
Abstract
Abstract
He, Lipeng, Yu Jiang, Hai Su, Juxiang Li, and Xiaoshu Cheng. Vascular endothelial function assessed by postischemic diastolic blood pressure is associated with acclimatization and acute mountain sickness. High Alt Med Biol 17:11–15, 2016.—
Methods:
Forty-two age- and body mass index-matched young male residents at sea level (<400 m) or moderate altitude (1000–2000 m above sea level) were enrolled. All subjects had never been to 3200 m before. Brachial BP was measured at a station at 1380 m altitude before and 1, 5, and 10 minutes after right arm ischemia. AMS score was evaluated after 3-day training at a high altitude of 3200 m.
Results:
In moderate altitude versus sea-level residents: (1) systolic BP curves for both arms overlapped well; (2) mean right arm DBP decline post right arm ischemia was larger, while left arm, which was not subjected to ischemia, did not show DBP decline in either group; and (3) AMS scores were significantly lower (3.19 ± 2.16 vs. 5.52 ± 4.58, p = 0.043) in those residing at moderate altitude compared to those from low altitude. There was a low negative correlation between AMS score and right arm area between curves-DBP (r = −0.320, p = 0.039).
Conclusion:
Moderate altitude relative to sea-level residents had a larger mean postischemic DBP decline in weak but significant association with lower mean AMS score at 3200 m. These data suggest that differences in vascular endothelial function related to altitude of residence persist during travel to high altitude and might contribute to AMS risk.
Introduction
A
It is well known that high-altitude residents have low susceptibility to AMS (Staab et al., 2013; Yan, 2014). The underlying mechanisms involve acclimatization, genetics, and other factors (Wang et al., 2011; Bigham and Lee, 2014), such as the lower carotid wall/lumen ratio reported among highlanders relative to lowlanders in one study (Lewis et al., 2014).
Previous studies suggest an association between AMS and vascular endothelial dysfunction (Maloney et al., 2000; Lewis et al., 2014). In an experimental study, 1 hour of hypoxic exposure induced sustained reduction in flow-mediated dilatation (FMD) among healthy lowlanders, while FMD and endothelial-independent dilatation declined when at high altitude relative to sea level (Lewis et al., 2014).
Although FMD is the most commonly used method to evaluate vascular endothelial function (Corretti et al., 2002), this method requires expensive equipment. The brachial diastolic blood pressure (DBP) decline after 5 minutes of arm ischemia may provide a simple, inexpensive, and highly operational alternative as suggested by a study, in which it positively correlated with arterial dilatation (ΔD/D0) in the FMD test (Hu et al., 2014).
Identification of practical means of AMS risk prediction assessment, which has been the focus of several studies (Song et al., 2013; Canouï-Poitrine et al., 2014; Coustet et al., 2015), has important preventive value. This study therefore tested the hypothesis that postischemic DBP response differs between sea-level residents and moderate-altitude residents when exposed to high altitude, with postischemic DBP decline associated with AMS risk.
Participants and Methods
The proposal and consent procedures of this study were approved by the Ethics Committees of the Second Affiliated Hospital of Nanchang University. After explaining the value and procedure of this study, all participants provided verbal informed consent for noninvasive BP measurement before and after 5 minutes of arm ischemia.
Participants
In March 2015, 42 healthy young males who had undergone physical, electrocardiographic, and routine blood chemistry examination were enrolled and evenly assigned according to the original place of residence to either a sea-level group (i.e., <400 m above sea level) or a moderate-altitude (i.e., 1000–2000 m above sea level) group. The young males in the two groups had similar age and body mass index (BMI) distributions, and all subjects had never been to 3200 m before.
Methods
The baseline systolic blood pressure (SBP) (124.2 ± 9.6 and 121.4 ± 9.6 mmHg) and DBP (70.5 ± 7.7 and 68.7 ± 10.2 mmHg) were numerically slightly lower in the moderate-altitude group, and distributions of other parameters were not significantly different between groups (Table 1).
BMI, body mass index; DBP, diastolic blood pressure; HR, heart rate; SBP, systolic blood pressure; SpO2, oxyhemoglobin saturation.
The study phases are schematized in Figure 1. All participants stayed at a station at an average altitude of 1380 m for 4 days for acclimatization. On the day before transitioning to a training base at 3200 m, fasting venous blood was sampled for routine hematology, liver and renal function tests, lipid profiles, and levels of creatine kinase (CK) and its myocardial isoenzyme (CK-MB). Body height and weight, BP and heart rate, and oxyhemoglobin saturation (SpO2, Fingertip Oximeter prince-100B; Shenzhen Creative Industry Co., Ltd.) were measured. Anxiety score was evaluated using a Self-Rating Anxiety Scale SAS (Zung, 1971), and BP examination was performed.

Study design.
Three-day physical training was conducted at a training base located at an altitude of 3200 m. During the said period, subjects regularly received training on hand-to-hand combat for 5 hours daily and climbed a mountain up to 4300 m with a 20 kg load for 20 minutes. At the afternoon of the third day, the subjects returned to the station by an automobile. After arriving at the station, the plateau response scale (AMS score) was evaluated based on the classification and diagnostic criteria of high-altitude disease in China.
The Chinese AMS score was calculated as follows: according to their severity, headache was assigned 1, 2, 4, or 7 points and vomiting was assigned 2, 4, or 7 points, respectively. Other symptoms, such as dizziness/light-headedness, nausea, palpitation, shortness of breath, chest pain, blurred vision, sleeplessness (insomnia), anorexia, abdominal distension, diarrhea, constipation, cyanosis of the lips, lethargy, and numbness of the extremities, were assigned 1 point each if present. Based on total scores, four grades of AMS were devised, namely normal (i.e., no AMS (total score of 1–4 points); mild (total score of 5–10 points); moderate (total score of 11–16 points); and severe (total score of 16 points) (West, 2010).
BP measurement
BP examination was performed in a room at 22°C–24°C. Before BP measurement, participants were asked to empty their bladder and to rest for 10 minutes. Bilateral brachial BP was measured twice and 2 minutes apart using two automated BP measurement devices (HEM-7112; Omron), and their average was recorded as the baseline BP (BPb). After BPb measurement, the cuff on the right arm was inflated to 50 mmHg (sphygmomanometric) above SBP for 5 minutes to block blood flow to the right arm. This means that ischemia only developed in the right arm and not in the left arm.
The cuff then was rapidly deflated, and bilateral BP was measured at 1, 5, and 10 minutes (BPp1, BPp5, and BPp10) after cuff release. The differences between BPb and BPp at different time points were calculated as individual BPb-p. In the present study, the area between the BPb curve as reference and the BPp curve was calculated as the area between curves (ABC)-BP using the cubic spline interpolation method (Purkayastha et al., 2011). The absolute value was expressed as the final value. For example, a DBP curve with more obvious DBP decline after arm ischemia had higher ABC-DBP.
Statistical analysis
Data were analyzed with SPSS 10.0 statistical software (SPSS, Inc., Chicago, IL). Continuous variables are expressed as mean ± SD and were compared using the t-test and analysis of variance (ANOVA) test, as appropriate. The correlation between ABC-BP and AMS score was analyzed by linear regression analysis using the Pearson coefficient. A p value of <0.05 was considered statistically significant.
Results
There were no significant differences between the two groups in BP or other baseline parameters assessed (Table 1).
The bilateral curves of SBP overlapped well, with no significant difference in ABC-SBP between sea-level group and moderate-altitude group. In contrast, the DBP decline, and consequently ABC-DBP, for right arm ischemia were greater for the moderate-altitude group than the sea-level group. However, in the nonischemic left arm, the DBP curves did not show a DBP decline and overlapped well with no significant difference in ABC-DBP between the two groups (Fig. 2 and Table 2).
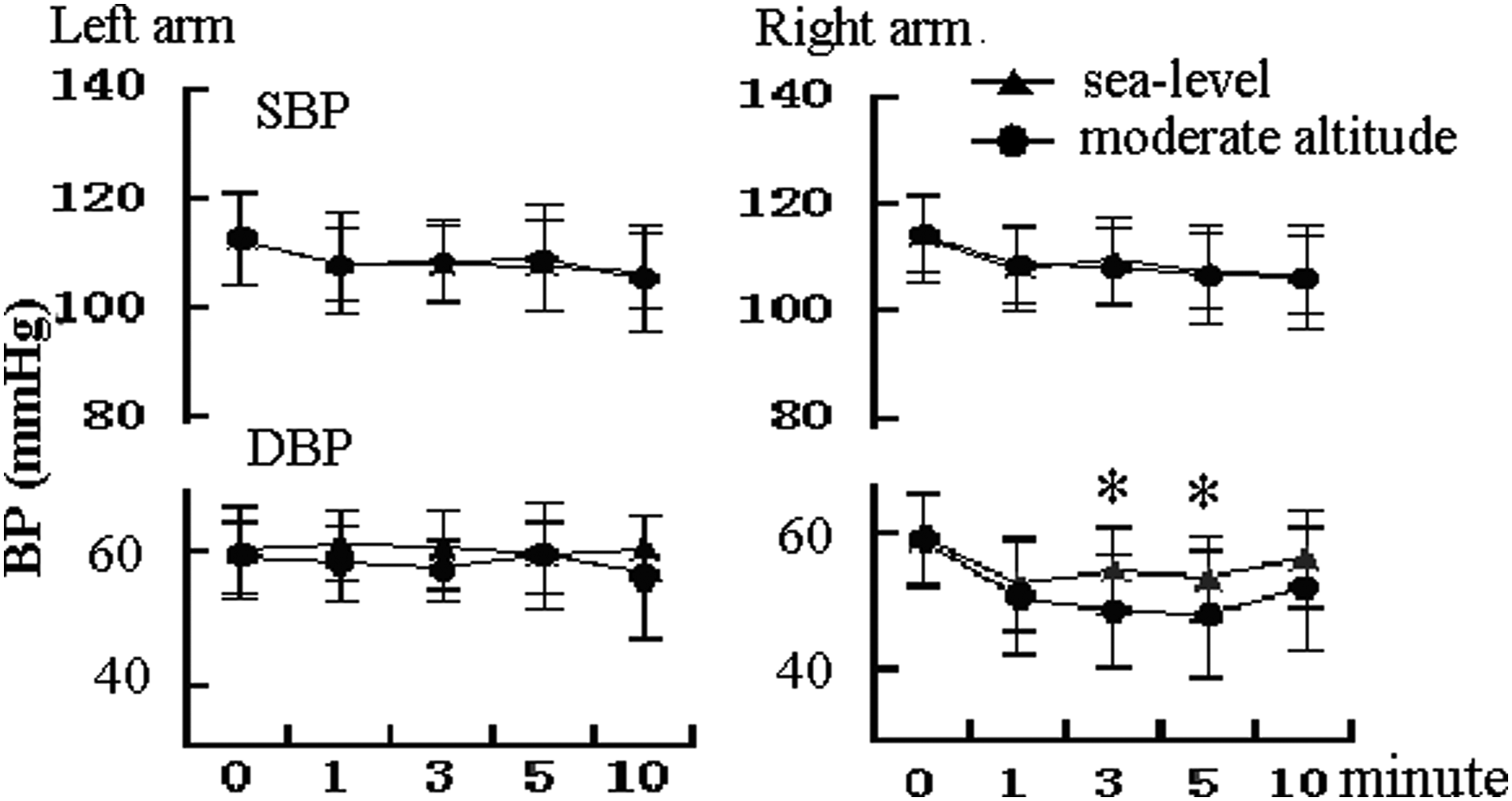
Comparisons of SBP and DBP curves for both arms at 1320 m between the sea-level group and moderate-altitude group. *p < 0.05. DBP, diastolic blood pressure; SBP, systolic blood pressure.
p = compared with sea level.
The AMS score was lower in the moderate-altitude group than in the sea-level group (3.19 ± 2.16 vs. 5.52 ± 4.58, respectively, p = 0.043) (Fig. 3). A weak but statistically significant negative correlation was found between the AMS score and ABC-DBP of the right arm at 3200 m (r = −0.320, p = 0.039) (Fig. 4).
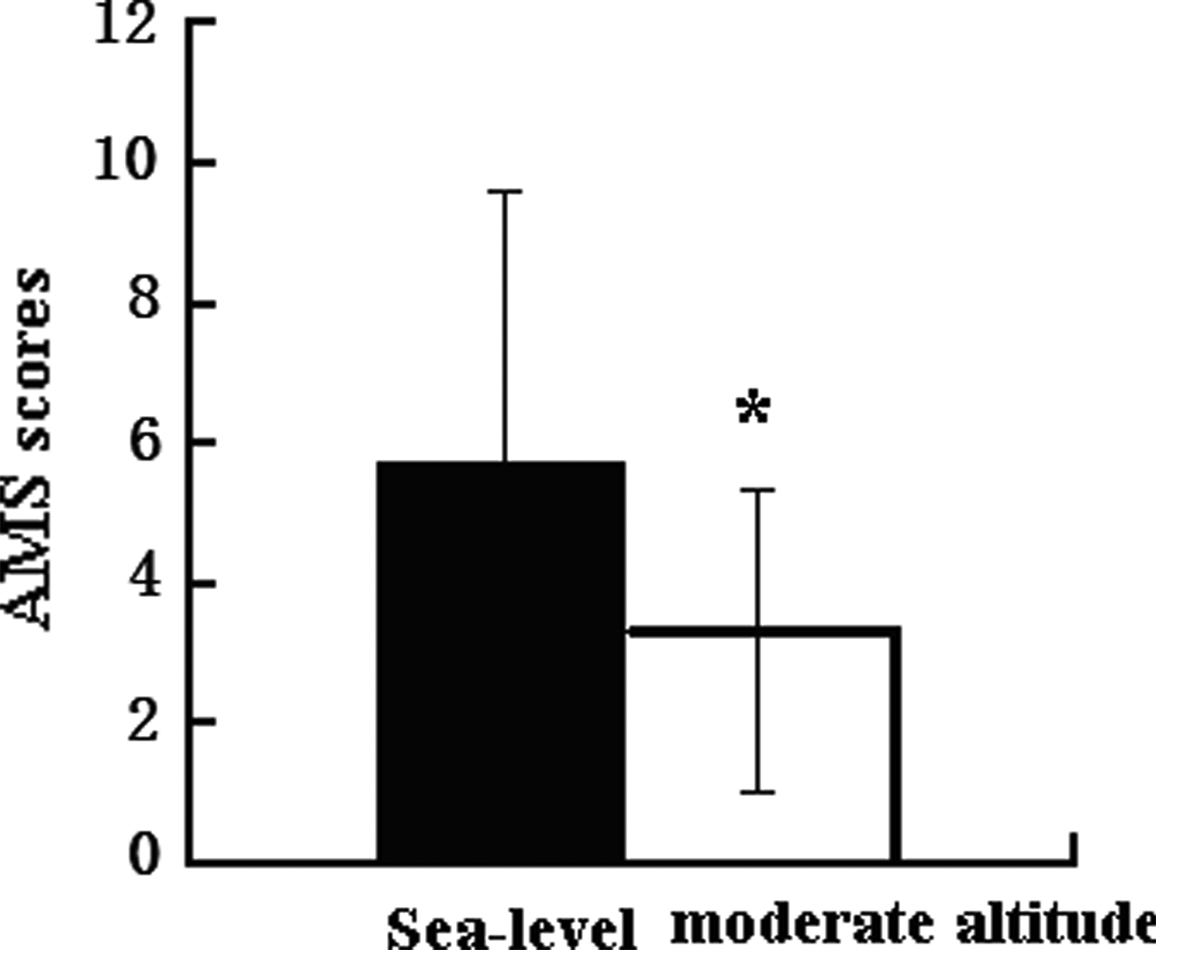
Comparison of AMS scores evaluated at 1320 m after return from high altitude between the sea-level group and moderate-altitude group. *p < 0.05. AMS, acute mountain sickness.
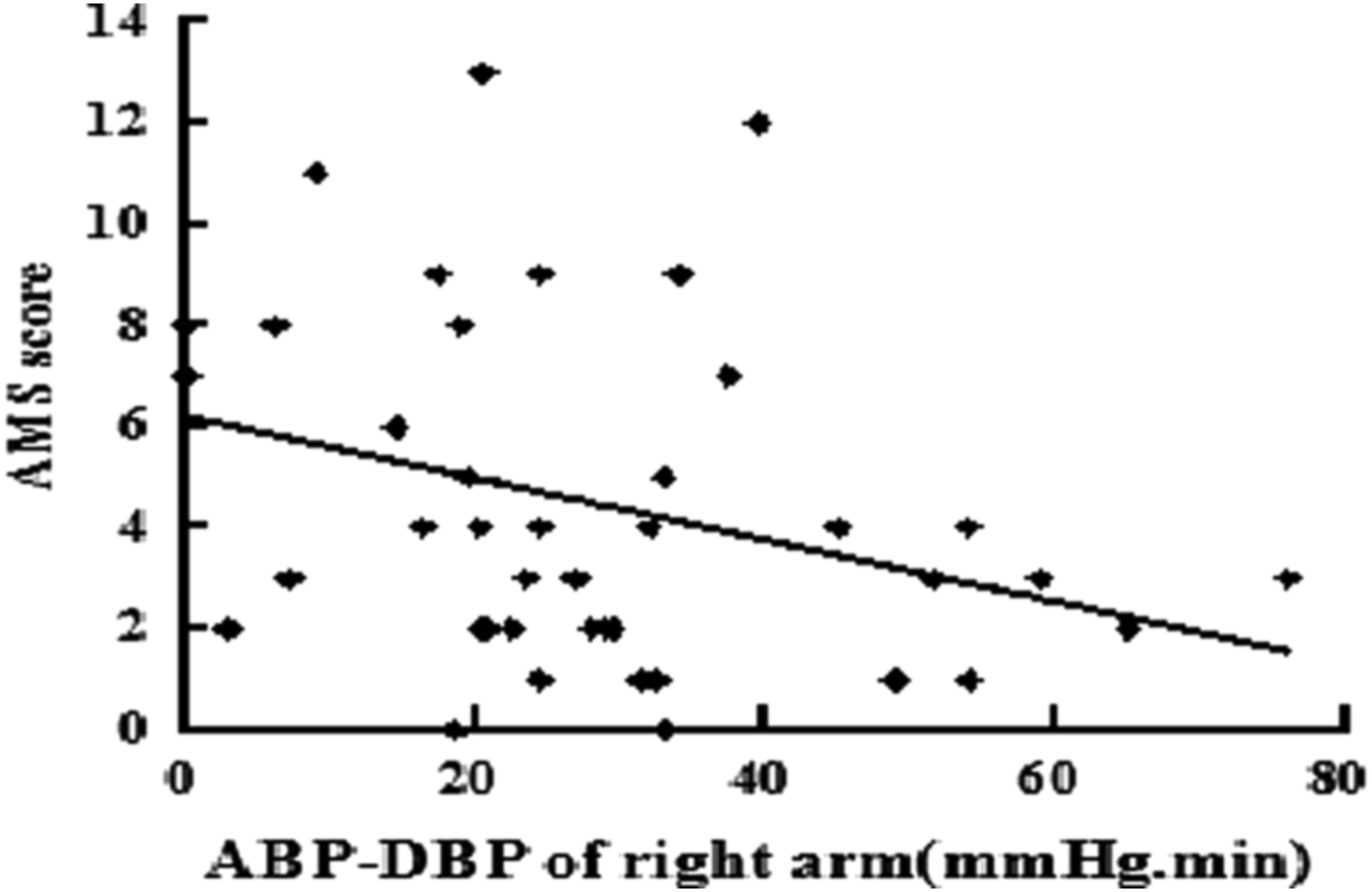
Correlation between AMS score and right arm ABC-DBP. Higher ABC-DBP indicates a more pronounced DBP decline after arm ischemia. ABC-DBP, area between curves-DBP.
Discussion
The present study has three main findings as follows: (1) The study validated that postischemic DBP decline might be useful in evaluating vasodilatation at moderate altitude with well-preserved SpO2, as had been documented for a sea-level area (Hu et al., 2014); (2) Moderate-altitude residents had larger postischemic DBP decline, that is, larger ABC-DBP compared with age- and BMI-matched sea-level residents; and (3) The ABC-DBP in the ischemic right arm negatively correlated with AMS scores, although the correlation was low and insufficient to suggest causality.
The finding first reported in the present study of a more pronounced postischemic DBP decline among moderate-altitude residents than among age- and BMI-matched sea-level residents indicates that the sea-level residents may have less postischemic vasodilatation capacity when staying at 1380 m for 4 days compared with moderate-altitude residents.
Because most factors possibly influencing vascular endothelial function were comparable (Black et al., 2009), the difference in the postischemic DBP decline between the two groups appears mainly dependent on the different residence altitude. The latter finding appears to complement that of previous studies showing an association between vascular endothelial dysfunction and AMS (Maloney et al., 2000), which would suggest that individuals living permanently at sea level do not adapt to high-altitude hypoxia, and present more obvious vascular endothelial dysfunction compared with moderate-altitude residents (Beidleman et al., 2009; Bruno et al., 2014; Lewis et al., 2014). The better adaptive capacity of moderate-altitude residents to hypoxia at 1380 m is related to their acclimatization and genetics. A study found that highlanders (5050 m) had altered arterial structure, with lower carotid wall/lumen ratio; however, whether this is an adaptive or maladaptive response remains to be established (Lewis et al., 2014). The genetics of high-altitude residents also appear different from that of sea-level residents (Wang et al., 2011; Bigham and Lee, 2014). Further studies are warranted to better characterize the influence of diverse factors on AMS development by residents at different altitudes when transitioning to a high-altitude setting.
Lower postischemic DBP as seen in the present study indicates better postischemic vasodilatation or vascular endothelial function; one can therefore posit that vascular endothelial dysfunction may be an important pathological factor in AMS development. Studies have revealed an association between vascular endothelial dysfunction and AMS (Maloney et al., 2000; Buroker et al., 2013); however, there is an apparent contradiction that will require explanation. Further research is needed to better characterize the weak association between AMS and vascular endothelial dysfunction seen in the present study, which is insufficient to suggest causality.
Clinical implication
It is important to find a sensitive predictor for preventing AMS (Song et al., 2013; Canouï-Poitrine et al., 2014; Coustet et al., 2015). In the present study, ABC-DBP after 5 minutes of right arm ischemia showed a negative correlation with AMS scores; however, the correlation was low and insufficient to suggest causality. Further research is warranted to assess the value of postischemic DBP measurement, which is a simple, inexpensive, and highly operational strategy, in studying AMS.
Limitations
The sample size of this study was small, and no severe AMS developed among the young men studied. Thus, better characterization of the clinical value of the apparent association between postischemic DBP decline and AMS is warranted. In addition, the present study did not evaluate the postischemic DBP response when the participants remained at their original place of residence; therefore, the change in postischemic DBP response from sea level to an altitude of 1380 m could not be determined for the sea-level residents.
Conclusion
Despite a preacclimatization period of 4 days at 1380 m, moderate-altitude residents had a larger DBP decline after arm ischemia than sea-level residents, and DBP decline was negatively associated with lower AMS scores. These data suggest that differences in vascular endothelial function related to altitude of residence persist during travel to high altitude and might contribute to AMS risk.
Footnotes
Acknowledgments
This work was supported by the National Science and Technology Infrastructure Program (No. 2013BAI05B10) and the Ministry of Health of the Armed Police Forces (No. WJWSB2012-06).
Author Disclosure Statement
No competing financial interests exist.