial system in the youth is designed to receive spurts of blood continually from the left ventricle and to distribute this pulsatile input as steady flow through peripheral capillaries. In such a system, a proper coupling between the heart and the vascular tree minimizes aortic pressure fluctuations and limits flow pulsatility in the large arteries. Factors for optimal efficiency of vascular–ventricular interaction include greater distensibility of proximal than distal aorta, dispersion of peripheral reflecting sites, the location of the heart in the upper thorax, and the inverse relationship between heart rate and body length (Taylor, 1967).
With aging, the pulsatory behavior of BP may cause fatigue and fracture of elastin lamellae of central arteries, leading to replacement of elastic by connective tissue, thus causing arteries to stiffen and dilate. Changes are most marked in the aorta and its major proximal branches, and less marked in the peripheral muscular arteries (O'Rourke et al., 1968; Virmani et al., 1991; Boutouyrie et al., 1992; Lakatta, 2000; Wilkinson et al., 2001).
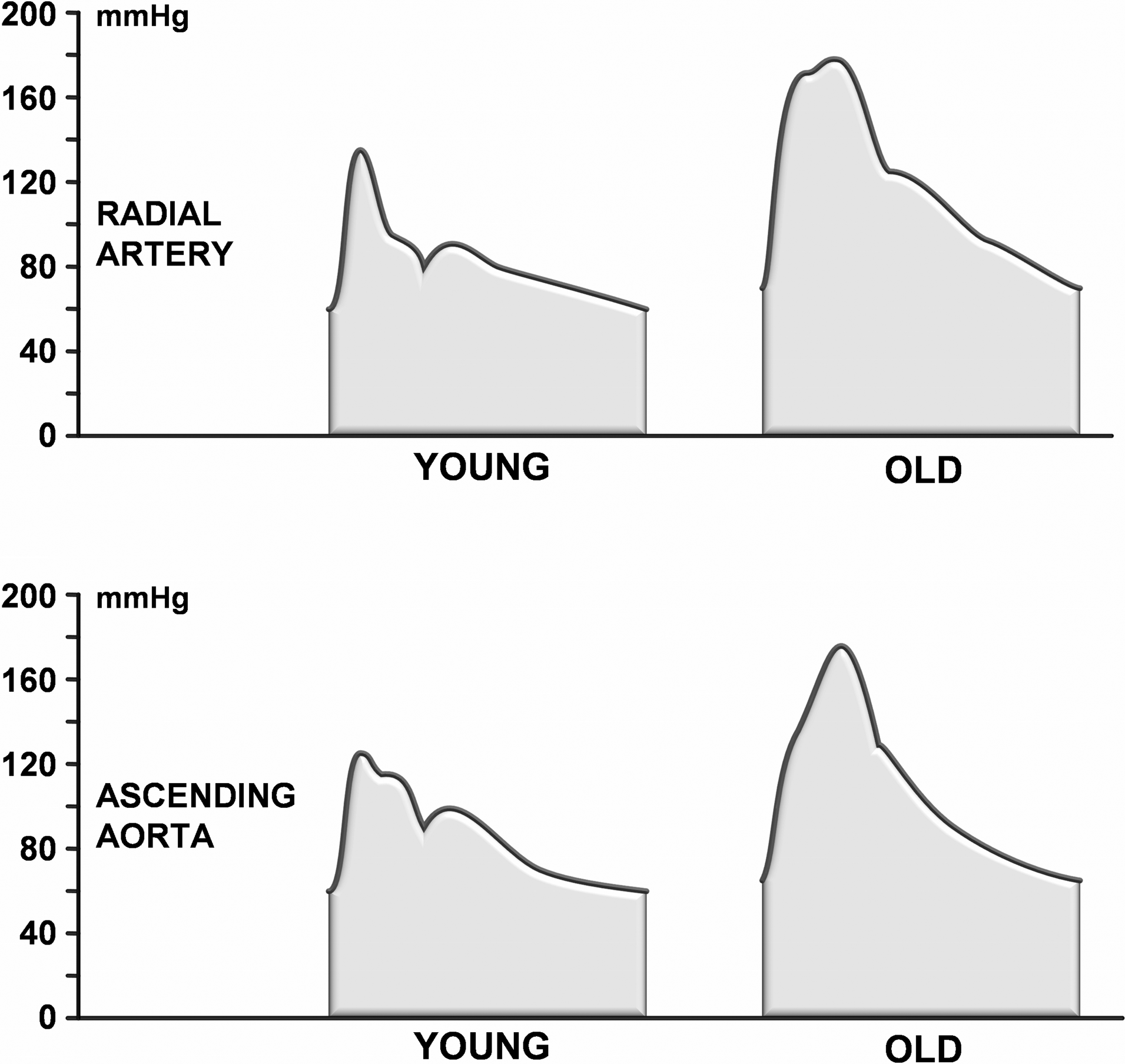
As the aorta ages and stiffens, aortic pulse wave velocity (PWV) increases, wave reflection returns earlier to the heart and the favorable interactive “tuning” between LV and arterial tree is progressively lost (Kelly et al., 1989). As a consequence, aortic systolic pressure rises, diastolic pressure falls, and pulsations of flow extend further into smaller vessels (O'Rourke and Hashimoto, 2007). The approximately two-fold increase in aortic PWV that occurs between 20 and 80 years is less evident in brachial pulse pressure. Moreover, while in the younger subjects pulse pressure (and also systolic BP) is markedly higher in brachial or radial artery than in the aorta (the phenomenon known as blood pressure amplification), this difference is much lower in the elderly (Nichols et al., 2011; Salvi 2015) (Fig. 1).

Schematic representation of the amplification phenomenon of blood pressure. In young people (left panel), the delayed superposition of reflected waves (dark gray areas) on forward waves (light gray areas) in ascending aorta causes a considerable difference in systolic blood pressure between peripheral and central arteries; this difference in systolic blood pressure is known as “amplification phenomenon”. In the elderly (right panel), reflected waves return earlier in ascending aorta because of arterial stiffness. As a result, there is a precocious superposition of backward waves on forward waves and a reduced amplification phenomenon. Taken from Salvi et al., 2015 by permission.
The effects of aging on arterial function and in BP levels may thus be underestimated if focus is put on brachial cuff systolic pressure only. In fact, while brachial pulse pressure increases with aging roughly from 35 to 60 mm Hg (i.e., by 70%) (Franklin et al., 1997), the increase in central aortic pulse pressure is even more prominent, roughly from 22 to 65 mm Hg (i.e., almost three-fold) (Fig. 2). Thus, in order to have a better estimate of the age-related changes in BP levels, aortic central BP levels should be considered in addition to conventional brachial cuff pressures measurements.
Pressure Waveforms in the radial artery (top panel) and in the ascending aorta (lower panel) of young and old subjects. Taken from Salvi et al., 2015 by permission.
Regarding the response of pulse pressure at altitude, a recent study explored whether central and peripheral pulse pressure values might be affected by exposure to high altitude hypoxia and the effects on them by acetazolamide (i.e., a drug prescribed to prevent and treat mountain sickness). Overall, exposure to high altitude was associated with progressive reductions in central and peripheral pulse pressure (Fig. 3). Potential mechanisms for this include reductions in stroke volume associated with hypoxia-triggered tachycardia and the increase in diastolic BP levels caused by the increase in vascular tone associated with the increase in central sympathetic drive to peripheral vasculature (Parati et al., 2013).
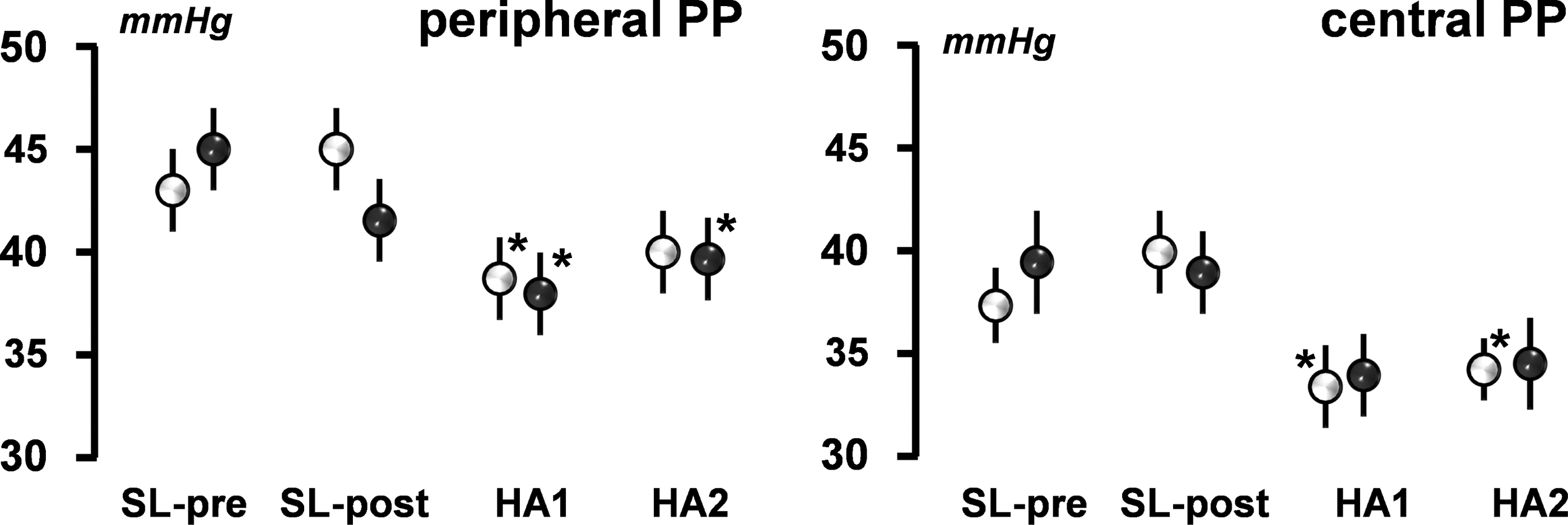
Behavior of peripheral and central pulse pressure levels during acute exposure to high altitude. Values are comparatively shown for the placebo group (white circles) and the acetazolamide group (black circles) at the different steps of the HIGHCARE Alps 2011 Study. Central blood pressure was measured at the common carotid artery; and peripheral blood pressure was measured at the brachial artery. Data are expressed as mean+SE. *p=0.05, vs. sea level basal values of the same group. HA1, high altitude, within 4–6 h after arrival to 4559 m a.s.l.; HA2, after 2 full days of permanence at high altitude; PP, pulse pressure; SL-pre, sea level, off treatment; SL-post, sea level, on treatment.
Apart from the alterations in elastic properties of arterial walls, aging is also associated with increased central sympathetic drive to peripheral circulation and with impairment in neural and reflex mechanisms of BP control, which in turn promote elevation of BP levels, and development, progression, and establishment of arterial hypertension. Of note, aging-related increases in aortic stiffness and thickening of intima-media layers (Nagai et al., 1998) may be responsible for a reduced stimulation of arterial baroreceptors located in these vascular areas by pulsatile BP (Mattace-Raso et al., 2007). The consequently reduced sensitivity of the arterial baroreflex reduces its efficacy in modulating sympathetic drive and thus in buffering BP fluctuations, leading to the increased systolic BP and pulse pressure variability typically observed in the elderly (Schillaci et al., 2012).
Evidence has also been provided by several studies that aging is associated with changes in the activity or responsiveness of hormonal systems, which in due course influence homeostatic mechanisms in the elderly (Weinstein and Anderson, 2010). In particular, aging disrupts the activity and responsiveness of the renin-angiotensin-aldosterone system (RAS). The altered systemic and intrarenal RAS may predispose the elderly population to acute kidney injury and chronic kidney disease (leading to fluid and electrolyte imbalances) (Yoon and Choi, 2014); development and progression of myocardial hypertrophy (Kumar et al., 2008), and vascular dysfunction, all of which may promote the development of arterial hypertension. Finally, the change in RAS activity leads to an altered response to RAS blockade. Indeed, the effects of angiotensin-converting enzyme (ACE) inhibitors on blood pressure, renal function, and proteinuria are blunted in aging animals (Anderson et al., 1994) and elderly populations exhibit a decreased antihypertensive response to ACE inhibitors than younger groups (Anderson, 1997).
High Altitude and Blood Pressure
During acute exposure to high altitude, important ventilatory and cardiovascular adaptations develop in response to changing environmental conditions, in particular to hypobaric hypoxia, in order to maintain homeostasis. The reduction in oxygen partial pressure in the inspired air determines a reduction in venous blood re-oxygenation. As a consequence of reduced quantity of blood transported oxygen, oxygen extraction to peripheral tissues is also reduced, leading to a significant reduction in exercise capacity. A proper adaptive cardiovascular response to altitude is thus essential.
Under high altitude exposure, systemic BP undergoes significant changes as a net result of a number of physiological responses. The pattern of these changes seems to have three distinct phases. Over the first minutes or hours of hypoxia exposure, BP remains largely unchanged because of direct vasodilatory effect of hypoxia counteracting chemoreflex-induced sympathetic activation (Wolfel et al., 1994). Subsequently pressor mechanisms begin to dominate, leading to BP increase (Hansen and Sander, 2003). Finally, after a longer period of high altitude permanence, these mechanisms may be partly inhibited when blood oxygen concentration increases through both ventilatory and alveolar diffusion acclimatization and hematocrit increase (the latter due to erythropoiesis and reduction in plasma volume). This may explain lower BP values observed in highlanders when compared to lowlanders exposed to altitude hypoxia (Grocott et al., 2007).
BP responses to high altitude over relatively short periods of time (days, weeks) have been most extensively investigated and seem to be quite relevant from a clinical point of view. In fact, short-term exposures to high altitude are common among tourists, skiers, or workers, and the associated BP increase may be clinically relevant as suggested by the finding of increased risk of sudden death in skiers with pre-existing hypertension acutely exposed to high altitude (Burtscher, 2007). Several studies at high altitude have reported BP increase during acute exposure based on conventional BP measurement (Bartsch et al., 1988; Reeves et al., 1992, Modesti et al., 2006). This method, however, has important acknowledged limitations (limited reproducibility, presence of “white-coat effect”, observer bias, etc.). More solid information comes from studies that implemented 24 h ambulatory blood pressure monitoring, a technique known to provide a much more accurate and comprehensive assessment of BP behavior over day and night (O'Brien et al., 2013; Parati et al., 2014b).
In one of the first studies in this field, Wolfel et al. (1994) showed a variable increase in day and night ABP in 5 subjects under placebo during acute and prolonged exposure to an altitude of 4300 m. Further contributions came from our group, through a set of HIGHCARE (HIGH altitude CArdiovascular REsearch) projects. In the HIGHCARE-ALPS study (Bilo et al., 2011), conducted in a group of healthy young or middle-aged individuals, ambulatory BP and HR significantly increased during a relatively short (2–3 days) permanence at high altitude (4559 m). This increase was mainly evident during night-time, leading to a reduced degree of nocturnal blood pressure fall compared with sea level (Bilo et al., 2011). Potential mechanisms for the night time BP rise during HA exposure include poor sleep quality/sleep fragmentation (which cause sympathetic activation) as well as oxygen desaturation episodes associated with sleep-related breathing disorders (where hypoxia causes chemoreflex-induced increase in sympathetic activity) (Lombardi et al., 2013).
Other potential, although less studied mechanisms, include impairment in baroreflex function, which may affect BP responses to posture changes and sleep (Bernardi et al., 1998), increased blood viscosity, increase in vasopressin and endothelin-1 levels, as well as fluid alterations associated with dysregulation of the RAS system. A further report from the HIGHCARE-Himalaya study, a parallel group, randomized, double-blind trial, explored the changes in conventional BP and 24 h ambulatory BP when moving from sea level to high altitude (Parati et al., 2014a). In this study the exposure to progressively higher altitudes was associated with a progressive, marked increase of systolic and diastolic ambulatory BP levels, more evident than the increase in conventional BP. This increase occurred immediately after the high altitude was reached; persisted during prolonged altitude exposure; involved the daytime ambulatory BP values, but—also in this case—was particularly pronounced for the night-time BP levels, with a consequent reduction of the nocturnal dipping phenomenon, maximal at the highest altitude reached, and disappeared after return to sea level (Parati et al., 2014a) (Fig. 4).
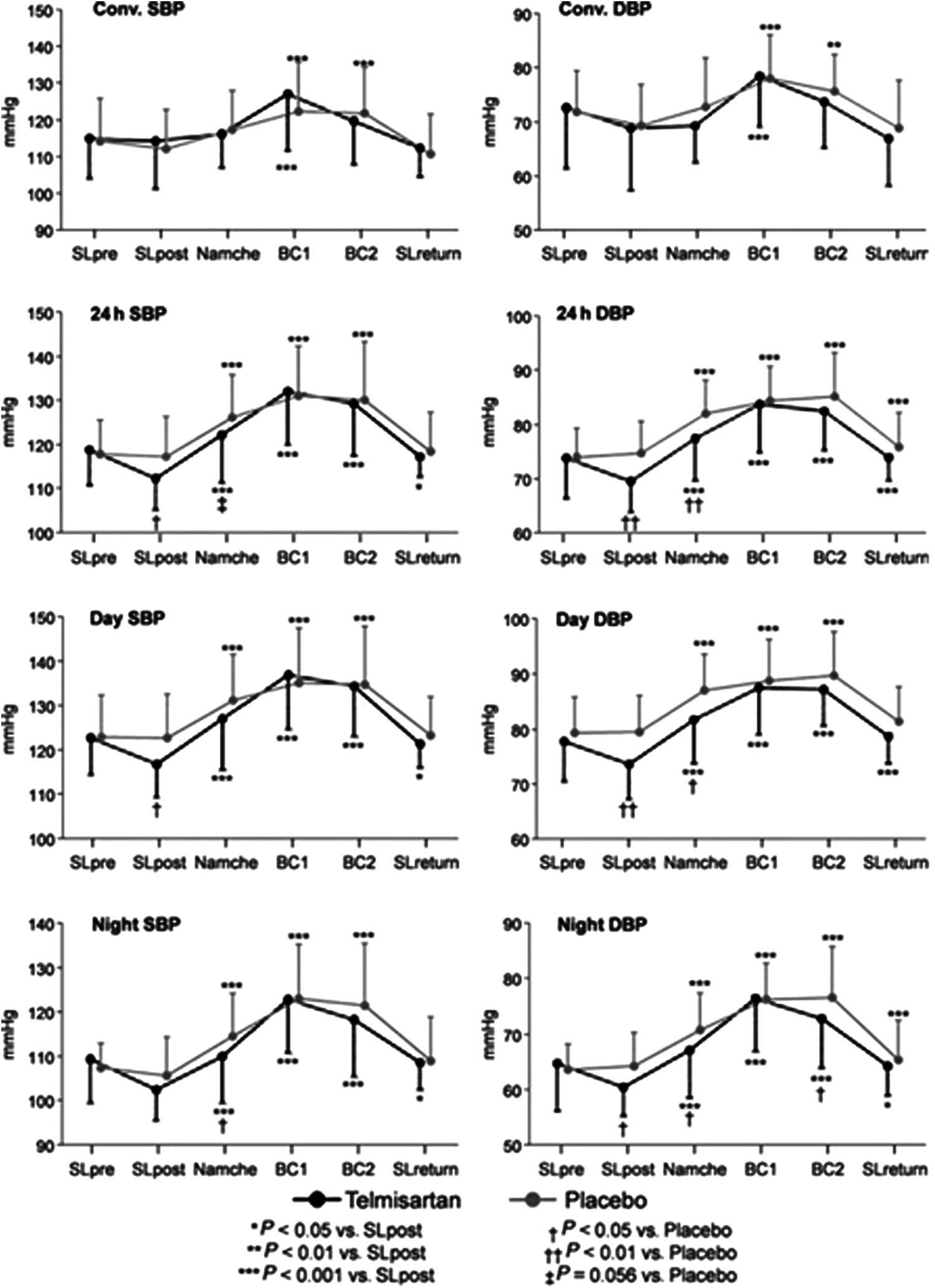
Conventional, 24 h, daytime and night-time systolic blood pressure (SBP) and diastolic blood pressure (DBP) for the different study conditions. Data from the HIGHCARE-Himalaya study in participants randomized to receive placebo or telmisartan 80 mg once a day. ***p<0.001 vs. SLpost; **p<0.01 vs. SL-post; *p<0.05 vs. SL-post; ##p<0.01 vs. Placebo; #p<0.05 vs. Placebo; §p=0.56 vs. Placebo. Modified from Parati et al., 2014a by permission.
Finally, in the HIGHCARE-Andes Lowlanders Study carried out in 2012, BP response to altitude was assessed for the first time in a group of hypertensive subjects (Bilo et al., 2013), showing a significant increase in BP levels over the 24 hours, and separately during daytime and nighttime subperiods, on top of the already elevated BP levels characterizing the hypertension condition (Bilo et al., 2013). Of note, the increase in ambulatory BP tended to be more pronounced compared with conventional BP, further emphasizing the finding from the HIGHCARE Himalaya study (Parati et al., 2014a) that casual conventional BP measurements may underestimate the pressor effect of high altitude hypoxia. This increase was accompanied by an attenuation of nocturnal BP fall (dipping), possibly explained by a further reduction in SpO2 accompanied by a further increase in sympathetic activity, which occur during sleep at high altitude, as compared to daytime period.
Finally, previous reports have indicated that ethnic differences and genetic variation may influence the magnitude of physiological adaptations during high altitude exposure (Vats et al., 2013). One of these studies exploring the variation in acclimatization patterns of two different ethnic groups (Indian vs. Kyrgyz subjects) on going from sea level to 3200 m, showed significant increases in diastolic blood pressure and heart rate after 3 days permanence at altitude in Indian but not in Kyrgyz subjects, in whom significant increases were only evident by day 14. (Vats et al., 2013). Another study addressing the effect of migration (intergenerational change) in BP levels between Tibet-born and India-born Tibetans permanently residing in Northern India, did not find significant differences in BP between two generations in both the sexes (Bera, 2006). Despite these findings, the effect of altitude on BP levels in persons belonging to different ethnic groups and how aging may modulate this relationship should still be properly studied.
Physiological Mechanisms Underlying BP Responses to High Altitude
As discussed previously, BP response to high altitude is multiphasic, and is the net effect of complex changes in regulatory mechanisms, determined by their sequence and timing.
In the initial response, the prevailing mechanism is a direct vasodilatory effect of hypoxia, relying on local regulatory mechanisms aimed at assuring adequate oxygen supply to peripheral tissues. These mechanisms include production and generation of nitric oxide (NO), ATP release from red blood cells, and changes mediated by hypoxia inducible factor-1 (HIF-1).
If the exposure to high altitude lasts for a few hours or more, pressor mechanisms dominate, the most important one being sympathetic activation. Hypoxia is a potent sympathetic activator via stimulation of the peripheral chemoreceptors, as demonstrated by the increase in heart rate and plasma norepinephrine observed in this condition (Wolfel et al., 1994). Similarly, in the placebo group of HIGHCARE-Himalaya study, noradrenaline showed a marked progressive increase with exposure to the 3400 and 5400 m altitudes, with a tendency to return to baseline values upon return to sea level (Valentini et al., 2012; Agostoni et al., 2013; Parati et al., 2014a) (Fig. 5).
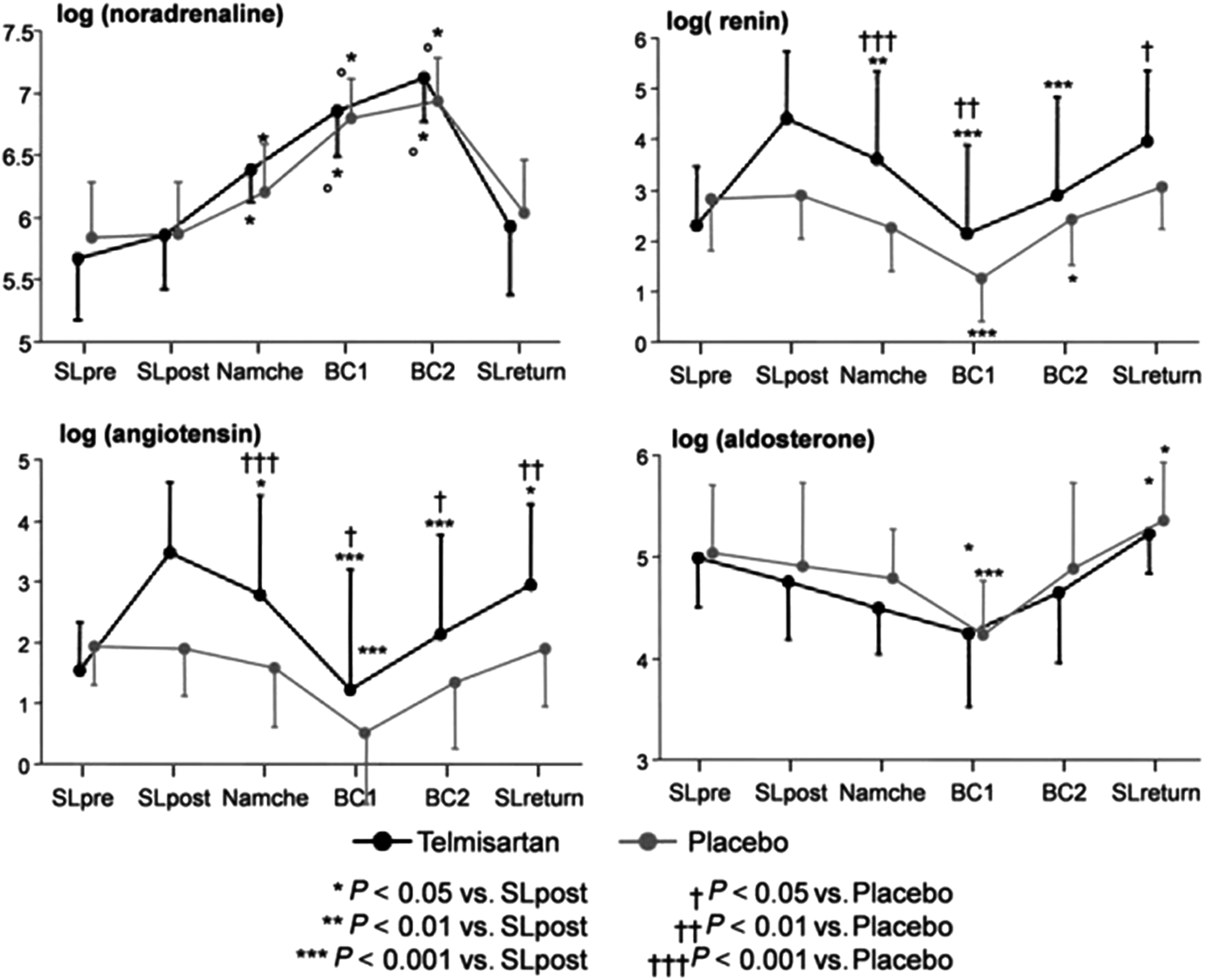
Plasma noradrenaline (log[ng/L]) and renin (log[mU/L]), serum angiotensin (log[pg/ mL]), and aldosterone (log[ng/L]) levels in both treatment groups throughout the HIGHCARE Himalaya study, in participants randomized to placebo or telmisartan 80 mg once a day. Noradrenaline: °p<0.001 vs. Namche; ***p<0.001 vs. SL-post. Others: ***p<0.001 vs. SL-post; **p<0.01 vs. SL-post; *p<0.05 vs. SL-post; ###p<0.001 vs. Placebo; ##p<0.01 vs. Placebo; #p<0.05 vs. Placebo. Modified from Parati et al., 2014a by permission.
An even more direct evidence of sympathetic activation in this setting comes from a study by Hansen et al. where the frequency of firing of sympathetic nervous fibers, recorded with peroneal nerve microneurography, was clearly increased during high altitude exposure (Hansen and Sander, 2003). Moreover, exposure to high altitude is associated with a number of environmental stimuli, other than hypoxia, which can stimulate the sympathetic nervous system: low temperature, psychophysical stress, poor sleep quality, pain (headache). The main effects of sympathetic activation include peripheral vasoconstriction, increase in heart rate and myocardial contractility, all of which favor an increase in BP.
While sympathetic activation is likely to be the primary reason for the pressor response to high altitude, other mechanisms may be also involved, many of which were investigated in the HIGHCARE-Himalaya study. During high altitude permanence, hematocrit levels increase as a consequence of plasma volume depletion and, later, by hypoxic stimulation of erythropoiesis (Piperno et al., 2011). In turn, an increased hematocrit leads to increased blood viscosity, which increases peripheral resistances and thus blood pressure levels (Parati et al., 2014a). The relative importance of blood viscosity in the determination of blood pressure has been emphasized by the evidence from studies in hypertensive polycythemic patients in whom reductions in blood viscosity without changing blood volume (i.e., isovolumic hemodilution) causes a significant fall in both clinic and 24-hour ambulatory BP levels (Bertinieri et al., 1998).
An increase in endothelin-1 levels may also contribute to vasoconstriction and elevation of BP levels during high altitude exposure (Modesti et al., 2006). Conversely, no contribution to the pressor effect seems to come from the renin-angiotensin-aldosterone system. In fact, in line with previously published data (Zaccaria et al., 1998), in HIGHCARE-Himalaya the activity of this system appeared suppressed, most evidently when very high altitude (5400 m) was reached (Modesti et al., 2006). Among underlying mechanisms, a direct inhibition of renin secretion and an inhibiting effect of increased BP on juxtaglomerular apparatus can be hypothesized.
It is not clear why the increase in BP at high altitude appears particularly pronounced at night. Plausible causes of this phenomenon include: poor sleep quality; nocturnal SpO2 reduction (compared with daytime levels) leading to a greater night-time hypoxic chemoreceptor stimulation; altered baroreflex function, possibly affecting physiological BP responses to supine position during sleep.
Another possible mechanism whereby high altitude exposure leads to changes in BP levels is related to functional changes in elastic properties of large arteries. In fact, in healthy subjects acutely exposed to an altitude of 4559 m, the HIGHCARE-ALPS study showed a significant increase in carotid-femoral PWV, a recognized index of aortic stiffness, and an increase in central aortic systolic pressure (Parati et al., 2013). Similar changes were found also in healthy participants of HIGHCARE-Himalaya at 5400 m (unpublished data). The mechanisms behind this finding are unclear. Distensibility of large arteries depends on intrinsic structural characteristics of the vessels, and on transient functional alterations of vascular wall itself. One could hypothesize that sympathetic activation leads to an increase in the tone of smooth muscle cells present in the wall of the aorta and large arteries, thereby increasing their rigidity. However, no change was observed in carotid-radial PWV (i.e., an index of distensibility of muscular arteries), which could be expected to be affected by sympathetic activation to an even higher degree. Therefore one may not exclude that hypoxia induces transient changes in the viscoelastic properties of arterial wall matrix.
Figure 6 resumes the main mechanisms by which aging and high altitude may influence BP regulation during high altitude exposure.
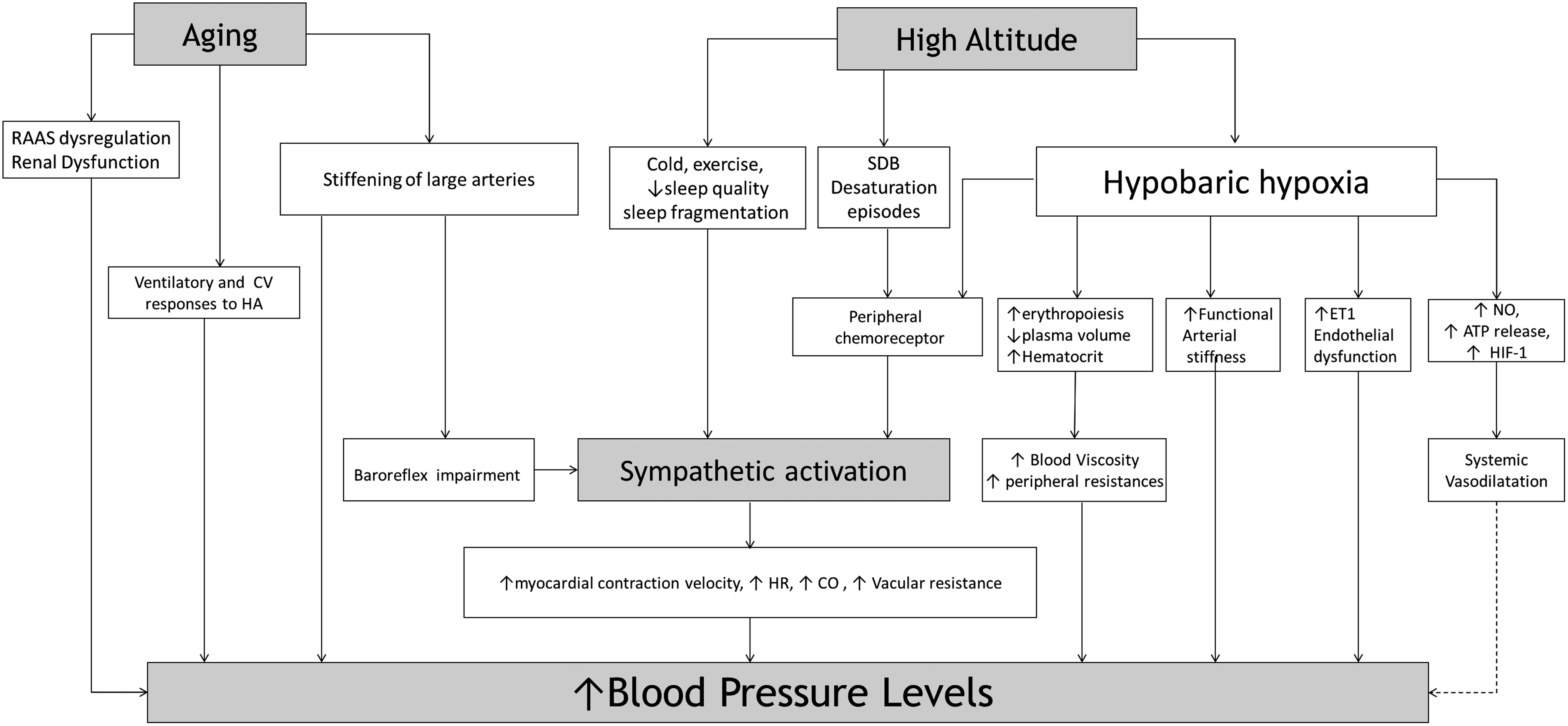
Effects of aging and altitude in BP regulation. CO, cardiac output; CV, cardiovascular; DBP, diastolic blood pressure; ET-1, endothelin-1; HA, high altitude; HIF-1: hypoxia inducible factor-1; HR, heart rate; NO, nitric oxide; PP, pulse pressure; RAAS, renin angiotensin aldosterone system; SBP, systolic blood pressure; SDB: sleep disordered breathing.
Effects of Aging on Blood Pressure and Its Regulation at High Altitude
The evidence on the physiological responses to high altitude in the elderly (i.e., subjects >65 years according to WHO definition) is limited and sometimes contradictory. For instance, discordant changes in hypoxic ventilatory drive with aging were described: while some authors observed its reduction in the elderly (65 to 79 years of age) compared with younger subjects (mainly due to reduced neuromuscular inspiratory output) (Peterson et al., 1981), others found that aging was associated with significant improvements in respiratory response to hypoxia and blood oxygenation, at least in men (Richalet et al., 2012).
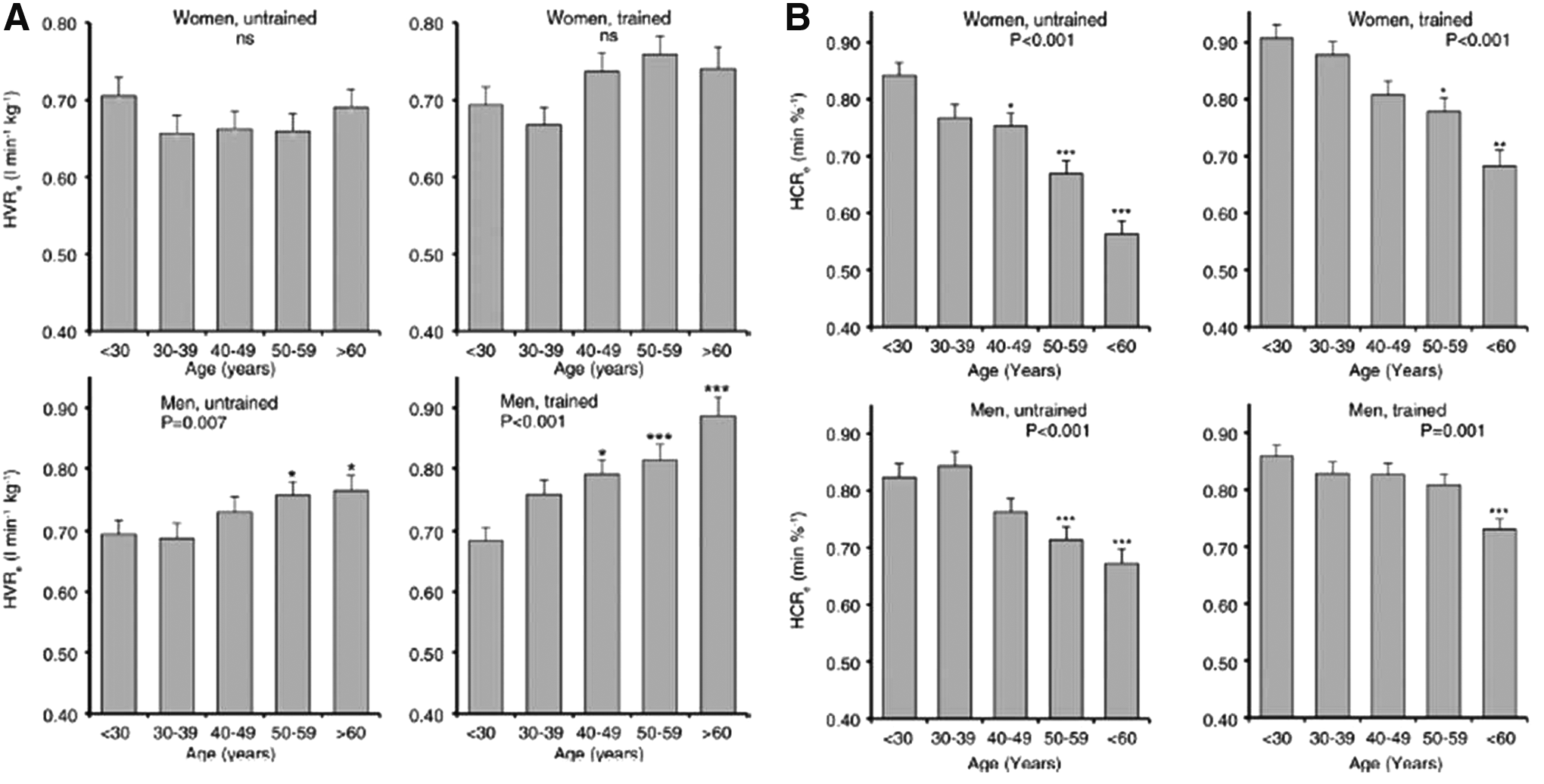
Although these alterations might theoretically affect the normal adaptive response to altitude in elderly subjects, the physiological response to acute exposure to hypobaric hypoxia in these subjects has been shown to be largely similar to that observed in younger individuals (Levine et al., 1997). In fact, after 5 days of high altitude exposure, elderly individuals (mean age 68±3 years) appear to acclimatize well, their responses being physiologically almost indistinguishable from those seen at sea level (Levine et al., 1997). Nonetheless, the observed changes in ventilatory physiology with aging suggest possible changes in chemoreflex function with potential consequences also in terms of cardiovascular reactions to high altitude. This possibility is further supported by the findings of a large cross-sectional study conducted by Richalet et al. (2012) in which increasing age was associated with a blunted cardiac response to hypoxia in both sexes, despite the significant improvements in respiratory response to hypoxia and blood oxygenation in men (Fig. 7).
A few studies directly addressed the relationship between aging and BP levels in people living at high altitude or the BP response to acute high altitude exposure in elderly subjects. Levine et al. (1997) assessed several hemodynamic variables in elderly subjects during acute simulated hypoxia (corresponding to 2500 m) and after 5 days of actual permanence at such an altitude. Compared with normoxic condition, they observed a decrease of BP in acute hypoxia, attributable to direct hypoxic vasodilation, with BP values returning to baseline level during high altitude sojourn. This was accompanied by a modest increase in heart rate. A similar pattern of changes was maintained also during exercise in both conditions.
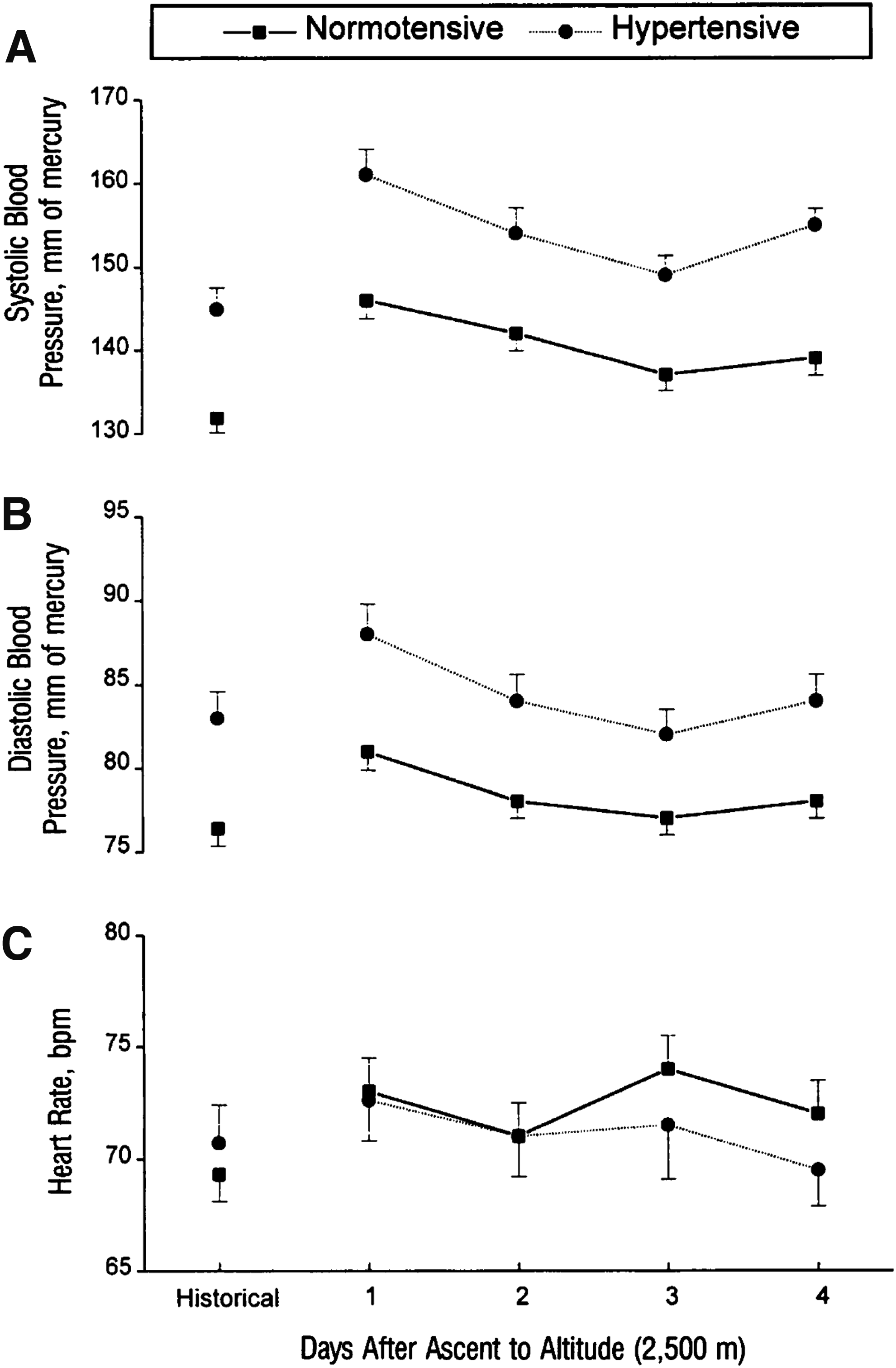
Interesting data were provided by Roach et al. (1995) on 97 elderly subjects (mean age 69.8±0.5 years; range, 59 to 83) during several days' sojourn at an altitude of 2500 m. The authors found a clearly increased BP on the first day of permanence, which decreased over the subsequent days. The values were much higher in subjects with arterial hypertension. An important limitation of this study was the fact that BP at sea level was obtained based on historical records and not directly measured (Fig. 8).
Systolic
There is only very limited information on the effects of aging on ambulatory blood pressure at high altitude. Our HIGHCARE-Himalaya study did not include elderly subjects; however, we observed that BP increase induced by high altitude exposure was more pronounced in the subgroup of subjects aged >50 years compared to the younger ones (Parati et al., 2014a).
To our knowledge, the only study directly comparing BP response to high altitude between older and younger subjects was published by Veglio et al. (1999). In this study, during acute exposure to moderate (2950 m) altitude, ambulatory BP increased to a similar extent in older (mean age 65.2 years, range 60–83) and younger adults (mean age 40.2 years, range 32–45), both during daytime and night-time, although the sample size of this study was too small to allow solid comparisons between groups (Fig. 9).
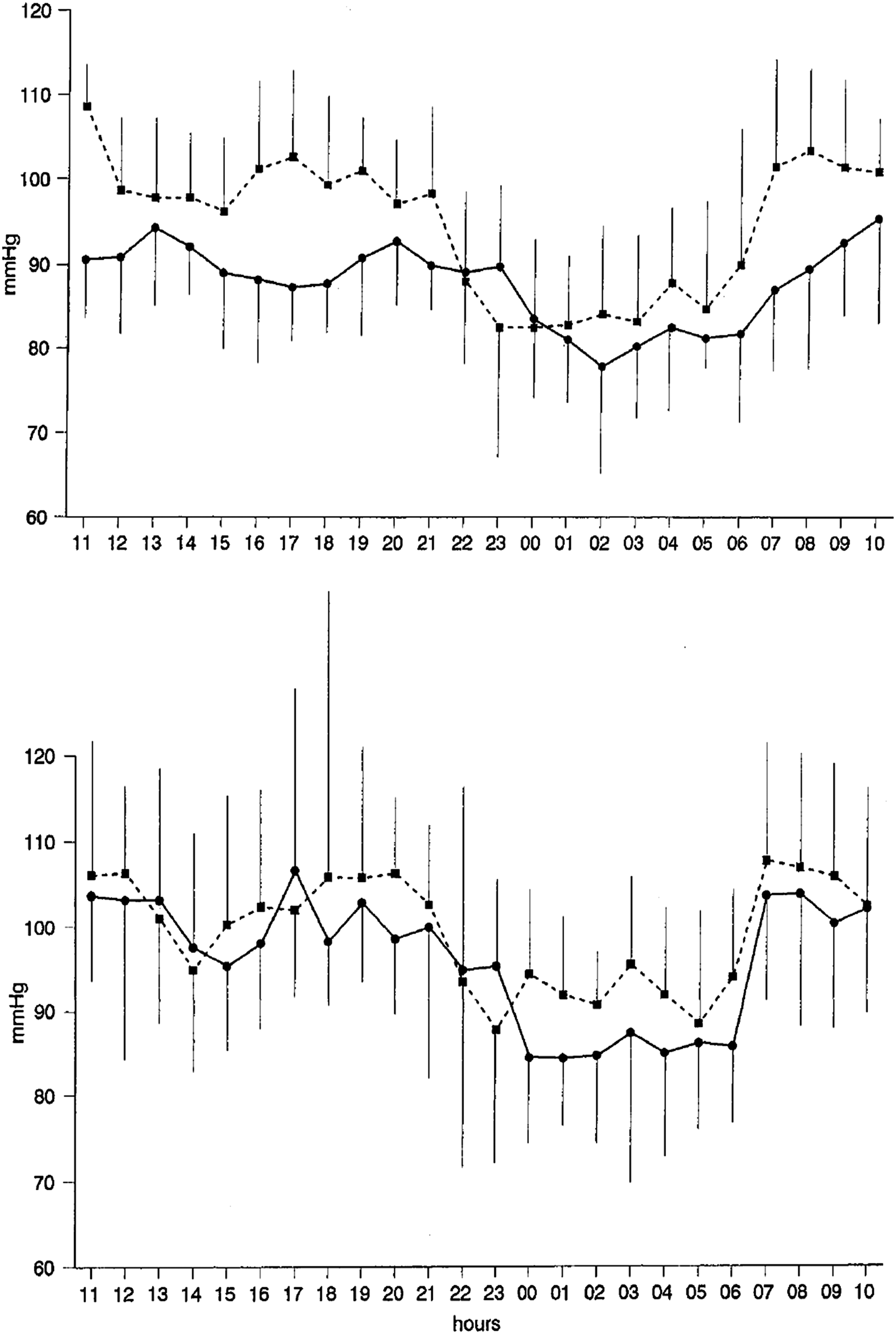
24-h mean blood pressure profile in basal condition (solid line) and at 2950 m (dashed line) in a group of adults (upper panel) and in a group of elderly subjects (lower panel). Modified from Veglio et al., 1999 by permission.
In the present review, we also aimed at addressing how BP behaves with aging in people permanently living at high altitude. Some information in this regard comes from a cross-sectional report conducted in a community of highlanders of Leh in Ladakh (332 subjects aged 13–81 years living at an altitude of 3524 m), and in a Japanese community of low-landers in U town, Hokkaido (216 citizens, 24–79 years of age living at 25 m above sea level), which comparatively investigated the effect of aging on BP levels and heart rate (Otsuka et al., 2005). Compared to lowlanders, people living at high altitude displayed higher diastolic BP levels and HR values (83.2 vs. 76.9 mmHg and 78.6 vs. 69.2 bpm, p<0.001) without significant difference for systolic BP levels. However, when BP levels were assessed as a function of age, highlanders exhibited a significantly higher increase in BP levels with age when compared to lowlanders (i.e., systolic BP increased 0.75 vs. 0.32 mmHg/year and diastolic 0.32 vs. 0.08 mmHg/year, respectively; Otsuka et al., 2005) (Fig. 10).This may suggest that the course of vascular aging is different in subjects living at high altitude, although it has to be remembered that such comparisons are made difficult by important confounders related to lifestyle. Moreover, elevated hematocrit in highlanders may have direct influence on BP levels, making the comparison even more difficult.
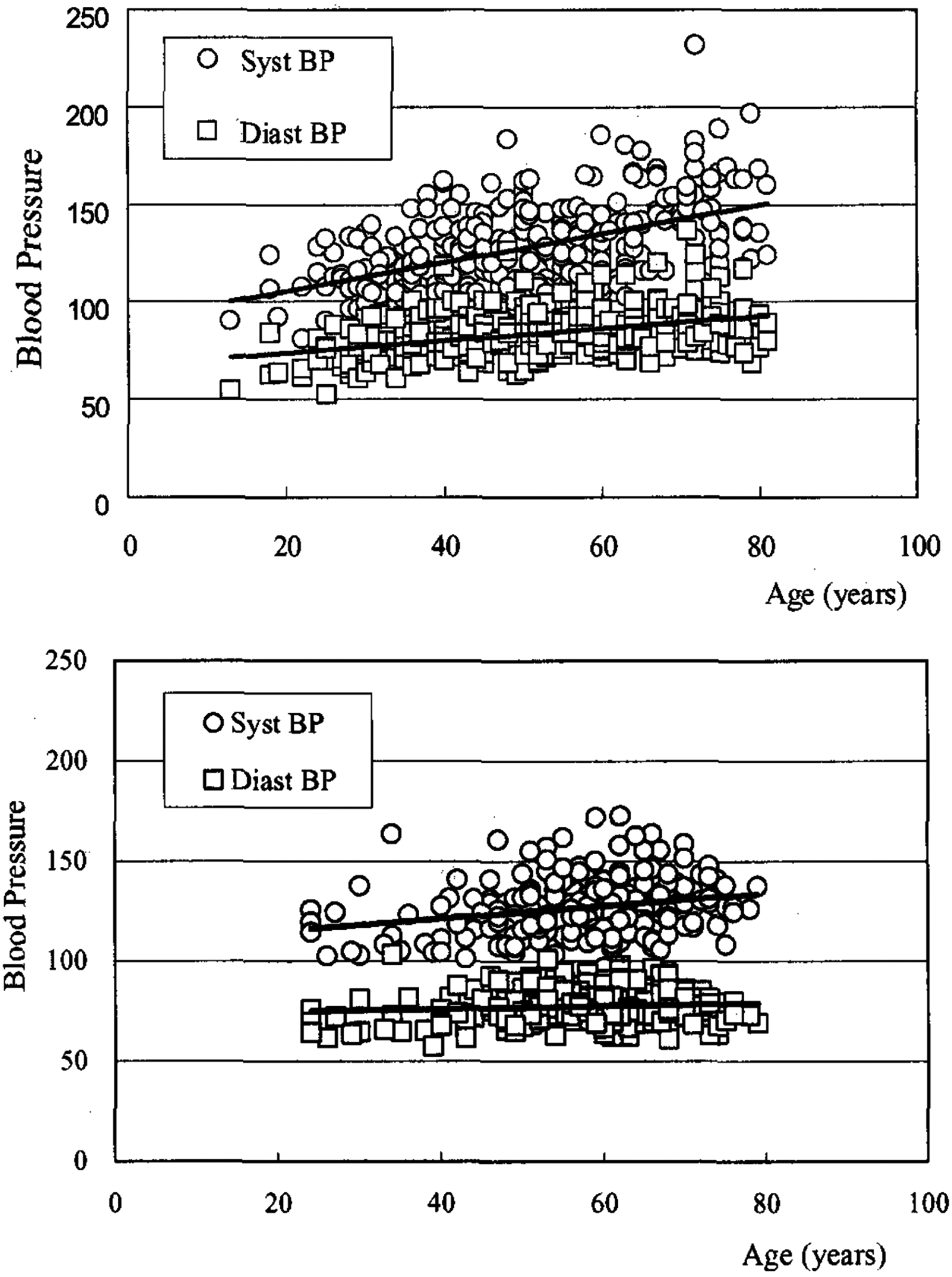
Comparison of slopes of regression lines between BP and age in highland (upper panel, Leh, Ladakh, altitude 3524 m, top) and lowland (lower panel, U town, Hokkaido, altitude 25 m, bottom) citizens. In this cross-sectional study, the increase in BP with age was steeper among highland than lowland residents (systolic BP: 0.7476 vs. 0.3179 mmHg/year, t=3.642, p<0.0005; diastolic BP: 0.3196 vs. 0.0750 mmHg/year, t=3.410, p<0.001). Taken from Otsuka et al., 2005 by permission.
Antihypertensive Treatment, Aging, and High Altitude
For many years an age-related increase in systolic BP was considered to be physiological and without clinical consequences. In 1990s, the first BP lowering trials in subjects aged over 65 years demonstrated clearly the clinical usefulness of antihypertensive treatment in this age group (Probstfield and Furberg, 1990). More recently, the HYVET trial extended the indication for BP lowering treatment beyond 80 years of age (Beckett et al., 2008). Consequently, the recent hypertension guidelines recognize that hypertension should be treated in elderly and very elderly subjects, at least whenever SBP is equal or higher than 160 mmHg (Mancia et al., 2013).
There is still debate, however, regarding the treatment choice. The European Society of Hypertension (ESH)/European Society of Cardiology (ESC) 2013 hypertension guidelines recommend treatment of hypertension in the elderly with the same drug classes used in younger individuals (with the exception of elderly patients with isolated systolic hypertension in whom the use of low-dose diuretics and dihydropyridine calcium channel blockers is supported) (Mancia et al., 2013). This recommendation is mainly based on the evidence of prospective studies and meta-analyses comparing the benefits of different antihypertensive regimens in patients younger or older than 65 years, which have shown that the BP lowering effects of antihypertensive drugs are not different between younger and older patients (Turnbull et al., 2008).
However, other hypertension societies (American Society of Hypertension, International Society of Hypertension, and NICE guidelines, as well as the Eighth Joint National Committee) suggest the use of specific drugs classes in the elderly, calling attention on the reduced effectiveness of certain drugs in this age group (i.e., ACE inhibitors and older generation beta-blockers) (Ritchie et al., 2011; Armstrong, 2014; Murthy et al., 2014).
Regarding treatment modifications when going to high altitude, although evidence suggests that blood pressure rises to a modest/moderate extent in patients with mild to moderate hypertension upon acute ascent to high altitude, there is no clear evidence of an increased risk of complications due to these increased pressures. Besides, there is little information about blood pressure responses in people with severe hypertension (blood pressure ≥160/95) who are often excluded from travel to and/or work at high altitude (Wu et al., 2007; 2012).
Given the prevalence of hypertension among high altitude travelers (from 6% to 14%) (Faulhaber et al., 2007), and the fact that some individuals have marked elevations in their blood pressure during HA exposure, it would seem obvious that those patients should have their medications adjusted. However, at present there are insufficient data to support specific recommendations on how to make these adjustments. Besides, the blood pressure responses at altitude are highly variable among subjects.
It is thus strongly recommended for those patients with poorly controlled or labile hypertension, or who know from prior sojourns that they have marked rises in their BP, to keep their BP levels monitored upon ascent to high altitude and travel with a plan for altering their medical regimen in the event marked or symptomatic BP elevations might occur, in accordance with sea-level practices for patients with hypertensive urgency or emergency. Given the wide availability of BP measuring devices for self-BP monitoring it is feasible and prudent for these patients to carry such devices with them on a high altitude sojourn, which would allow monitoring of their BP levels according to current guidelines (Parati et al., 2010).
Regarding the BP effects of antihypertensive medications at high altitude, only very few studies have explored this issue, and none of them has been specifically conducted in elderly subjects. The HIGHCARE-ALPS 2006 study (Bilo et al., 2011) conducted in a group of healthy young or middle-aged individuals, explored whether pharmacological blockade of adrenergic system with beta-blockers might have any important consequences in terms of blood pressure responses to acute high altitude exposure (Capanna Regina Margherita, 4559 m). In contrast to a study preformed previously (Wolfel et al., 1994) where the short-acting beta-blocker propranolol was used (currently less used in clinical practice), the HIGHCARE-ALPS 2006 study explored the effects of two vasodilating beta-blockers, carvedilol and nebivolol. These compounds, which are commonly prescribed in conditions characterized by an enhanced sympathetic activity, such as chronic heart failure and hypertension, differ in their degree of beta-l selectivity and in additional features apart from beta-adrenergic receptor blockade, such as alpha-adrenergic receptor antagonism and antioxidative properties (carvedilol) or vasodilating properties related to nitric oxide-releasing activity (nebivolol). These pharmacological differences might translate into relevant differences in their clinical effects, in conditions of sympathetic activation such as under hypobaric hypoxia exposure.
In the HIGHCARE-ALPS 2006 study, both these beta-blockers significantly reduced 24-h and daytime blood pressure at sea level (with a minor influence on night-time blood pressure) compared with placebo. At high altitude, 24-h blood pressure increased in all groups (compared with on-treatment values at sea level) and this increase was mainly driven by a marked elevation in night-time blood pressure. At high altitude, carvedilol fully maintained the BP lowering effect achieved at sea level, and thus 24-h blood pressure remained significantly lower in participants taking carvedilol than placebo. In contrast, at high altitude nebivolol lost some of the antihypertensive effect seen at sea level with a particularly marked increase in blood pressure during daytime. Conversely, the increase in night-time systolic blood pressure at high altitude with nebivolol was less pronounced than in placebo or carvedilol group with a lower proportion of participants who shifted to a non-dipping pattern. Thus, both vasodilating beta-blockers used in this study partly counteracted the increases in BP and HR at high altitude, with carvedilol being more potent than nebivolol.
Importantly, however, the use of beta-blockers was associated with tolerability issues: in both groups on active treatment oxygen saturation at high altitude was reduced compared with placebo and, in the carvedilol group, adverse effects were more pronounced and exercise capacity was more importantly reduced. Of note, the reduced exercise performance during HA exposure, similar to what has been shown in HF patients, may be favorably modulated by selective beta1-blockers such as bisoprolol and nebivolol (Valentini et al., 2012; Agostoni, 2013).
In the HIGHCARE-Himalaya study, a parallel group, randomized, double-blind trial, we assessed whether the efficacy of antihypertensive treatment with an angiotensin receptor blocker, telmisartan, in lowering conventional BP and ABP was maintained at high altitude. Healthy participants were randomized to receive either telmisartan 80 mg or placebo once daily. While telmisartan did not have a significant lowering effect on conventional BP, it caused a significant ambulatory BP reduction at sea level and at the altitude of 3400 m, without modifying significantly the size of the pressor response to such altitude. At 5400 m, however, the BP lowering effect of the drug was no longer evident upon arrival and after 12 days of permanence at this altitude. This behavior was explained by the suppression of the renin–angiotensin–aldosterone system, observed at the higher altitude. This implies that, in subjects already under angiotensin II receptor blockade, treatment efficacy will likely be maintained up to 3400 m, but the antihypertensive effect of angiotensin II receptor blockade will probably be lost at very high altitudes. Thus, this study showed that high altitude may modify the effects of cardiovascular drugs, in this case of an angiotensin receptor blocker, thereby affecting their efficacy.
In the HIGHCARE-Andes Lowlanders Study, BP changes in response to high altitude exposure and the BP effects of antihypertensive combination treatment with an angiotensin II receptor blocker and a calcium channel blocker (ARB/CCB) both at sea level and during high altitude exposure were assessed in a group of patients with mild hypertension (Bilo et al., 2015).
In this study, the combined treatment with telmisartan and slow-release nifedipine at an altitude of 3260 m maintained its efficacy and was well tolerated. Indeed, although the BP increase at altitude observed in the active treatment group was only slightly less pronounced than in the placebo group, in treated subjects BP levels at high altitude were lower than the initial BP values observed off-treatment at sea level. Moreover, active treatment group had higher SpO2 levels (possibly due to the known dilatatory effect of nifedipine on pulmonary circulation, improving lung ventilation-perfusion ratio).
Although the efficacy of the commonly used antihypertensive drugs is normally maintained in the elderly, it has to be acknowledged that none of the above studies included subjects aged above 65 years. One could argue, for instance, that the activity of the renin–angiotensin–aldosterone system is more frequently reduced in the elderly, and thus that the use of inhibitors of this system is less rational. Therefore, further information directly obtained from clinical studies on antihypertensive medication use in the elderly exposed to high altitude is needed.
Conclusions
Because of increasing awareness of healthy lifestyle, adequate preventive measures, and wider availability of effective therapies, an increasing number of people reach an advanced age in good health and wish to maintain active lifestyle, including activities at elevated altitudes. Although the prevalence of hypertension in this age group is very high, the knowledge regarding the behavior of blood pressure, the possible risks related to BP increases and the effects of antihypertensive medication during high altitude permanence is yet scanty.
The few available studies, sometimes yielding conflicting results, suggest that the cardiovascular responses of the elderly to high altitude exposure are not much different from what can be seen in younger subjects: an increase in BP and heart rate is evident, although the adaptation to high altitude permanence might be actually somewhat better. As regards pharmacological BP control at high altitude, no specific studies have ever been performed in elderly individuals. Thus, at present we can only extrapolate to elderly subjects what has been reported in middle aged and young individuals investigated both at sea level and at altitude, waiting for studies specifically addressing this issue.
Finally, an important area that requires much further research is how the exposure to modestly elevated altitudes (corresponding to many mountain resorts) affects elderly hypertensive patients with co-morbidities.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.