
Abstract
Abstract
Richalet, Jean-Paul, and François J. Lhuissier. Aging, tolerance to high altitude, and cardiorespiratory response to hypoxia. High Alt Med Biol. 16:117–124, 2015.—It is generally accepted that aging is rather protective, at least at moderate altitude. Some anecdotal reports even mention successful ascent of peaks over 8000 m and even Everest by elderly people. However, very few studies have explored the influence of aging on tolerance to high altitude and prevalence of acute high altitude related diseases, taking into account all confounding factors such as speed of ascent, altitude reached, sex, training status, and chemo-responsiveness. Changes in physiological responses to hypoxia with aging were assessed through a cross-sectional 20-year study including 4675 subjects (2789 men, 1886 women; 14–85 yrs old) and a longitudinal study including 30 subjects explored at a mean 10.4-year interval. In men, ventilatory response to hypoxia increased, while desaturation was less pronounced with aging. Cardiac response to hypoxia was blunted with aging in both genders. Similar results were found in the longitudinal study, with a decrease in cardiac and an increase in ventilatory response to hypoxia with aging. These adaptive responses were less pronounced or absent in post-menopausal untrained women. In conclusion, in normal healthy and active subjects, aging has no deleterious effect on cardiac and ventilatory responses to hypoxia, at least up to the eighth decade. Aging is not a contraindication for high altitude, as far as no pathological condition interferes and physical fitness is compatible with the intensity of the expected physical demand of one's individual. Physiological evaluation through hypoxic exercise testing before going to high altitude is helpful to detect risk factors of severe high altitude-related diseases.
Introduction
A
These observations might be considered paradoxical since aging is generally associated with decreased physical and cognitive performance, blunting of physiological responses to environmental stimuli.
In a prospective study conducted in a cohort of 1326 persons, we showed that the risk of severe high altitude illness (SHAI: severe high altitude illness=severe acute mountain sickness, high altitude pulmonary and cerebral edema) decreased with increasing age (Richalet et al., 2012). In a multivariate analysis, young age (<46 years) was associated with increased risk of SHAI. However, the main physiological risk factor of SHAI was established to be the peripheral chemosensitivity to hypoxia, evaluated by the ventilatory response to a hypoxic challenge at moderate exercise. A score was established to predict individual susceptibility to SHAI (Canouï-Poitrine et al., 2014), with maximal number of 11 points: history of SHAI (2.5 points), rapid ascent (>400 m/night) (2 points), history of migraine (1.5 points), geographical location (Aconcagua, Ladakh, Mt. Blanc) (1 point), age <46 yrs (0.5 point), regular endurance physical activity (0.5 point), low ventilatory response to hypoxia at exercise (<0.68 L/min/kg) (3 points), low cardiac response to hypoxia at exercise (<0.72 b/min/%) (1 point). Age ≥46 yrs appears in this score as a protective factor in subjects who have a previous experience of high altitude exposure (Canouï-Poitrine et al., 2014).
When comparing specifically, in this cohort, the incidence of severe AMS, peripheral edema, high altitude pulmonary edema (HAPE), and high altitude cerebral edema (HACE) in three different age categories of approximately equal dimension (less than 36 years old, between 36 and 52 years old, and over 52 years old), we observed a significant decrease in AMS and peripheral edema and a tendency for a decrease in HAPE and HACE (Fig. 1). It is important to note that speed of ascent and maximal altitude reached during the stay at high altitude were not significantly different between younger and older categories (number of subjects with speed of ascent >400 m: 31% and 29%; maximal altitude reached: 5070±1113, 4996±847 m, respectively, in the <32 years and >52 years groups) , suggesting that these two important determinant factors for AMS do not explain for the age effect.
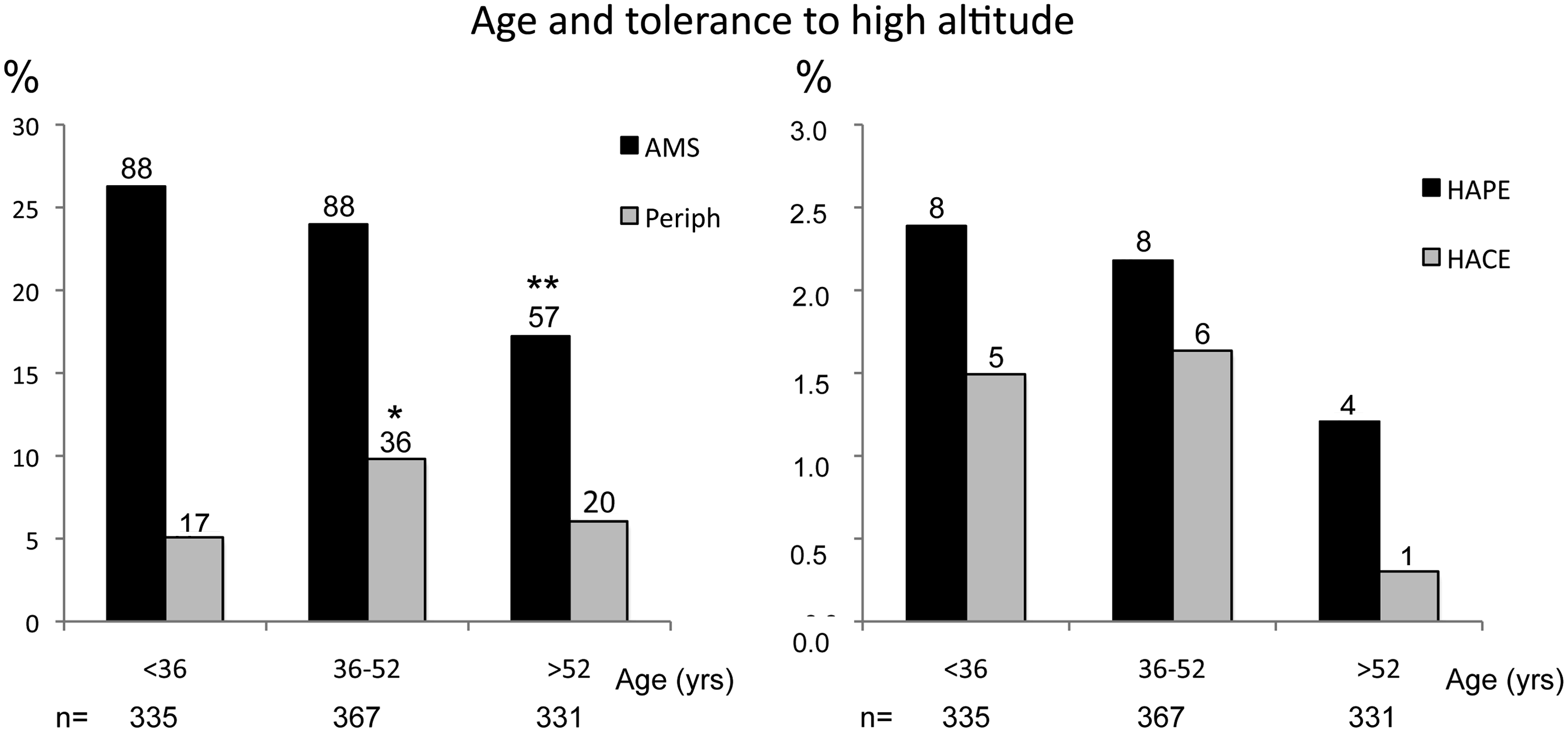
Prevalence of high altitude sickness in a group of 1033 subjects, free of acetazolamide, as a function of age. AMS, acute mountain sickness; HAPE, high altitude pulmonary edema; HACE, high altitude cerebral edema; Periph, peripheral edema. On the top of each bar: absolute number of subjects in each group. Comparison of prevalence between age groups (Chi2): **p=0.015; *p=0.034. Adapted from Richalet et al., 2012.
As ventilatory response to hypoxia is a determinant factor of susceptibility to SHAI, we hypothesized that aging could be a protective factor through changes in ventilatory or cardiac responses to hypoxia. Men and women do not age in the same way and very little is known about the influence of menopause on the ventilatory response of women to exercise or hypoxia. However, an improved ventilatory response to hypoxia (HVR) was described during the luteal phase (Schoene et al., 1981; White et al., 1983) and pregnancy (Moore et al., 1987; Hannhart et al., 1989), suggesting that sex hormones might also influence the tolerance to hypoxia. Training status may also interfere with the tolerance to hypoxia since endurance trained athletes show an exacerbated exercise-induced arterial desaturation in hypoxic conditions (Mollard et al., 2007). Moreover, endurance training seems to increase the risk of developing SHAI (Richalet et al., 2012; Canouï-Poitrine et al., 2014).
Our objective was therefore to explore the effect of aging on the cardiac and ventilatory responses to hypoxia at exercise, taking into account the sex and the level of endurance training (Lhuissier et al., 2012). Subjects went through a routine hypoxic exercise test that has been described in details elsewhere (Richalet et al., 2012; Canouï-Poitrine et al., 2014). Ventilatory (HVRe) and cardiac (HCRe) responses to hypoxia at exercise were calculated, as well as desaturation at exercise (ΔSae). First, in a cross-sectional study, we evaluated the influence of age on the physiological response to hypoxia in a group of 4675 subjects. Second, we performed a longitudinal study in a subset of 30 subjects who underwent twice the same test, at a mean interval of 10.4 years.
Cross-Sectional Study
During a 20-year period, from 1992 to 2011, 4788 patients came to the altitude medicine consultation at Avicenne hospital (Bobigny, France) before a sojourn of at least 3 days above 4000 m of altitude with overnight sleeping above 3500 m. After excluding patients taking beta-blockers or hormonal treatment for menopause, 4675 persons (14–85 years old, 2789 men, 1886 women) who came for the first time to the consultation were included in the study. Results are shown in Tables 1 and 2 and in Figures 2 to 4.
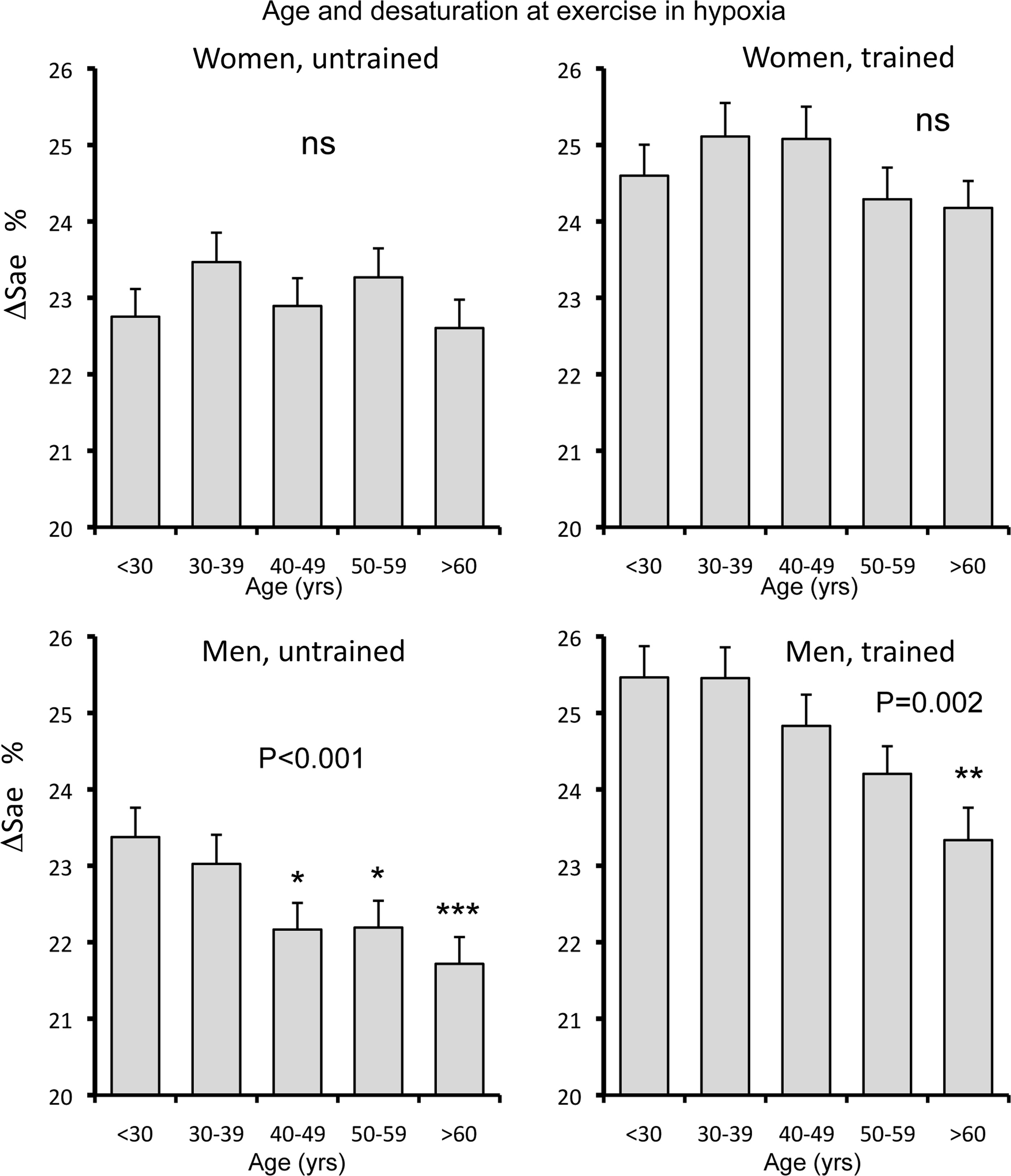
Variation of hypoxia-induced desaturation at exercise (ΔSae, %) in untrained (n=1411) and trained (n=475) women and untrained (n=1709) and trained (n=1080) men as a function of age categories. P are obtained from a 2-way ANOVA (age x training status). The p values on the figure refer to the age effect. A post-hoc test with Bonferroni correction was applied to compare age categories (reference: <30 years old): *p<0.05, **p<0.01, ***p<0.001. Training effect: women, p<0.001; men, p<0.001. Values are mean±SEM. Adapted from Lhuissier et al., 2012.
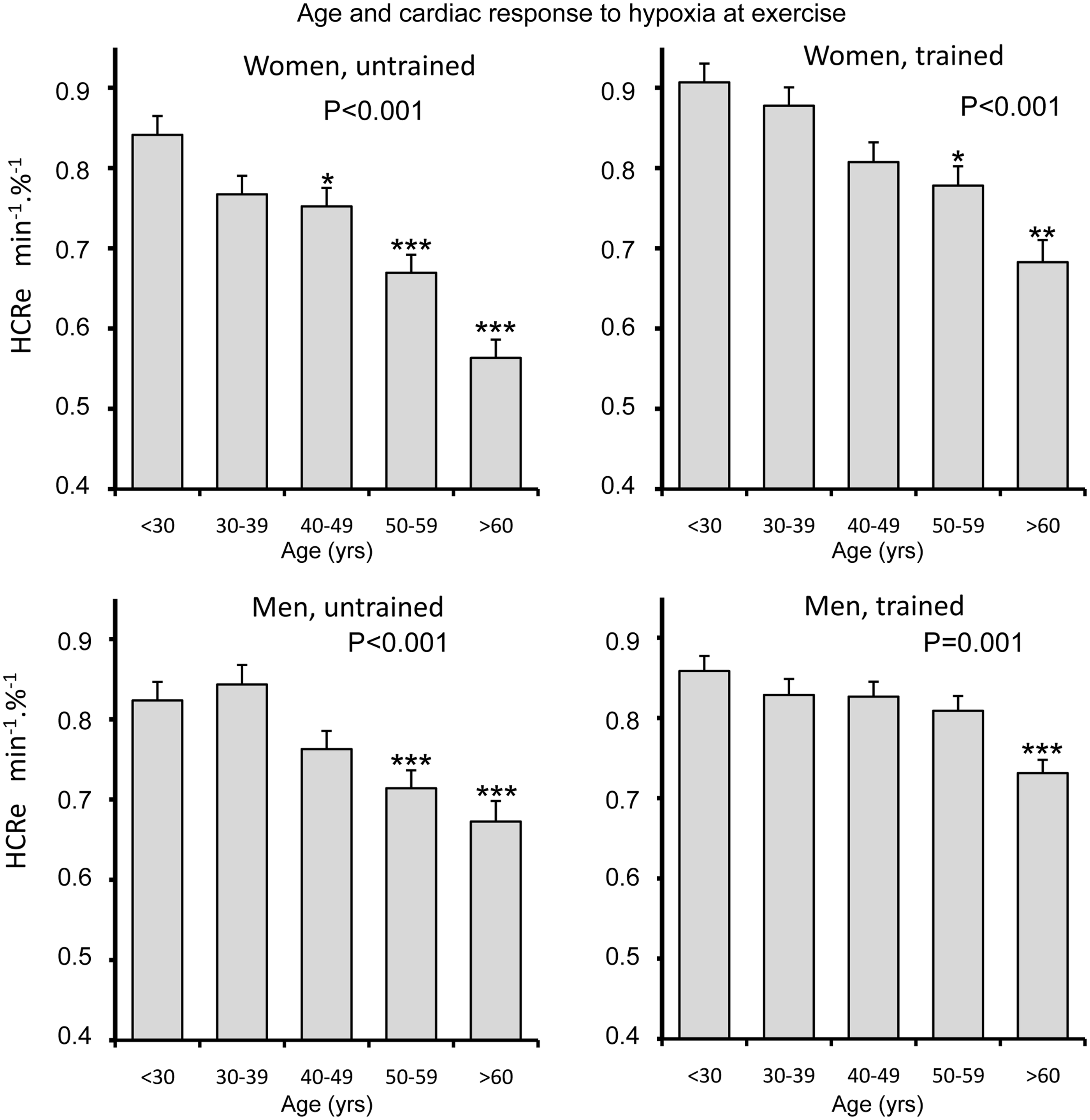
Variation of cardiac response to hypoxia at exercise (HCRe, min−1.%−1) in untrained (n=1411) and trained (n=475) women and untrained (n=1709) and trained (n=1080) men as a function of age categories. P are obtained from a two-way ANOVA (age x training status). The p values on the figure refer to the age effect. A post-hoc test with Bonferroni correction was applied to compare age categories (reference: <30 years old): *p<0.05, **p<0.01, ***p<0.001. Training effect: women, p<0.001; men, p<0.001. Values are mean±SEM. Adapted from Lhuissier et al., 2012.
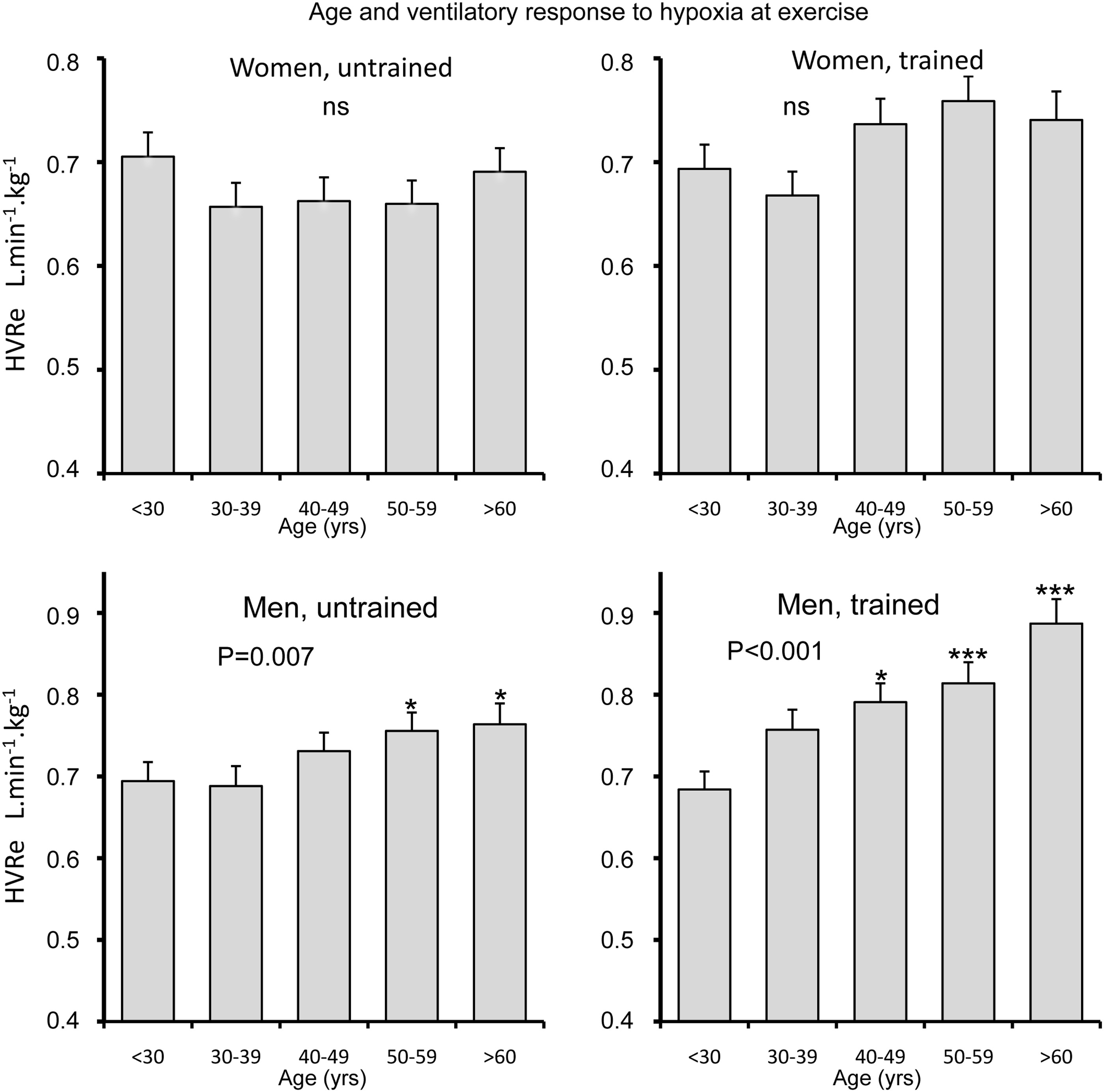
Variation of ventilatory response to hypoxia at exercise (HVRe, L.min−1.kg−1) in untrained (n=1411) and trained (n=475) women and untrained (n=1709) and trained (n=1080) men as a function of age categories. P are obtained from a two-way ANOVA (age x training status). The p values on the figure refer to the age effect. A post-hoc test with Bonferroni correction was applied to compare age categories (reference: <30 years old): *p<0.05, **p<0.01, ***p<0.001. Training effect: women, p=0.013; men, p<0.001. Values are mean±SEM. Adapted from Lhuissier et al., 2012.
Mean±standard deviation; ΔSae, desaturation at exercise; HCRe, HVRe, cardiac and ventilatory response to hypoxia at exercise; p, Student t-test. Adapted from Lhuissier et al., 2012.
Mean±standard deviation. Interaction between sex and menopause/age by a TWO-way ANOVA. ΔSae, desaturation at exercise; HCRe, HVRe, cardiac and ventilatory response to hypoxia at exercise. Adapted from Lhuissier et al., 2012.
Most variables are significantly related to age, sex, and training status. The hypoxia-induced desaturation at exercise (ΔSae) was similar in men in women. ΔSae decreased with age in men and increased with training both in men and women (Fig. 2). Cardiac response to hypoxia at exercise (HCRe) was slightly higher in men than in women (Table 1), decreased with age in all categories but less in trained than in untrained subjects (Fig. 3). Ventilatory response to hypoxia at exercise (HVRe) was higher in men than in women (Table 1), increased with age only in men and more in trained than untrained subjects (Fig. 4). Altogether, the most significant observations were a decrease in heart rate response with aging in both genders, blunted by training, and an increase in the ventilatory response with aging only in men, and exacerbated by training.
The effects of menopause on cardio-respiratory variables are illustrated in Table 2. Differential effects of menopause/age were found between men and women in some variables, suggesting that menopause is the cause of these changes. For many variables, the changes were different between trained and untrained post-menopausal women. The decrease with aging in hypoxia-induced desaturation at exercise (ΔSae) was blunted in post-menopausal women. The decrease with aging in cardiac response to hypoxia at exercise (HCRe) was exacerbated in untrained post-menopausal women. The increase with aging of the ventilatory response to hypoxia at exercise (HVRe) observed in men was absent in untrained post-menopausal women.
To conclude, adaptive responses observed in men (increase in ventilation and O2 saturation, decrease in heart rate) with aging were less pronounced or absent in untrained post-menopausal women but conserved in trained ones.
Longitudinal Study
From this cohort of patients coming to the consultation, we extracted a subgroup of 30 subjects (21 men, 9 women) who came twice at a mean interval of 10.4 years (5 to 19 years) and performed the same routine evaluation. Physiological variables before and after a mean period of 10.4 years are shown in Table 3. Between the two evaluations, ΔSae insignificantly decreased, HCRe decreased and HVRe increased. A significant difference between men and women was only found for HVRe. Altogether, we found in the longitudinal study in 30 subjects studied at a 10.4-year interval the same overall results as in the cross-sectional study in 4675 subjects: the ventilatory response to hypoxia and exercise slightly improved, while the cardiac response was blunted. Changes were similar in men and women.
Mean±standard deviation. ΔSae,desaturation at exercise; HCRe, HVRe, cardiac and ventilatory response to hypoxia at exercise; P time, comparison between first and second evaluation; P sex, comparison between men and women. No significant interaction was found between time and sex factors. Adapted from Lhuissier et al., 2012.
To summarize, a cross-sectional analysis in a cohort of 4675 subjects from 14 to 85 years of age and a longitudinal study in a group of 30 subjects explored at two occasions separated by a mean gap of 10.4 years gave similar results and suggest that aging is associated with a blunting of cardiac chronotropic function and an increase in ventilatory response leading to maintenance of arterial O2 saturation both at rest and at submaximal exercise in normoxia and hypoxia. In post-menopausal women, the adaptive responses to exercise and hypoxia are less pronounced or absent when compared to men at the same age but endurance training can partly reverse these menopause effects.
Aging and Ventilatory Response
The influence of aging on ventilatory response to acute hypoxia has been scarcely studied in humans. The previous protocols compared young (20–40 years) to older (60–85 years) groups and always included a limited number of subjects, between 15 (Vovk et al., 2004) and 112 (Garcia-Rio et al., 2007). Most of these studies used isocapnic hypoxia and all focused on response at rest. Authors used different methods to explore HVR: the relation
The increase in HVR in elderly is consistent with the observation that Sa
Since HVR depends on the carotid bodies (CBs), some authors studied the modifications of their morphology with age. Degenerative changes have been observed in rats and humans (Heath, 1991). Some authors have pointed out the contrast between morphometric and functional studies (Pokorski et al., 2004; Pokorski and Antosiewicz, 2010). They suggested that a smaller number of type I cells in CBs could be sufficient to sustain a functional activity and/or that the impairment in CB function could lead to compensatory mechanisms in brain respiratory areas.
Menopause and Ventilatory Response
The enhancement of HVR with aging is blunted in women compared to men (Lhuissier et al., 2012). Very little is known about the effect of menopause on these adaptations. Pokorski compared HVR in old and young women and found no difference (Pokorski and Marczak, 2003). Wenninger studied the effects of age and gender on HVR in rats and reported a greater HVR in females than in males at old age (Wenninger et al., 2009). Regardless of age, a majority of authors found no difference in HVR between genders (Sajkov et al., 1997; Teppema and Dahan, 2010). In women, an enhancement of HVR was described during the luteal phase compared to the follicular phase (Schoene et al., 1981; White et al., 1983) and during pregnancy (Moore et al., 1987; Hannhart et al., 1989). These observations appear rational since stimulating effects of male and female sex hormones on ventilation, HVR, and CBs sensitivity to hypoxia were reported in cats (Hannhart et al., 1989; Tatsumi et al., 1994), and in humans for testosterone (White et al., 1985). Thus, a blunted increase of HVR with age in menopausal women appears to be consistent with their relative lack of female sex hormones.
Aging and Cardiocirculatory Responses
Concerning cardiac response to exercise and hypoxia, our data indicate that older subjects have a lower HR at submaximal exercise (Lhuissier et al., 2012). At rest, the decrease in HR with age in both normoxia and hypoxia is consistent with the reduction in intrinsic HR and β-adrenergic responsiveness, which might also be responsible for the decreased maximal HR with aging (Christou and Seals, 2008). The blunted cardiac responses to hypoxia observed in our study at exercise, and previously reported at rest (Kronenberg and Drage, 1973), can be related to the same physiological mechanisms of blunted adrenergic activity (Favret and Richalet, 2007).
The association of an increased ventilatory response and a decreased cardiac response to hypoxia in moderate exercise conditions is optimal for the O2 transfer in the lungs through increased alveolar PO2 and blood transit time (Fig. 5). Therefore, the diffusion limitation that may account for the greater exercise-induced desaturation in hypoxia in young and trained subjects (McKenzie, 2012) is less prominent in elderly and less trained subjects. Conversely, at maximal exercise in hypoxic conditions, there would be a clear disadvantage of aging since maximal O2 consumption decreases and muscle mass and power progressively decline (Hawkins and Wiswell, 2003; Tanaka and Seals, 2003).
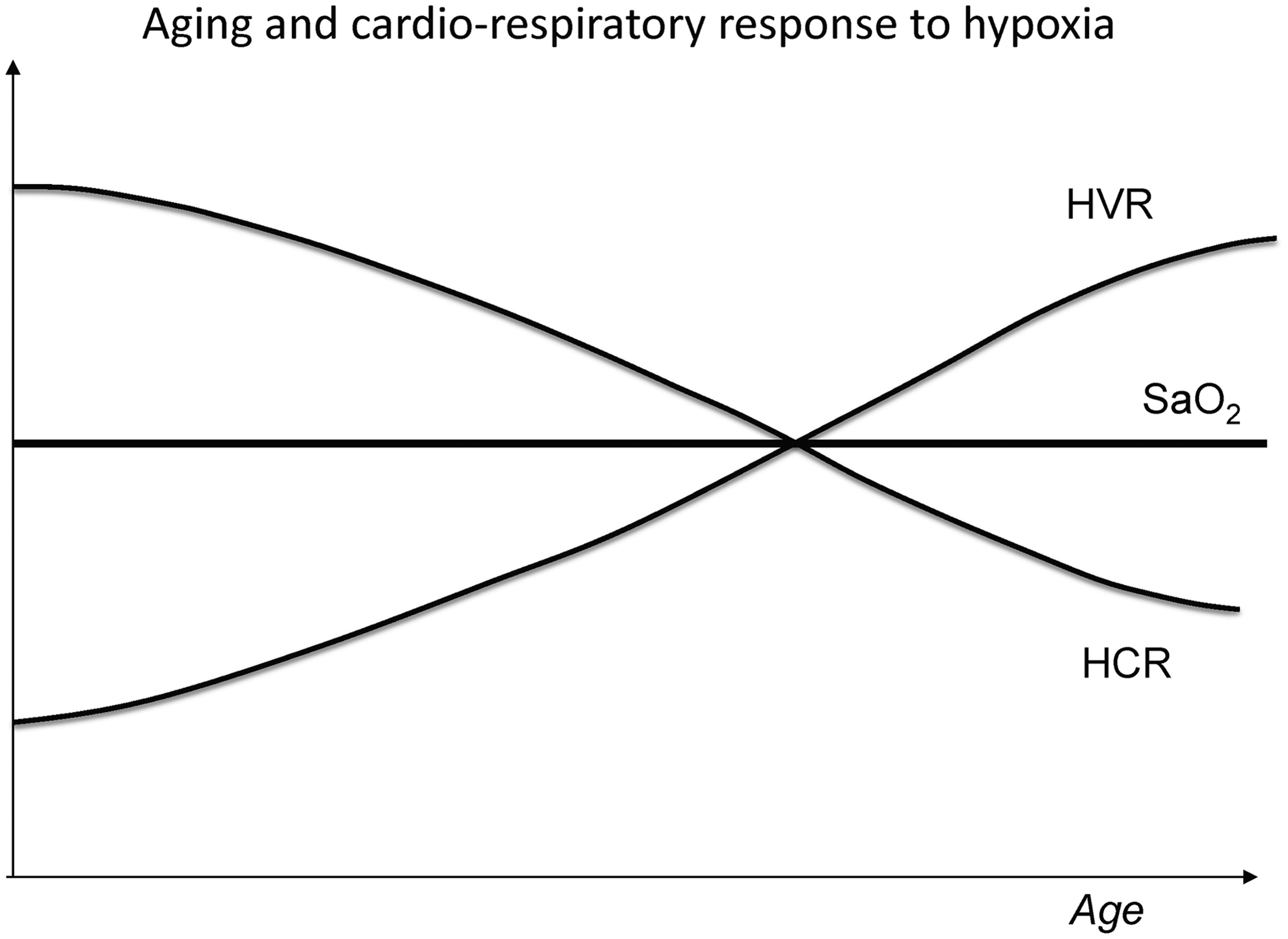
Schematic representation of variation of cardiac (HCR) and ventilatory (HVR) responses to hypoxia and arterial O2 saturation with aging. A higher HVR and a lower HCR will favor O2 uptake in the lungs and allow the maintenance of a normal O2 saturation, at moderate exercise.
Conclusion
In normal healthy and active subjects, aging has no deleterious effect on cardiac and ventilatory responses to hypoxia, at least up to the eighth decade. Epidemiological studies in large cohorts showed that low HCRe, low HVRe, high ΔSae, and younger age are associated with increased risk of SHAI. These observations are probably due to concomitant changes in the physiological parameters that determine the tolerance to altitude hypoxia. In fact, there is an increased HVRe and a decreased ΔSae with aging, allowing elderly to challenge hypoxia similarly to younger ones. It appears that aging is not a contraindication for high altitude, as far as no pathological condition interferes and physical fitness is compatible with the intensity of the expected physical demand of one's individual. It is clear that, as the intensity of exercise comes closer to maximal aerobic power, the physical performance of elderly people is severely impaired. In any case, physiological evaluation through hypoxic exercise testing before going to high altitude is helpful to detect eventual risk factors of severe high altitude related diseases.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.