
Abstract
Abstract
Bloch, Konrad E., Tsogyal D. Latshang, and Silvia Ulrich. Patients with obstructive sleep apnea at altitude. High Alt Med Biol 16:110–116, 2015.—Obstructive sleep apnea (OSA) is highly prevalent in the general population, in particular in men and women of older age. In OSA patients sleeping near sea level, the apneas/hypopneas associated with intermittent hypoxemia are predominantly due to upper airway collapse. When OSA patients stay at altitudes above 1600 m, corresponding to that of many tourist destinations, hypobaric hypoxia promotes frequent central apneas in addition to obstructive events, resulting in combined intermittent and sustained hypoxia. This induces strong sympathetic activation with elevated heart rate, cardiac arrhythmia, and systemic hypertension. There are concerns that these changes expose susceptible OSA patients, in particular those with advanced age and co-morbidities, to an excessive risk of cardiovascular and other adverse events during a stay at altitude. Based on data from randomized trials, it seems advisable for OSA patients to use continuous positive airway pressure treatment with computer controlled mask pressure adjustment (autoCPAP) in combination with acetazolamide during an altitude sojourn. If CPAP therapy is not feasible, acetazolamide alone is better than no treatment at all, as it improves oxygenation and sleep apnea and prevents excessive blood pressure rises of OSA patients at altitude.
Clinical Aspects of Obstructive Sleep Apnea (Near Sea Level)
O
A sleep study demonstrating an increased number of apneas/hypopneas may confirm the diagnosis (Epstein et al., 2009). According to recent guidelines, an apnea/hypopnea index (i.e., a mean number of events per hour of sleep, AHI), equal to or exceeding 15/h, or an AHI equal to or exceeding 5/h associated with symptoms, also termed OSA syndrome, is required to confirm the diagnosis of OSA and consider treatment (Epstein et al., 2009). The severity of OSA is graded according to the AHI as mild, moderate or severe (>5 and <15/h, >=15 and <30/h, >=30/h, respectively). Symptomatic OSA is generally considered to warrant treatment in order to improve symptoms and quality of life, and to reduce the risk of traffic accidents and cardiovascular disease. Continuous positive airway pressure (CPAP) applied during sleep via a nasal mask is the main treatment for OSA (Basner, 2007), with behavioral modifications (regular sleeping hours, avoidance of alcohol, smoking, weight reduction in obese patients) recommended as adjunctive measures. In persons unable to tolerate CPAP, the use of a mandibular advancement device is an effective second line treatment option (Randerath et al., 2011). Surgical procedures are generally limited to selected cases (Won et al., 2008).
Age-Related Prevalence of Obstructive Sleep Apnea
The major clinical relevance of OSA is related to its serious consequences on the well-being of affected persons as well as to its very high prevalence. Epidemiologic studies in the general adult population have revealed prevalence rates of symptomatic sleep apnea (AHI ≥5/h) of 2% of middle-aged females and 4% of males (Young et al., 1993). If the prevalence rate of sleep apnea was evaluated independent of symptoms of OSA, even much higher prevalence rates have been reported; for example, 47% of a community sample of 5615 men and women participating in the Sleep Heart Health Study had an AHI ≥5/h (Young et al., 2002; Redline et al., 2004). Advanced age and male gender were major determinants of the risk of having OSA. Thus, the odds of having an AHI ≥15/h increased by 52% (95% confidence interval 40%–65%) with every decade of age above 40 years when adjusted for various cofactors. The adjusted odds for having sleep apnea (AHI ≥15/h) was 1.51 (95% confidence interval 1.20–1.90) for men compared to women (Young et al., 2002).
Age and High Altitude Periodic Breathing
In healthy subjects, the increased ventilatory drive induced by exposure to hypobaric hypoxia promotes high altitude periodic breathing, an alternating pattern of hyperventilation, and central apneas/hypopneas associated with cyclic oscillations of oxygen saturation and sleep disturbances (Nussbaumer-Ochsner et al., 2012b; Latshang et al., 2013) In a study performed in 51 healthy subjects sleeping at 490, 1630, and 2590 m, multiple regression analysis controlling for various confounding factors including the AHI and mean nocturnal oxygen saturation at 490 m baseline (among others) predicted a slightly greater AHI in the first night at 2590 m in persons aged 38 years (i.e., 10.9/h) compared to persons aged 24 y (9.3/h) and 20 y (8.9/h), respectively (Table 3 in Latshang et al., 2013). There was a large variation in the individual susceptibility to altitude-related periodic breathing in that study. In children, 9–12 years old, ascending from 490 m to 3450 m within a few hours, we observed a reduced amount of periodic breathing in the first night at high altitude compared to accompanying fathers, aged 36–57 years. Thus, the mean time of the night spent with periodic breathing was only 8% in children, whereas the corresponding value in fathers was 34%, even though the nocturnal oxygen saturation of children and fathers was similar (85% vs. 84%) (Kohler et al., 2008). The difference in susceptibility to periodic breathing was related to a lower apnea threshold in children. Whether aging, or physiologic changes during puberty, or other factors were responsible for the different prevalence rates of periodic breathing in this study remains elusive.
In studies performed at very high altitude, up to 6250 m at Muztagh Ata, age seemed not to have played a major role in predisposing to high altitude periodic breathing when various confounding factors were controlled for in multiple regression (Bloch et al., 2010). A systematic analysis of the literature revealed that studies on high altitude periodic breathing, including the ones cited above, have included mostly younger subjects, and the number of participants was small (Nussbaumer-Ochsner and Bloch, 2014). Therefore, the data available to date do not allow to conclusively assess the effects of age on high altitude periodic breathing.
Effects of Altitude in Lowlanders with OSA
Given the high prevalence of OSA, it is expected that a large proportion of the increasing number of mountain travelers suffer from OSA, among them many older persons. Since both OSA and older age are associated with increasing cardiovascular and other co-morbidities, there are concerns that the combined effects of intermittent and sustained hypoxia during a stay at altitude may expose OSA patients to an excessive risk of adverse health effects.
A preliminary reports on 5 OSA patients exposed to a simulated altitude of 2750 m in a normobaric, hypoxic chamber near sea level has suggested that obstructive apneas were replaced by central apneas (Burgess et al., 2006). In another study, 11 OSA patients living at an altitude of >2400 m underwent sleep studies at their home residence, in a sleep laboratory at 1370 m, and near sea level (5 of the 11 patients) (Patz et al., 2006). The highest AHI was recorded at the highest elevation, at the altitude of residence, while descending to lower elevation was associated with a decrease in sleep apnea due to disappearance of central events. No details on other physiologic consequences such as on sleep structure, daytime performance, or cardiovascular effects were provided. Systematic studies of the effects of altitude exposure in patients with OSA were therefore needed in order to create robust scientific evidence as a basis to counsel OSA patients planning altitude travel. To address this point, we undertook a series of randomized, controlled trials evaluating clinical and physiologic effects of altitude in patients with OSA. These studies will be discussed in the following.
Because carrying a CPAP device is inconvenient, and electrical power is not generally available in remote mountain areas, certain patients with OSA prefer to discontinue their CPAP therapy during altitude travel. In order to reflect this behavior and its physiological consequences, we asked 34 lowlanders with OSA living below 800 m and using long-term CPAP therapy to discontinue the treatment for 3 nights before undergoing baseline studies at 490 m (Nussbaumer-Ochsner et al., 2010). Subsequently, participants traveled within a few hours to Swiss mountain villages at 1860 m and 2590 m, respectively, and stayed at each altitude for 2 nights.
Expectedly, discontinuation of CPAP therapy resulted in recurrence of breathing disturbances with moderate to severe OSA at 490 m (median AHI off CPAP of 51.2/h). At 1860 m and even more so at 2590 m, mean nocturnal oxygen saturation was significantly reduced (to median values of 86% in the first night at 2590 m) and the AHI was considerably increased (median AHI of 90.0/h), mainly due to emergence of central apneas/hypopneas (Fig. 1, panel A). This was associated with reductions in sleep efficiency and deep non-rapid eye movement sleep (NREM stages 3 and 4), and with frequent arousals. Although questionnaire evaluations suggested that patients did not feel more sleepy after spending nights at the higher altitudes, driving simulator tests revealed that their ability to stay in the center of the simulated street was impaired, and more off-road events occurred (Fig. 2). Cardiovascular effects in the OSA patients staying at moderate altitude without CPAP therapy consisted in an elevated heart rate and blood pressure (median increase of 5 and 15 mmHg in diastolic and systolic blood pressure, respectively), more frequent nocturnal arrhythmias, a gain in weight of about 1 kg, and peripheral edema (Nussbaumer-Ochsner et al., 2010).
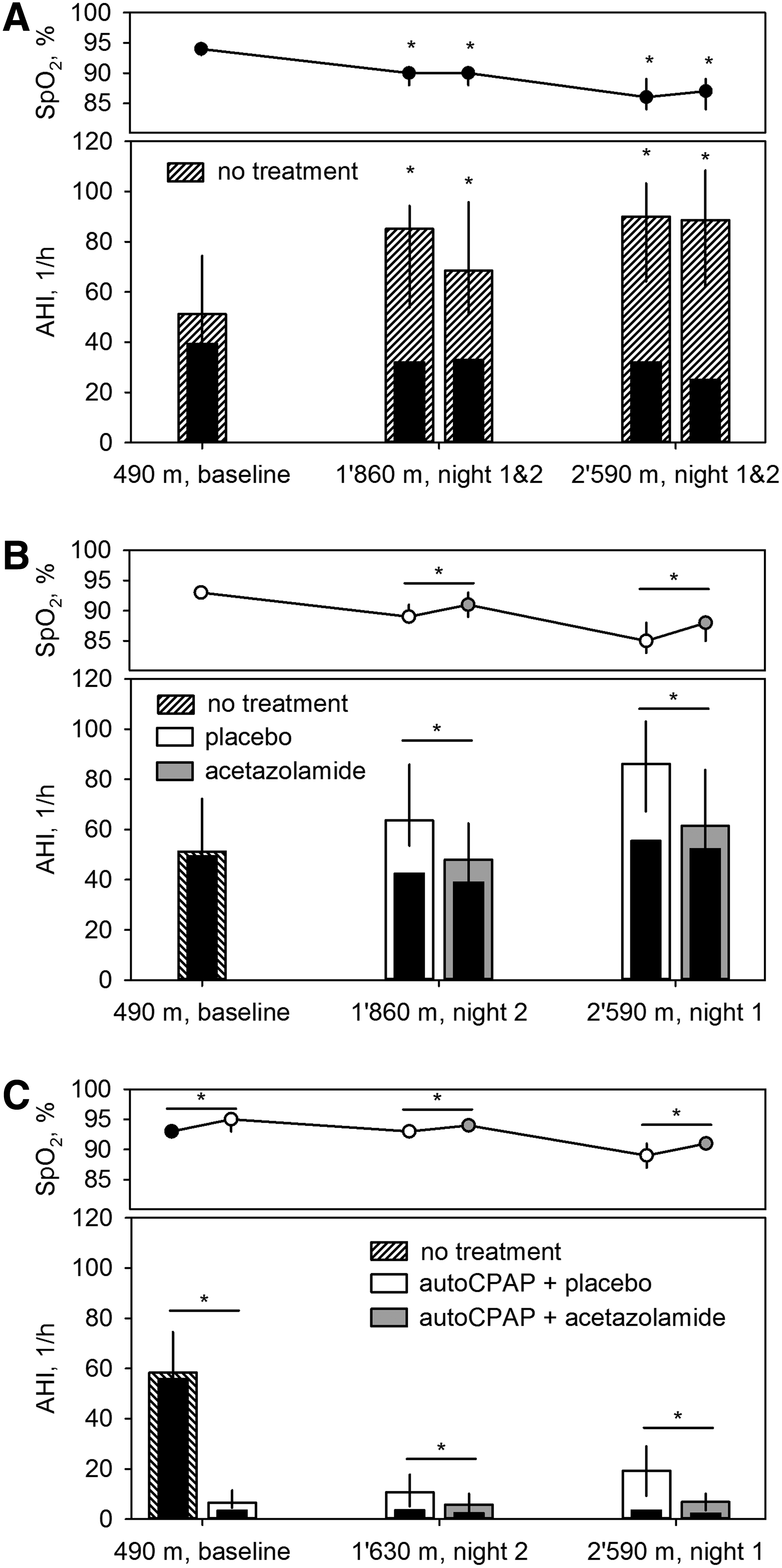
Summary of three trials performed in lowlanders with OSA travelling to moderate altitude. In the first trial
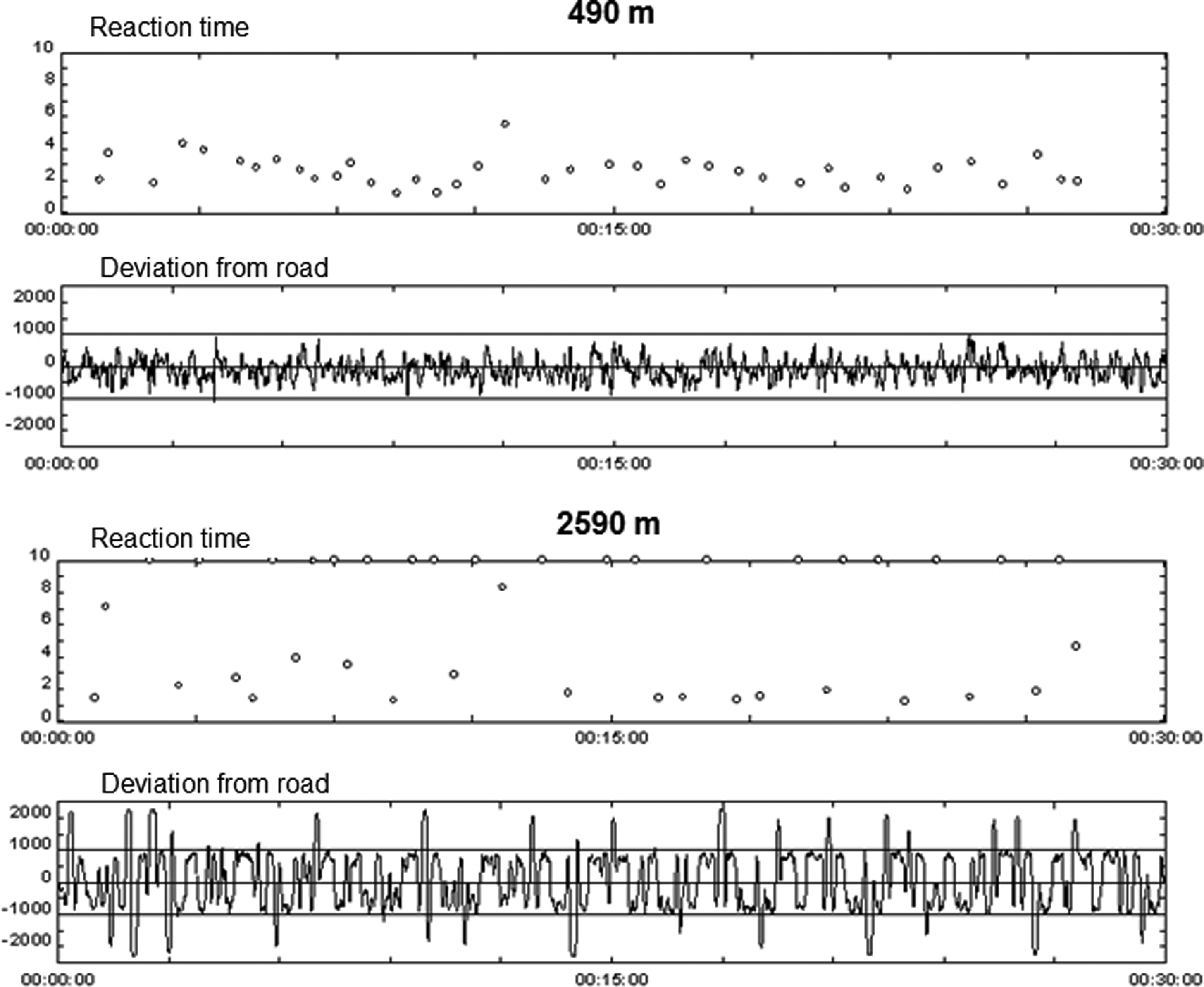
Computer driving simulator test performed by a patient with obstructive sleep apnea at 490 m (upper panel) and at 2590 m (lower panel). The response time to a number appearing in one corner of the computer screen and the distance from the center line of the road were recorded during a 30 min test drive. At 490 m the average reaction time was 2.6 sec and the patient was able to stay near the center line. At 2590 m, the patient missed the presented number several times (reaction time >10 sec) and he crossed the borders of the road several times (the boarders of the simulated road are represented by the horizontal lines above and below the center). Figure reproduced with permission from Nussbaumer-Ochsner et al., 2010.
Magnetic resonance imaging studies in untreated OSA patients at lowlands have demonstrated brain morphologic and functional alterations (Canessa et al., 2011), some of them resembling age-related changes (Macey et al., 2002). Structural deficits were correlated with neurocognitive impairments that improved with CPAP therapy. The described alterations of the brain are thought to be related to intermittent hypoxia with sympathetic overstimulation and impairment of vascular protective mechanisms (Balfors and Franklin, 1994). During altitude travel, OSA patients are exposed to both pronounced intermittent and sustained hypoxia as well as sympathetic excitation that might predispose to cerebral hypoxia.
To investigate whether lowlanders with OSA spending a night at 2590 m experienced cerebral hypoxia, we monitored cerebral oxygenation by transcutaneous near-infrared spectroscopy with sensors placed on the scalp over the prefrontal cortex (Ulrich et al., 2014). In 18 OSA patients participating in this study we found that mean nocturnal cerebral tissue oxygenation was reduced to 59% compared to the corresponding value of 65% at 490 m (Fig. 3). Moreover, in several patients cerebral tissue oxygenation dropped by more than 13% during apnea events. Similar drops in cerebral oxygenation induced by internal carotid artery clamping during neurosurgery have been associated with cerebral ischemia and neurophysiologic impairment (Al-Rawi and Kirkpatrick, 2006). Therefore, the findings (Ulrich et al., 2014) raise concerns that untreated OSA patients, in particular older ones and those with cardiovascular co-morbidity, may be at risk of suffering from cerebral ischemia when staying at altitude.
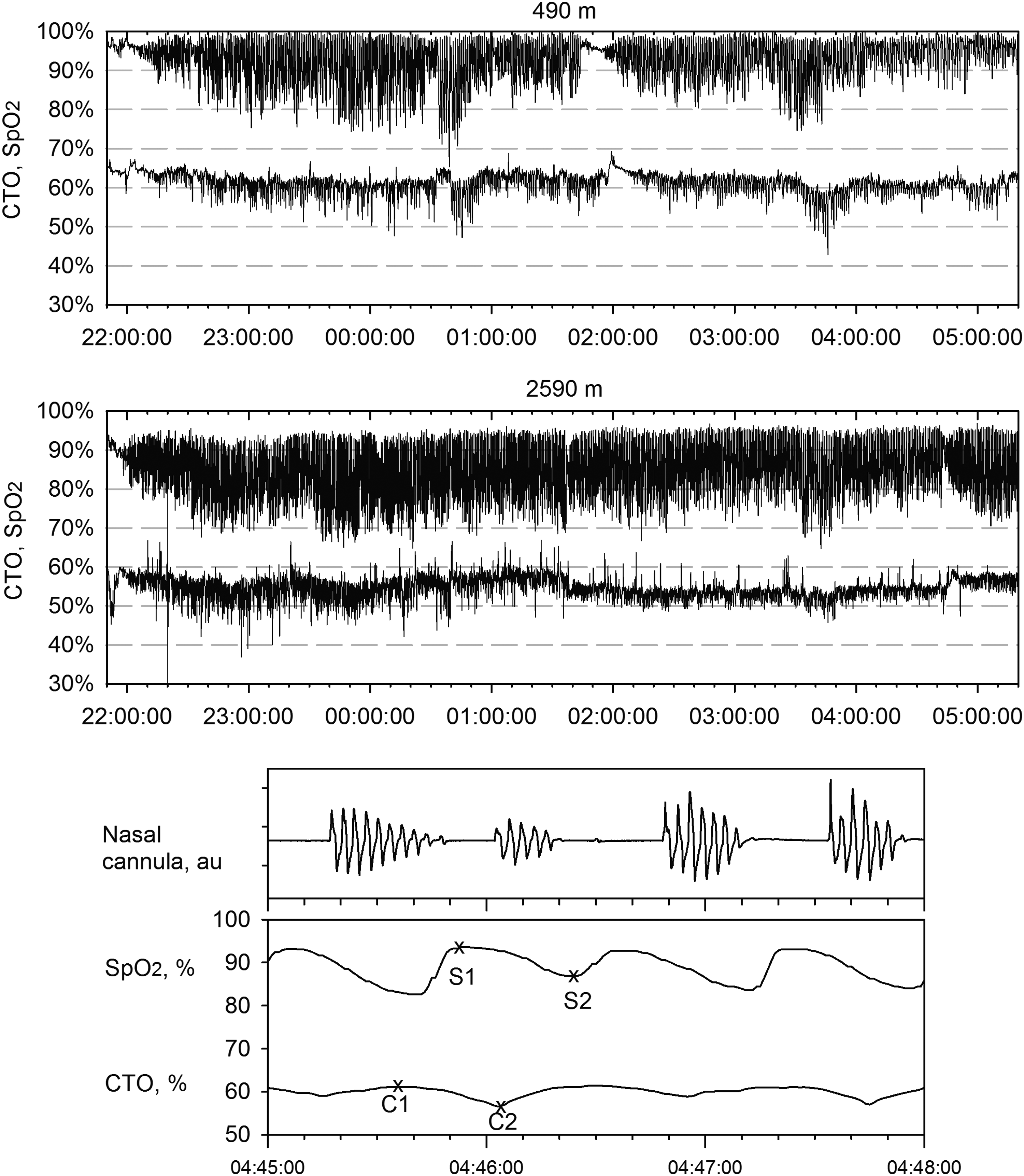
Nocturnal recordings of regional cerebral tissue oxygenation (CTO) by near-infrared spectroscopy and finger pulse oximetry (Sp
How to Treat Patients with OSA at Altitude
Considering the striking effects of altitude exposure in OSA patients, specific treatment seems advisable even during short altitude sojourns as reviewed recently in this journal (Latshang and Bloch, 2011) and graphically illustrated in Figure 1, panels B and C.
As CPAP therapy is not feasible for mountaineers staying overnight in a tent or in a mountain hut, we performed a first randomized, placebo-controlled, double-blind trial evaluating the efficacy of acetazolamide (250 mg twice a day) in improving nocturnal oxygenation and sleep apnea in 45 lowlanders discontinuing their CPAP therapy during a stay at 1860 and 2590 m, respectively (Nussbaumer-Ochsner et al., 2012a). We found that acetazolamide improved mean nocturnal oxygen saturation and the AHI compared to placebo (Fig. 1, panel B). It also improved sleep efficiency, and subjective insomnia, and prevented an excessive rise in blood pressure at altitude. The effects of acetazolamide on sleep apnea were related to a stimulation of ventilation resulting in hypocapnia while the apnea threshold for CO2 was reduced to a similar degree, thereby maintaining an unchanged CO2 reserve (Fig. 4). Despite the acetazolamide-induced hypocapnia, near-infrared spectroscopic studies did not show any evidence of impaired cerebral autoregulation (Ulrich et al., 2014). Based on these data, we concluded that OSA patients may benefit from acetazolamide treatment during an altitude sojourn if CPAP therapy is not feasible.

Mechanisms of central apnea reduction by acetazolamide based on data obtained in patients with obstructive sleep apnea at 2590 m. The diagram illustrates the hyperbolic relationship between alveolar ventilation (V'A) and alveolar PCO2 (PACO2) according to Dempsey et al., 2004). The eupneic PetCO2 on placebo (37 mmHg) was taken as the surrogate of eupneic PACO2 with corresponding V'A defined as 100%. PetCO2 of 31 mmHg at V'A=0 is the apnea threshold. Assuming an increase in metabolic rate on acetazolamide (by an arbitrary amount of 10%) related to hyperventilation, a second metabolic hyperbola was constructed (dashed line). The corresponding eupneic PetCO2 (35 mmHg) and apnea threshold PetCO2 (27 mmHg) are also shown. Driving PetCO2 from the eupneic level to the apnea threshold requires a greater ventilatory overshoot on acetazolamide (increase in V'A from 116% to 155%) than on placebo (from 100% to 123%). This is because the eupneic PetCO2 on acetazolamide is positioned more to the left to a steeper position on the metabolic hyperbola, while the CO2 reserve (difference between eupneic and apneic PetCO2) is similar to that on placebo. The slope of the lines connecting the apnea threshold with the corresponding eupneic PetCO2 reflects the ventilatory sensitivity to CO2 below eupnea which is similar on acetazolamide and on placebo. Figure reproduced with permission from Nussbaumer-Ochsner et al., 2012a.
In the studies using acetazolamide alone, breathing disturbances were not completely suppressed at altitude (Fig. 1, panel B). Therefore, we evaluated whether combined treatment with acetazolamide and nocturnal CPAP using computer controlled mask pressure adjustments (autoCPAP) would provide optimal control of sleep apnea at altitude. In a randomized, placebo-controlled, double-blind trial involving 51 lowlanders with OSA spending nights at 1630 m and 2590 m, respectively, we found that the combined treatment (i.e., acetazolamide 250 mg in the morning and 500 mg in the evening, combined with nocturnal autoCPAP) resulted in a nearly perfect control of sleep apnea and an improved nocturnal oxygen saturation compared to autoCPAP alone (Fig. 1, panel C) (Latshang et al., 2012).
Other favorable effects of the combined treatment compared to autoCPAP alone included an increased sleep efficiency, a greater proportion of deep sleep (NREM stages 3 and 4), and a reduction in the subjective insomnia (Fig. 5). During the stay at 2590 m, using autoCPAP and placebo, patients experienced an increase in weight by approximately 1 kg, and a slight reduction in the forced vital capacity, and in the carbon monoxide diffusing capacity (Latshang et al., 2012). These changes suggested fluid retention with pulmonary fluid accumulation as observed in healthy subjects at 4559 m (Cremona et al., 2002), although different mechanisms have likely been involved.

Effects of acetazolamide combined with continuous positive airway pressure (autoCPAP) in patients with obstructive sleep apnea at altitude. Median differences (and 95% confidence intervals) between outcomes assessed during treatment with acetazolamide and autoCPAP minus corresponding values on placebo and autoCPAP are shown for studies at 1630 m and 2590 m, respectively. AHI, apnea/hypopnea index; Sp
Conversely, combined treatment with autoCPAP and acetazolamide prevented the weight gain and the reduction in vital capacity at 2590 m. When autoCPAP was used with placebo, the mask pressure was adjusted to a higher level at 2590 m compared to 490 m or that with autoCPAP and acetazolamide at 2590 m (median CPAP of 10.0 mbar vs. 8.4 and 8.9 mbar, respectively) (Fig. 5). Correspondingly, the 90th percentile of CPAP was also higher at 2590 (on placebo) compared to 490 m (i.e., 13.0 compared to 11.2. mbar in NREM, and to 12.4 vs. 10.2 mbar in REM sleep). Presumably, in the absence of the diuretic effect of acetazolamide at altitude the computer algorithm of the CPAP device increased the mask pressure in response to a greater tendency for inspiratory flow limitation that was promoted by fluid retention and rostral fluid shift in supine position (Yumino et al., 2010).
Conclusions
The studies performed to date have shown that lowlanders with OSA experience pronounced hypoxemia and exacerbation of breathing disturbances when discontinuing CPAP therapy during a stay at even moderate altitude corresponding to that of many mountain tourist destinations. Although OSA affects persons of all ages, it is more prevalent with advancing age. The same holds true for various other conditions, including cardiovascular diseases. Therefore, older patients with OSA may be particularly susceptible to the effects of hypobaric hypoxia at altitude that induces an elevated sympathetic tone, systemic hypertension, cardiac arrhythmia, and impaired cerebral oxygen delivery. Based on available evidence patients with OSA should be encouraged to use CPAP therapy when sleeping at altitude if this is feasible. Acetazolamide may serve as an adjunct that provides even better control of breathing disturbances than CPAP alone, and this drug is better than no treatment at all if CPAP cannot be used. Whether mandibular advancement devices are effective alternatives for treatment of OSA at altitude and whether acclimatization over a few days improves breathing disturbances requires further study.
Footnotes
Acknowledgments
Grant support has been received from Swiss National Science Foundation, Zurich Lung Ligue, Zurich Center for Interdisciplinary Sleep Research, University of Zurich, Switzerland.
Author Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose.