
Abstract
Abstract
Boos, Christopher John, David R. Woods, Andrea Varias, Sheryl Biscocho, Peter Heseltine, and Adrian J. Mellor. High altitude and acute mountain sickness and changes in circulating endothelin-1, interleukin-6, and interleukin-17a. High Alt Med Biol. 17:25–31, 2016.—
Introduction
A
Tissue hypoxia is a recognized proinflammatory stimulus and affects endothelial function (Boos et al., 2012; Iglesias et al., 2015). There is accumulating evidence that HA exposure is associated with an inflammatory response and associated endothelial activation/dysfunction (Bruno et al., 2014); however, its link to HA-related illness and AMS remains uncertain (Kleger et al., 1996; Klausen et al., 1997; Swenson et al., 1997, 2002; Zhou et al., 2007; Julian et al., 2011; Mellor et al., 2013; Wojtal et al., 2014).
One of the main constraints of investigating these systemic inflammatory and endothelial responses has been the difficulty in assessing individuals at genuine HA. Many of the published studies have either utilized experimental hypoxia or a single altitude (Hagobian et al., 2006; Wahl et al., 2013; Iglesias et al., 2015). This has limitations as this environment is artificial and involves a shorter period hypoxic exposure leading to fewer cases of AMS than that observed in the real world. In addition, the vast majority of published studies have not adequately, if at all, adjusted for the effects of exercise, which in itself leads to a systemic inflammatory response and endothelial activation.
Candidate plasma markers to assess inflammation and endothelial activation have included interleukin-6 (IL-6), IL-17a, and endothelin-1 (ET-1) (Modesti et al., 2006; Zhou et al., 2007). IL-6 and IL-17a are proinflammatory interleukins released by activated T cells and macrophages. Increased systemic IL-6 and sputum and duodenal IL-17a expression has been observed at HA (Seys et al., 2013; Wojtal et al., 2014). ET-1 is released by the vascular endothelium, including within the cerebral circulation, in response to endothelial injury/activation and is a potent vasoconstrictor and mediator of the hypoxia-driven pulmonary vasoconstriction observed at HA (Pham et al., 2010). ET-1 is itself proinflammatory, triggering IL-6 release and adhesion molecule expression (Böhm et al., 2007). It has been linked to increased vascular permeability and cerebral edema in ischemic brains, suggesting its plausible role in the evolution of AMS and HACE (Moldes et al., 2008).
The measurement of these plasma markers has been hampered by a lack of validated assays with sufficient sensitivity to quantify them in a robust manner, particularly within the normal range. The recent advent of single-molecule counting technology has allowed for improved biomarker quantification within the normal range (Todd et al., 2013; Gottlieb et al., 2015). In this study, we sought to investigate the effects of stepwise increase in terrestrial HA on plasma markers of inflammation (IL-6 and IL-17a) and ET-1 and their relationship with symptoms of AMS.
Methods
Subjects
Forty-eight healthy participants from the UK Defence Medical Services HA expedition to the Cordillera Real region of Bolivia were studied as previously described (Mellor et al., 2013). Confirmation of health status was undertaken following a detailed health questionnaire and assessment by the volunteer's general practitioner. Twenty of these subjects were also studied at sea level (SL) pre and post a 6-hour trek (low altitude to ≤1085 m) undertaken 6 weeks before the expedition. This was undertaken to obtain a clearer picture of the effects of exercise over a typical length trek without the influence of HA and the associated hypoxia. Participants flew from UK to La Paz (altitude 3600 m) (day 0). Studies were performed at three altitudes. There were no constraints on the medications that the subjects took; however, these data were carefully recorded twice daily in their diaries. This was on day 2 at 3833 m following exercise (a trek of 6 hours, 600 m ascent and 16.8 km), day 3 at 3833 m at rest, day 5 at 4450 m following exercise (4 hours, 200 m ascent and 5.6 km), day 6 at 4450 m at rest, day 9 at 5129 m following exercise (4 hours, 400 m ascent and 1.59 km), and day 10 at 5129 m at rest. Samples were collected on rested subjects postexercise on arrival at the new altitude and collected again at rest the following day at the same altitude. Subjects were allowed to complete the trek in their own time.
Physiological data (heart rate, blood pressure, oxygen saturation [SpO2], and AMS scores) were recorded throughout the trek. Venous blood samples were collected post-trek and at rest at the main study altitudes.
Ethics
The study was approved by the UK Ministry of Defence Research and Medical Ethics Committee and conducted according to the standards of the Declaration of Helsinki.
Assay measurements
Venous blood samples were collected from individuals, underwent centrifugation, and immediately stored at −20°C in a portable freezer before shipment back to the UK (within 6 weeks of collection) where long further storage was at −80°C before analysis. Plasma IL-6, IL-17a, and ET-1 were measured with a quantitative fluorescent sandwich immunoassay using laboratory developed tests using single counting technology at Singulex, Inc., (Erenna®) as previously described (Todd et al., 2013; Gottilieb et al., 2015). The ET-1 assay's limits of blank and quantification were 0.07 and 0.33 pg/mL, respectively. Interassay coefficients of variation were 7% at an ET-1 concentration of 1.2 pg/mL and 6% at an ET-1 concentration of 1.8 pg/mL. The IL-6 assay's limits of quantification are 0.08–50 pg/mL with a low-end coefficient of variation of 2%–8% (average 6%). The quantification range for IL-17a is 0.030–20 pg/ml with a low-end coefficient of variation of 1%–13% (average 6%).
Physiological measurements
Resting recordings of oxygen saturation (SpO2) were performed using a Nellcor N-20P pulse oximeter (Nellcor Puritan Bennett, Coventry, UK) following a 15-second continuous recording with the most consistent reading being used. If there was any uncertainty, the measurement was repeated using a different warmed finger. Baseline heart rate and blood pressure were measured using an automated blood pressure cuff with the subject sitting upright for >10 minutes at rest M6 (Omron Healthcare, Milton Keynes, UK).
AMS scores
HA-related symptoms were assessed using the Lake Louis Scoring System twice daily (LLS) (Hackett and Oelz, 1992; Roach et al., 1993). The LLS allocates a score of 0–3 (symptom not present to severe) for symptoms of AMS (headache, gastrointestinal symptoms, fatigue/weakness, dizzy/light-headedness, difficulty sleeping). A total score of ≥3 in the presence of a headache is consistent with AMS and ≥6 with severe AMS.
Statistical methods and power calculations
Data were analyzed using SPSS® statistics version 22 and figures were created using GraphPad Prism®, version 4.03. The Kolmogorov–Smirnov test and inspection of the data were undertaken to assess normality of all continuous data. All data are presented as mean ± standard error of the mean (SEM). Between-group comparisons of categorical data for ≥3 groups were compared using a chi-squared test. Continuous data were compared using ordinary ANOVA with Tukey's post-test for parametric data and with Kruskal–Wallis and Dunn's post-test for nonparametric data. Paired assessment of continuous data (e.g., postexercise and rest) was performed using a paired t-test and the Wilcoxon matched pairs test for parametric and nonparametric data, respectively. Correlation (r; 95% confidence interval [CI]) was assessed using the Pearson correlation for normally distributed data and the Spearman Rank correlation for nonparametric data with 95% CI. Binary logistic regression was undertaken to assess the independent predictors of both AMS and severe AMS separately along with inclusion of age, sex, and altitudes and exercise in the model. For the regression analysis, as AMS scores vary with the altitude, we ensured that the AMS scores were linked to the relevant altitude, exercise status (i.e., morning rest or postexercise), SpO2, and individual plasma marker values. Collinearity diagnostics were run to ensure that collinearity did not occur.
A p-value <0.05 was considered statistically significant for all comparisons.
Sample size and power calculation
Hartman et al. (2000) noted a significant increase in IL-6 from 0.5 ± 0.2 to 2.0 ± 0.8 pg/mL (p = 0.02) in a cohort of 10 subjects at 3647 m. Based on this and published data on healthy controls, we predicted that a sample size of 20 subjects would have ≥80% power to detect a difference between mean IL-6 levels of 1.29 pg/mL at a significance level (alpha) of 0.05 (two tailed). Recently, Iglesias et al. (2015) noted a 54% increase in resting (typically ≤0.65 pg/mL) ET-1 (Δ0.2 pg/mL and standard deviation of 0.2 pg/mL) and 75% increase in IL-6 among 10 subjects exposed to hypobaric hypoxia to 4000 m. A sample size of 20 in each group would have ≥80% power to detect a difference in means of 0.13 pg/mL at a significance level (alpha) of 0.05 (two tailed). Circulating IL-17a levels have never been assessed at HA, but based on plasma levels in healthy controls of 0.2–0.6 pg/mL with a standard deviation of <0.5 pg/ml, a similar sample would have ≥80% power to detect a significant change.
Results
All 48 subjects were investigated at 3833 and 4450 m and 47 of 48 subjects reached the highest study altitude. The SL and HA groups were well matched for age (35.0 ± 11.1 vs. 35.0 ± 9.0 years; p = 0.98), sex (males 65% vs. 70.8%; p = 0.71), height (172.2 ± 8.1 vs. 175.6 ± 9.5 cm; p = 0.14), weight (77.1 ± 15.2 vs. 77.8 ± 14.0 kg; p = 0.87), current smoking status (1/20 vs. 3/48; p = 0.52), and basic fitness levels based on a standardized 1.5 mile SL timed run test (10.2 vs. 9.9 ± 1.2; p = 0.42). The prevalence of AMS was 27.1% at 3833 m, 8.7% at 4450 m, and 37.8% at 5129 m. HA was associated with a significant fall in resting and postexercise SpO2 and an increase in heart rate compared with SL rest (Table 1).
Data shown are for 20 subjects at SL and 48 at HA; p-value refers to results of overall Kruskal–Wallis/one-way ANOVA with relevant post-test HA compared with baseline rest; (a) 3833 m postexercise; (b) 3833 m at rest; (c) 4450 m postexercise, (d) 4450 m at rest; (e) 5129 m postexercise, and (f) 5129 m at rest.
Paired test of rest versus postexercise at similar altitude.
HA, high altitude; SL, sea level; SpO2, oxygen saturation.
The effects of HA and exercise on inflammatory and endothelial markers
ET-1, IL-6, and IL-17a levels were all significantly higher at HA (n = 48) than at SL rest (n = 20) (Table 1). Analysis of only the 20 subjects who were studied at both SL and at HA revealed that ET-1 (6.1 ± 2.4 vs. 4.3 ± 1.9 pg/mL; p < 0.001), IL-6 (3.4 ± 2.9 vs. 2.4 ± 2.3 pg/mL; p = 0.006), and IL-17a (1.2 ± 1.9 vs. 0.5 ± 0.4; p < 0.001) were all significantly higher at HA than at SL (rest and postexercise data combined). At SL (n = 20), exercise led to a significant paired increase (vs. rest) in ET-1 and IL-6 levels, but not IL-17a (Figs. 1–3). For the same 20 subjects, there was a mean pairwise increase in resting ET-1 levels at HA of +80.9%, +51.4%, and +76.8% at 3833, 4450, and 5129 m, respectively. The equivalent data for IL-6 were +380.5%, +173.8%, and +172.7% and for IL-17a were +122.4%, +158.2%, and +128.4%.
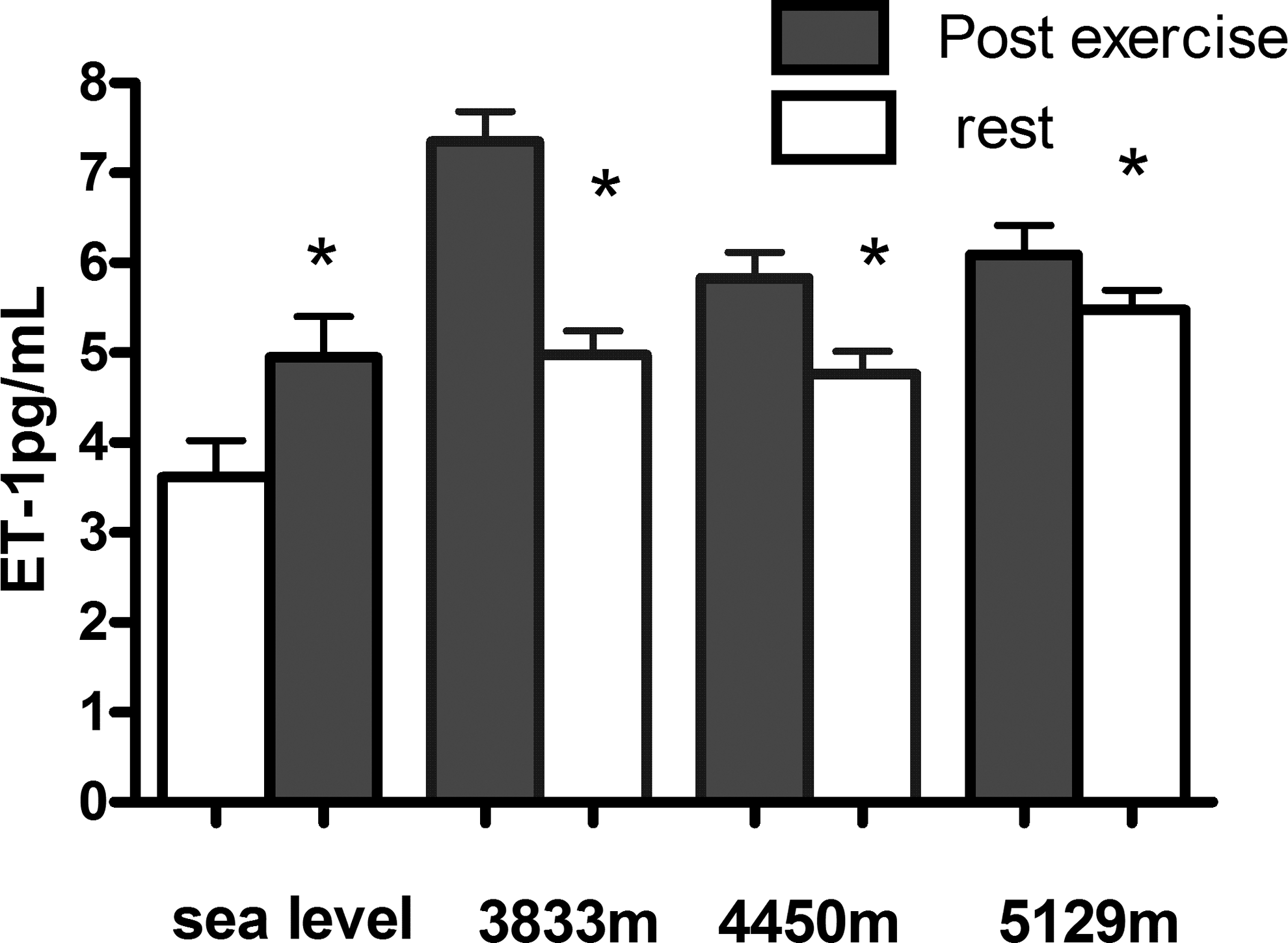
Effects of exercise on ET-1 levels (mean ± SEM) with increasing altitude. *Significant paired changes on rest versus exercise. Data shown are for 20 subjects at sea level (SL) and 48 at high altitude (HA).
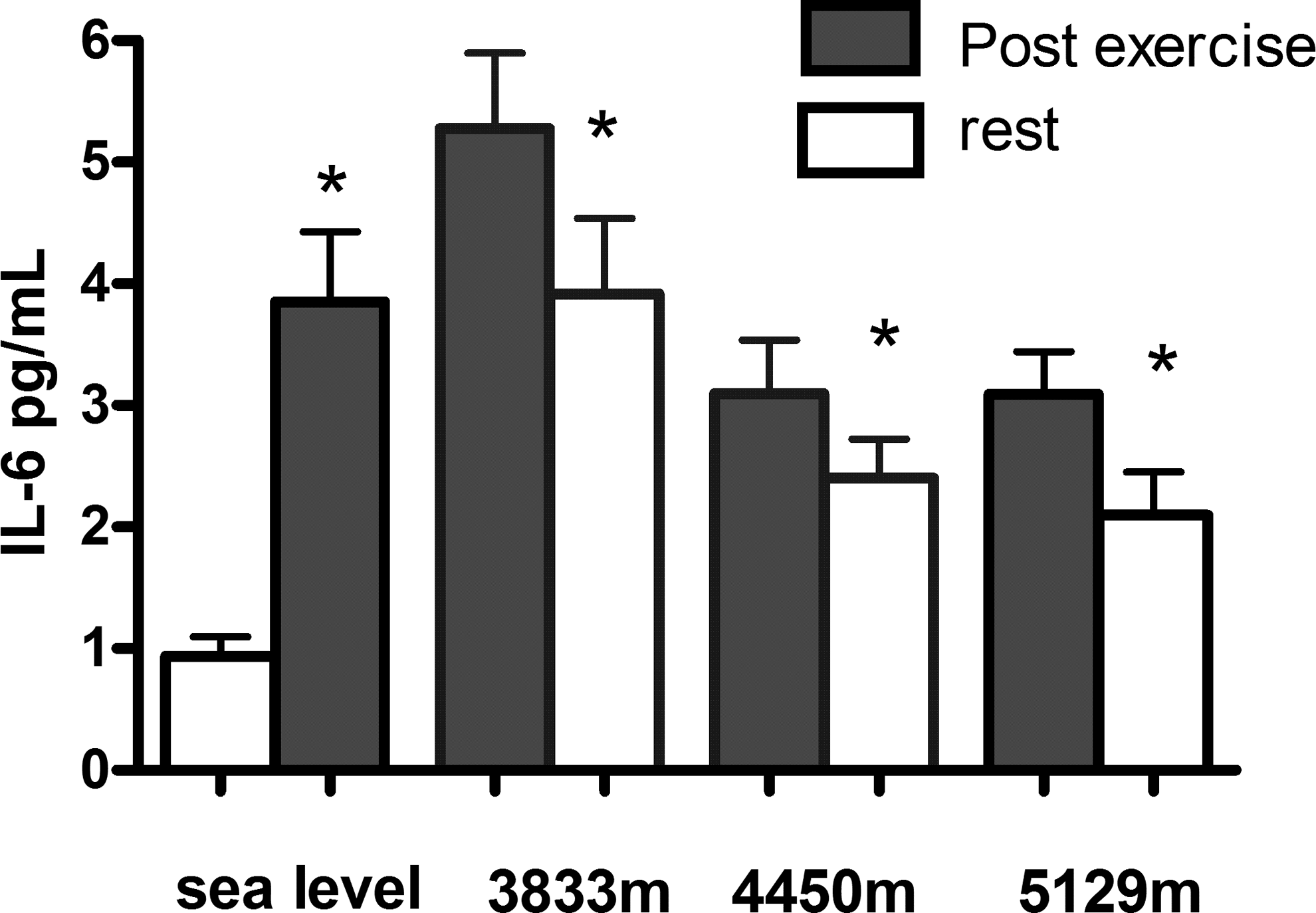
Effects of exercise on IL-6 levels (mean ± SEM) with increasing altitude. *Significant paired changes on rest versus exercise. Data shown are for 20 subjects at SL and 48 at HA.
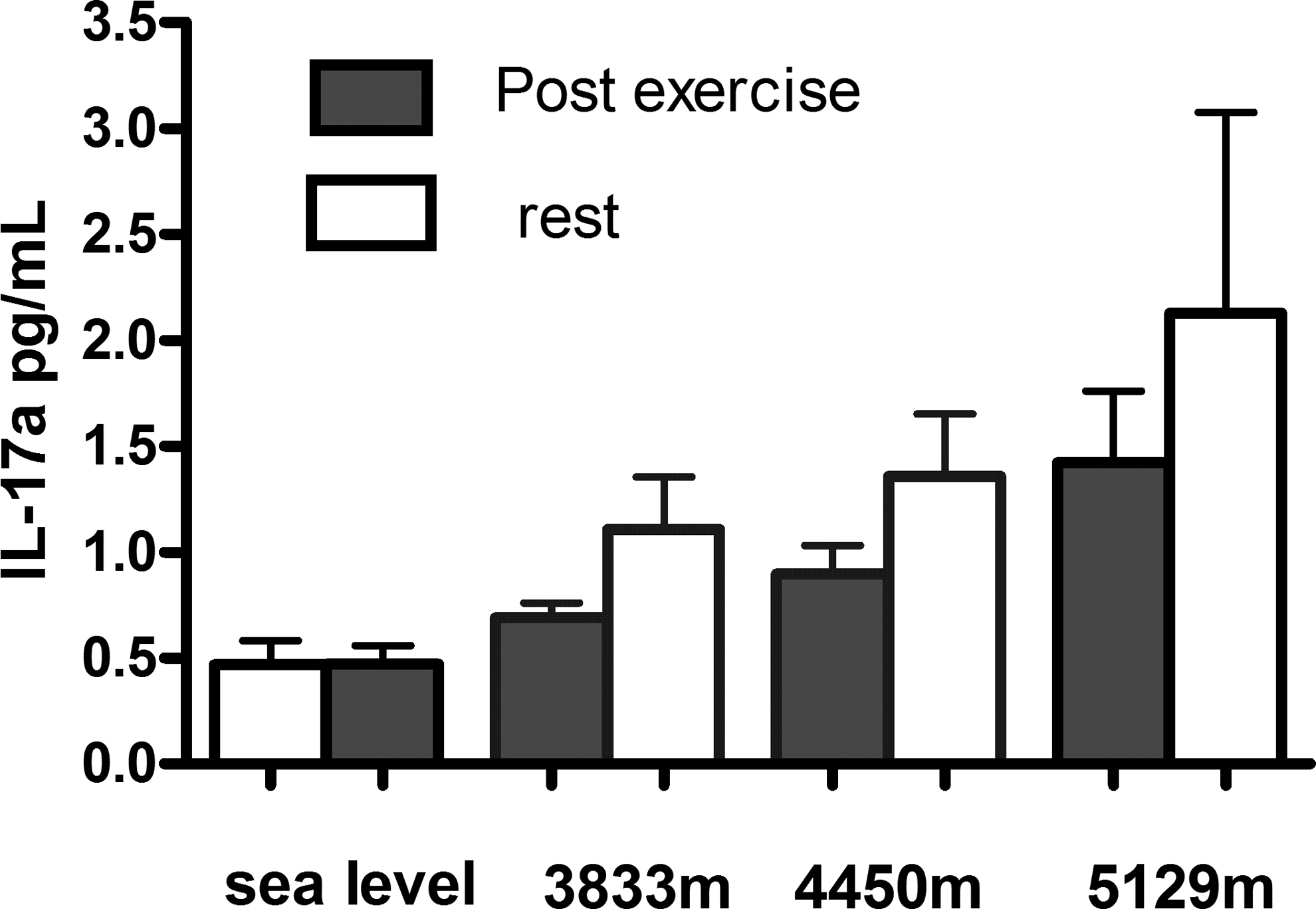
Effects of exercise on IL-17a (mean ± SEM) levels with increasing altitude. Data shown are for 20 subjects at SL and 48 at HA.
For the 48 subjects studied at HA, ET-1 and IL-6 levels were significantly higher postexercise compared with at rest at all altitudes (3833, 4450, and 5129 m) (Figs. 1 and 2). There was no significant change in postexercise versus resting IL-17a levels at HA (Fig. 3). ET-1 and IL-6 levels were higher at all time points at HA versus SL rest (Figs. 1 and 2). Compared with SL rest (0.46 ± 0.4 pg/mL), IL-17a levels were significantly higher at rest at 4450 m (1.4 ± 2.0 pg/mL; p < 0.001) and 5129 m (2.2 ± 6.4 pg/mL; p < 0.001) and postexercise at 5129 m (1.4 ± 2.3 pg/mL; p < 0.001) (Fig. 3).
Correlation
There was an overall inverse correlation between LLS and SpO2 (r = −0.32; −0.21 to −0.42: p < 0.001) and a positive correlation between LLS and IL-6 (r = 0.16; 0.05–0.27: p = 0.007) and ET-1 levels (r = 0.29; 0.18–0.39: p < 0.001). ET-1 inversely correlated with SpO2 (r = −0.36; −0.25 to −0.47: p < 0.001) as did IL-6 (r = −0.15; −0.04 to −0.28: p = 0.009) and IL-17a (r = −0.27; −0.16 to −0.38: p < 0.001). At HA, IL-6 levels were higher in those with AMS compared with those without AMS (3.9 ± 3.8 vs. 3.0 ± 3.0 pg/mL: p = 0.02) and again higher in those with severe AMS (5.1 ± 5.6 vs. 3.1 ± 3.0 pg/mL: p = 0.03). ET-1 levels were greater in those with AMS versus without (6.5 ± 2.3 vs. 5.2 ± 2.0 pg/mL: p < 0.001) and were even higher in severe AMS (6.7 ± 2.1 vs. 5.5 ± 2.2 pg/mL: p = 0.01) with a stepwise increase in ET-1 with increasing AMS severity (Fig. 4). IL-17a levels were not significantly different among those with AMS or severe AMS compared with those without. SpO2 levels were lower in those with both overall AMS (82.0% ± 6.5% vs. 86.1% ± 7.5%; p < 0.001) and severe AMS (79.6% ± 10.2% vs. 85.4% ± 6.8%; p = 0.001).
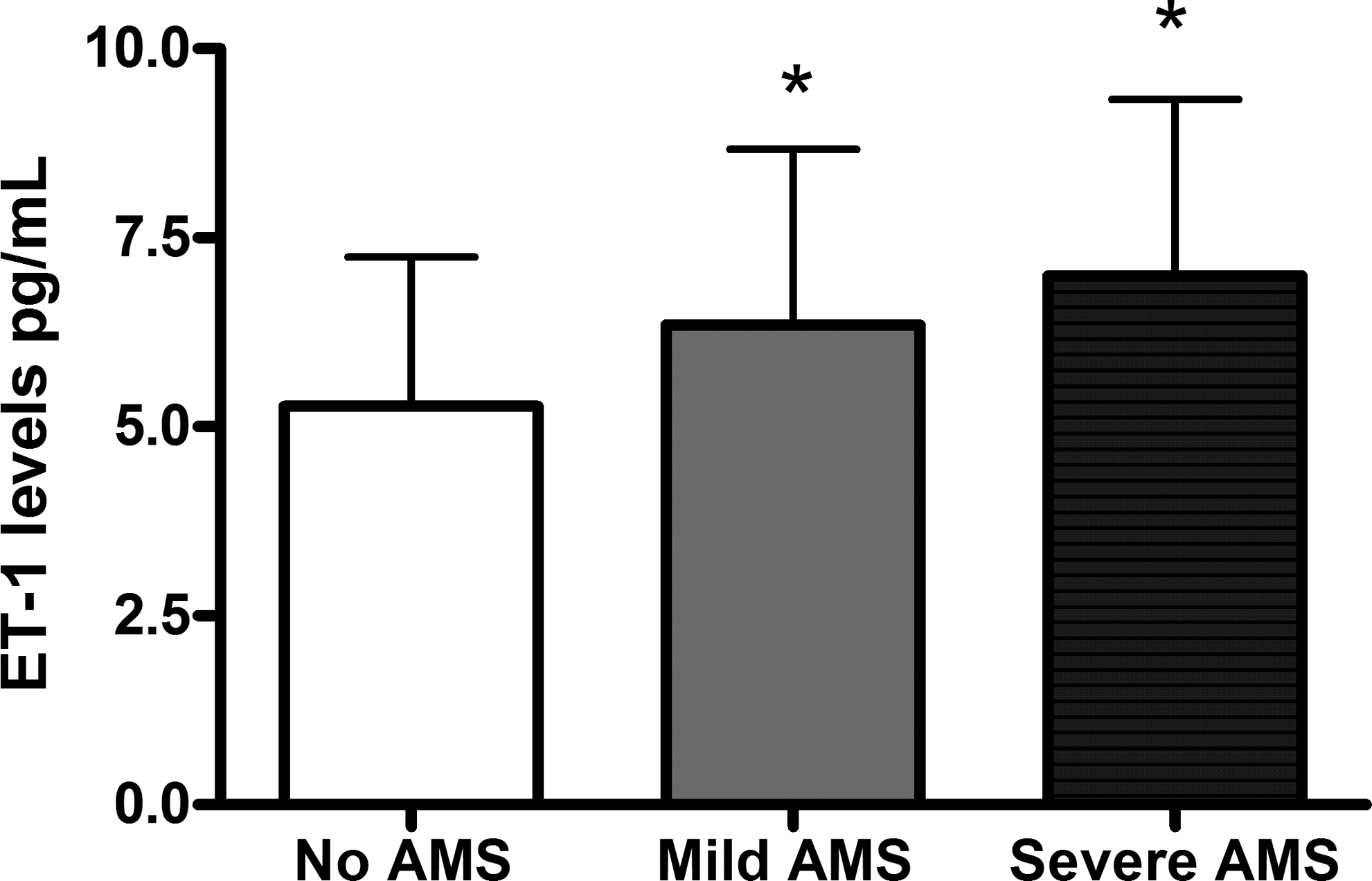
ET-1 levels with increasing severity of acute mountain sickness (AMS). *Significant compared with baseline on Kruskal–Wallis with post-test.
Multivariate analysis
The univariate predictors of AMS were altitude, exercise, SpO2, IL-6, and ET-1. A binary multivariate logistic regression analysis was performed to assess the independent predictors of AMS using these four univariate predictors as well as adjusting for the effects of exercise. ET-1 (p = 0.002) and reducing SpO2 (p = 0.02) were the only independent predictors (overall r2 = 0.16; p < 0.001) of AMS. ET-1 (p = 03) and SpO2 (p = 0.01) also remained as independent predictors of severe AMS (overall r2 = 0.19).
Discussion
This is the first study to assess the relationship between plasma markers of inflammation and endothelial activation/injury and the symptoms and severity of AMS. In this study, we found that HA is associated with a systemic inflammatory response and endothelial activation/injury as shown by a rise in the IL-6/IL-17a and ET-1, respectively, compared with SL. The increase in IL-6, IL17a, and ET-1 levels was related to the degree of hypoxia. ET-1 and SpO2 were independent predictors of both AMS and its severity on multivariate analysis.
Exercise is generally an integral part of HA exposure. Previous research has shown that hypoxia leads to increase in a number of systemic inflammatory cytokines and markers of endothelial activation/dysfunction (Hartmann et al., 2000; Mellor et al., 2014). However, it is well known that exercise, in the absence of hypoxia, can cause a rise in many of these plasma markers. This can lead to difficulties in the differentiation of the effects of HA from that of exercise. In the absence of hypoxia, in healthy adults, IL-6 levels have been shown to significantly rise (≥50%) immediately postexercise before rapidly falling toward pre-exercise levels over 3–6 hours, depending on the exercise stimulus (Sugama et al., 2012; Landers-Ramos et al., 2014). Similarly ET-1 levels also significantly increase postexercise (+0.1–0.2 pg/mL; ≥30%) typically peaking within one hour (Maeda et al., 1997; Kim et al., 2013). The effects of IL-17a and exercise have been barely studied with limited data showing either an immediate fall or no increase, followed by a return to healthy resting pre-exercise levels (≤0.6 pg/mL) over 1.5–3 hours (Sugama et al., 2012; Kanda et al., 2014).
Our data are consistent with the literature. We found that resting ET-1 and IL-6 levels were not only greater at every altitude study compared with SL rest but also the increase was even greater postexercise. This would suggest that not only was HA associated with an increase in markers of systemic inflammation (IL-6 and IL-17a) and endothelial activation (ET-1) but exercise also compounded this response. Resting systemic IL-17a levels were also higher at HA (significant at 4450 and 5129 m) versus SL, which is a novel finding. However, unlike ET-1 and IL-6, IL-17a levels were consistently (but nonsignificantly) lower postexercise at each altitude before the levels rose again on the resting samples taken >12 hours later the following day. The links between HA and the increase in IL-6, IL-17a, and ET-1 in our study are strengthened by the observed inverse relationship between IL-6, IL-17a, and ET-1 with SpO2, suggesting that HA-related hypoxia may be an important trigger for IL-6, IL-17a, and ET-1 release.
The pathogenesis of AMS is highly complex and is still poorly understood. Recognized mechanisms include altered vascular permeability, oxidative stress and abnormal renal responses, and water clearance to hypobaric hypoxia (Bärtsch and Swenson, 2013; Wojtal et al., 2014). While HA appears to be proinflammatory, the role of inflammation and endothelial dysfunction in the pathophysiology of AMS remains unproven and subject to debate (Kleger et al., 1996; Bärtsch and Swenson, 2013). Our data would partly support this as, while HA led to an increase in IL-6 and IL-17a, these markers were not independent predictors of AMS or its severity.
Conversely, ET-1 was an independent predictor of both overall AMS and severe AMS in our study; however, the overall risk prediction was relatively weak. This is a novel finding with a number of compelling factors to support this link. ET-1 is a well-established, although indirect, marker of both endothelial function and activation/damage. Increasing plasma ET-1 levels have been shown to strongly correlate with reducing brachial artery flow-mediated vasodilation (hence worsening endothelial function) and with levels of circulating endothelial microparticles (marker of endothelial injury), nitric oxide (NO) and NO synthase (eNOS) in adults with and without cardiovascular disease, and at levels not dissimilar to that observed in our current study (Cellini et al., 2012; Yang et al., 2013; Fan et al., 2014).
Diuresis is a key factor in the normal acclimatization to HA, serving to increase the hematocrit and oxygen carriage per unit of blood and counteracting the respiratory alkalosis of hypoxia-mediated hyperventilation (Bärtsch and Swenson, 2013; Mellor et al., 2015, 2014). It has been shown that in AMS this diuresis is reduced, leading to a net positive fluid balance, which may be triggered by an upregulation in arginine vasopressin (AVP) and copeptin and/or changes in peripheral chemosensitivity (Swenson et al., 1995; Boone and Deen, 2008; Mellor et al., 2015). There are both in vitro and in vivo data to show that ET-1 plays a pivotal role in water homeostasis and antagonizes the water-retaining effects of AVP to facilitate diuresis (Kamphuis et al., 1994; Ge et al., 2005). AVP is also a recognized stimulant for ET-1 release (Yamamoto et al., 1992). In a very recent study involving live rats, acute hypobaric hypoxia (8 hours at equivalent to 7000 m altitude) led to marked cerebral edema (akin to HACE) and significantly increased ET-1 content in the cortex, suggesting a strong link between cerebral ET-1 activation and severe AMS (Chen et al., 2014).
Our observation that reducing SpO2 was an independent predictor of AMS is not new and has been previously demonstrated, but remains subject to debate with conflicting results reported in the literature (O'Connor et al., 2004; Karinen et al., 2010). The fact that this relationship was observed for both overall AMS and severe AMS on multivariate analysis strengthens this finding.
This study has a number of limitations that should be acknowledged. The incidence of AMS was relatively low and may relate to the ascent profile, which included arriving at 3600 m to La Paz. The exercise stimulus was different in terms of duration, intensity, and altitude gain for each of the study altitudes. This is an important potential confounding factor given the significant influence of exercise on the plasma markers measured. However, this study reflects the reality of trekking to HA in the real world. Finally, while we observed an association between increasing ET-1 levels and severity of AMS, this relationship was not strong and does not necessarily reflect causation.
Conclusions
In this study, we have shown that HA is associated with endothelial activation (increased ET-1) and a proinflammatory (increased IL-6 and IL-17a) response. The rise in ET-1 and IL-6 is heavily influenced by the degree of exercise and symptoms of AMS. ET-1 appears to be an independent predictor of both AMS and its severity. Further larger studies would be helpful to further explore this novel finding.
Footnotes
Acknowledgments
The results of the present study do not constitute an endorsement by ACSM. Research reported in this study was supported by the Surgeon General, UK, and Singulex®. The content is solely the responsibility of the authors and does not necessarily represent the official views of the UK Defence Medical Services.
Author Disclosure Statement
This study utilizes a previously published cohort, but represents new and previously unpublished data. No competing financial interests exist.