
Abstract
Abstract
Willmann, Gabriel. Ultraviolet keratitis: From the pathophysiological basis to prevention and clinical management. High Alt Med Biol 16:277–282, 2015.—Ultraviolet keratitis is caused by the toxic effects of acute high-dose ultraviolet radiation (UVR) reflecting the sensitivity of the ocular surface to photochemical injury. The clinical syndrome presents with ocular pain, tearing, conjunctival chemosis, blepharospasm, and deterioration of vision typically several hours after exposure, lasting up to 3 days. Mountaineers, skiers, and beach recreationalists are particularly at risk to suffer from ultraviolet (UV) keratitis as the reflectivity of UVR in these environments is extremely high. The aim of this review is to raise awareness about the potential of UV damage on the eye with an emphasis on UV keratitis, to highlight the pathophysiological basis of corneal phototoxicity, and to provide practical guidance for the prevention and clinical management of UV keratitis commonly known as snow blindness.
Introduction
T
The energy of the radiation determines the degree of oxidative photodegradation on the ocular surface of the cornea. Usually severe ocular pain, tearing, conjunctival chemosis, blepharospasm, uncontrolled blinking of the eyelid, and deterioration of vision characterize the clinical syndrome with a delayed onset typically several hours after exposure (Cullen, 2002). While the course of the disease is often self-limiting and aiding treatment options are available, the only option to prevent corneal epithelial cells from degenerating from high-energy UVR is to minimize radiation exposure.
After an initial overview on UVR, the pathophysiological basis of phototoxicity, followed by measures of prevention and clinical management in respect to UV keratitis, will be discussed.
Pathophysiological Basis of UV Keratitis
Ultraviolet radiation
UVR is invisible to human perception and presents the shortwave electromagnetic spectrum of 100–400 nm. In contrast, visible light ranges from about 400 to 700 nm and infrared light from 700 to 1200 nm (Bachem, 1956). UVR can further be divided into UV-A (320–400 nm), UV-B (280–320 nm), and UV-C (100–280 nm) (Bachem, 1956; Pitts and Tredici, 1971; Norren and Vos, 1974). The ozone layer, in addition to water vapor and oxygen/carbon dioxide, is able to absorb almost all of UV-C and >90% of UV-B radiation (Norval et al., 2007). However, with a diminishing ozone layer, the amount of UV-B radiation today reaching the ocular surface has an increased potential for biological damage compared with decades ago (Behar-Cohen et al., 2014). Figure 1 provides an overview of the various effects of UVR on the eye.
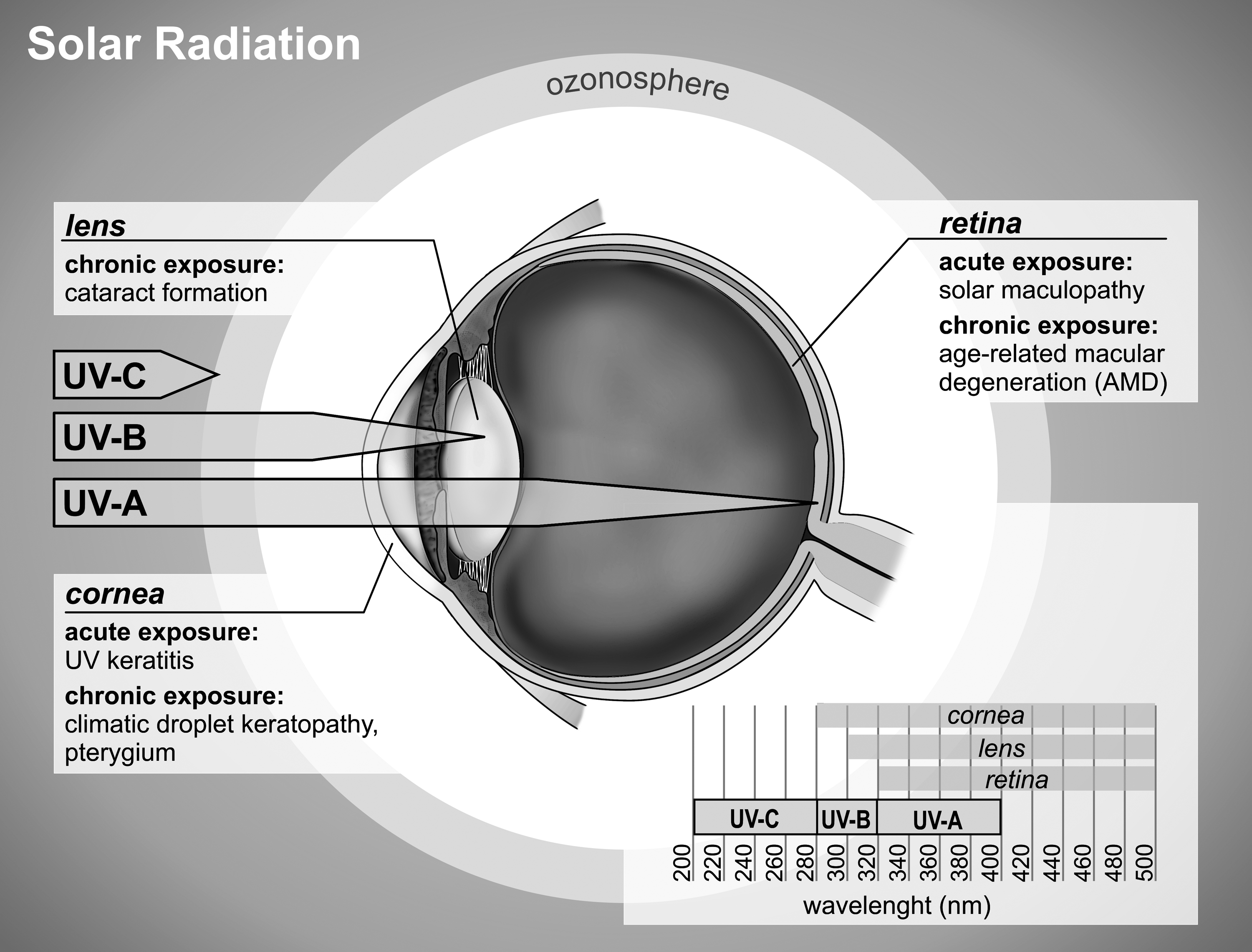
Ultraviolet radiation (UVR) can be divided into UV-A (320–400 nm), UV-B (280–320 nm), and UV-C (100–280 nm). Visible light ranges from about 400 to 700 nm and infrared light from 700 to 1200 nm. Extremely short and high-energy UV-C rays are almost completely absorbed by the ozone layer. The cornea absorbs a high fraction of all UV-B rays reaching the ocular surface, making it vulnerable to develop UV keratitis upon acute exposure. Cataract formation of the lens is mainly attributed to chronic UV-A radiation. Chronic UVR may also be responsible for other ocular surface diseases, while age-related macular degeneration is thought to be associated with the blue light fraction of the visible light.
Cogan and Kinsey (1946) have first reported the action spectrum of UVR for UV keratitis. At a wavelength of about 270 nm, only relatively little energy (0.005 J/cm2) is required to produce UV keratitis (Kolozsvari et al., 2002). Hence, a short wavelength of around 280 nm surmounts the damage potential of longer wavelengths of about 300–320 nm by a factor 600×, indicating that spectral energy increases as wavelength decreases (Reme et al., 1996; van Norren and Gorgels, 2011). For this reason, the International Organization for Standardization (ISO) 8990/3 norm defines a cutoff for potential ocular damage of 380 nm, which has been adopted by the World Health Organization (WHO).
As direct sunlight only contributes about 50% to the ambient UVR, scatter and reflection play a key role in overall ambient UVR (Sliney, 1997; Sydenham et al., 1997). According to Rayleigh's law, the shorter the wavelength, the greater the amount of scattered UVR, indicating that on a bright sunny day, the main proportion of UV-B incident to the eye and especially the cornea is largely contributed by diffuse scatter. Cloud cover or haze may further increase the amount of scatter. Another key component of the total ambient UVR is ground reflection, which greatly varies depending on the surface. While grass and rocks reflect at low rates (2%–5%), water reflects at higher (10%–25%), and snow cover at much higher rates (>90%) (Atkinson, 1921). High altitude and low latitude further increase the ambient UVR burden, putting high altitude mountaineers at great risk for the development of acute phototoxic diseases such as UV keratitis. UVR increases with altitude at a rate of ∼4% per 1000 feet as a result of decreased atmospheric absorption (Ellerton et al., 2009). Other environmental factors such as season of the year have been shown to influence the peak ocular exposure time as the total amount of UVR reaching the eye largely depends on the actual solar angle (Sasaki et al., 2011; Chao et al., 2013). Compared with summer, it shifts to actual solar noon in winter because the maximum daily solar altitude drops below the occlusion angle (Sliney, 1999; Sasaki et al., 2011). For the very same reason, the UVR burden to the eye may be as much as twice as high in the morning compared with noon (Chao et al., 2013). Finally, anatomical features as the upper orbital rim composition, the brow, and the nose also influence the amount of direct and reflected radiation entering the eye (Merriam, 1996).
Pathophysiological basis of phototoxicity to the cornea
Oxidative photodegradation is largely dependent on three factors: radiation exposure at a specific wavelength, tissue type containing a specific chromophore for that wavelength, and oxygen. The degree of damage depends on time of exposure and energy of radiation. Due to its high content in protein and nucleic acid, the cornea, particularly the corneal epithelium, absorbs predominantly UV-B in the range of 280–300 nm, acting as a major protection shield against UVR for the eye. However, when the threshold radiation dose for biological damage is reached, absorption of UVR leads to the generation of reactive oxygen species (ROS) as a result of an imbalance between ROS generation and antioxidant defense (Cullen, 2002; Chao et al., 2013).
The production of ROS leads to the disruption of important cellular components such as cellular membranes, DNA, and proteins with the consequence of biological dysfunction and damage (Bergendi et al., 1999). Mainly hydroxyl radicals induce the oxidative degradation of cellular membranes in the form of lipid peroxidation (Esterbauer et al., 1991). In addition, upon UVR, the hydroxyl radical can react with a number of DNA components targeting purine and pyrimidine bases and the deoxyribose backbone to alter DNA structure (Liu et al., 1996; Cai et al., 1998; Halliwell, 1998). Finally, proteins are targeted by ROS. Specifically, amino acids, cysteine, and methionine are affected by oxidative stress, resulting in structural and functional inactivation (Dean et al., 1997). Furthermore, high-dose UVR causes upregulation of proinflammatory cytokines by activation of nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) and leads to apoptosis in corneal cells by direct cell membrane damage through necrotic receptor activation (Black et al., 2011). Figure 2 presents an overview of the pathophysiological mechanism of UV keratitis.
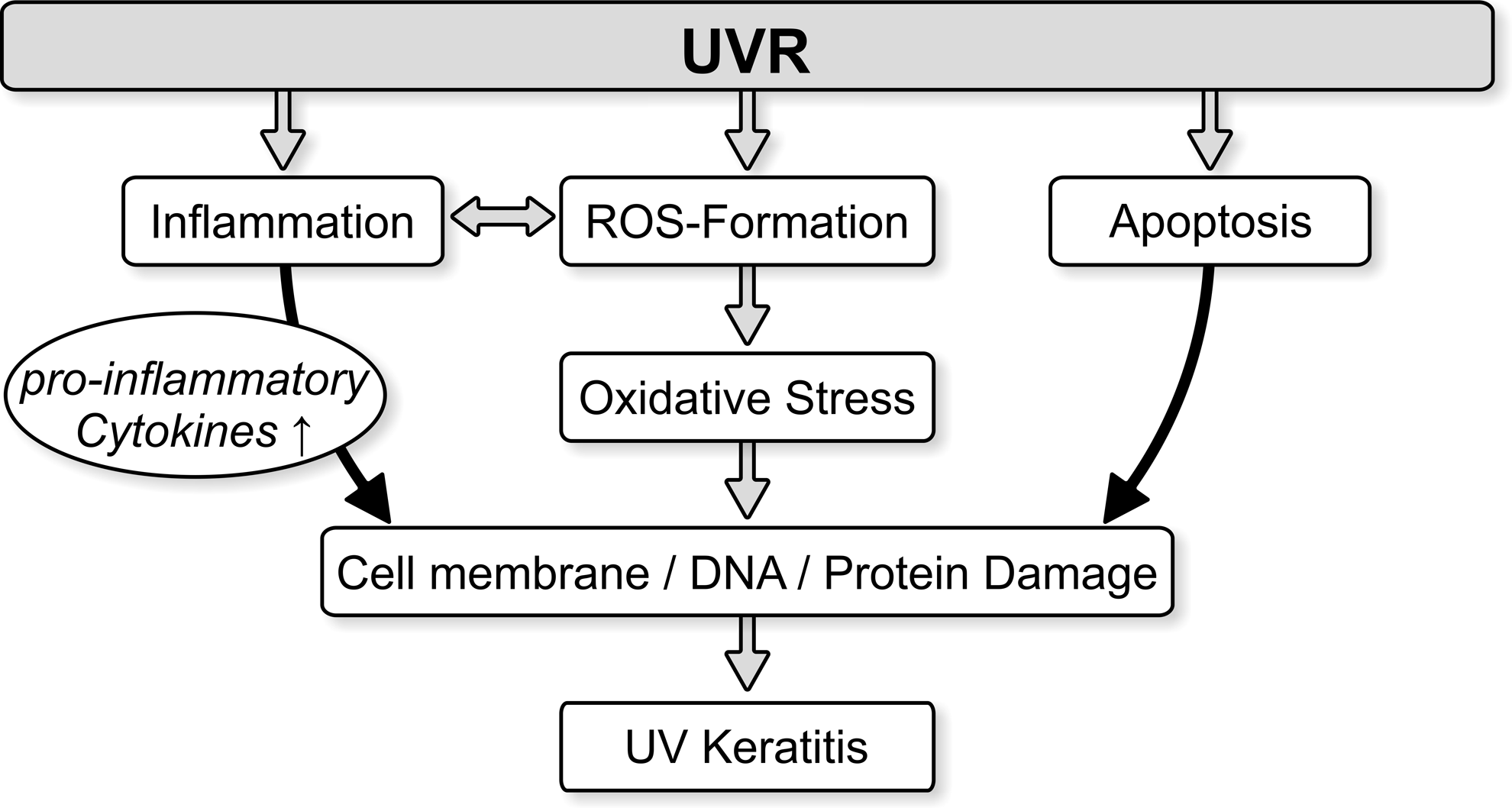
The mechanisms involved in phototoxicity to the cornea include oxidative stress by reactive oxygen species (ROS) formation, induction of inflammation with the production of proinflammatory cytokines, and apoptotic cell death through necrotic receptor activation. Evidence suggests that multiple enzymatic and nonenzymatic antioxidants of the cornea and tear film play a crucial role in protecting the ocular surface from the damaging oxidative effects of UVR.
The antioxidant defense system
The cornea together with the tear film and aqueous humor present the first barrier against UVR. Thus, the ocular surface has developed a cellular defense system to protect the eye. Various enzymatic and nonenzymatic antioxidants play a key role in protecting ocular tissues against oxidative damage by scavenging and neutralizing ROS. An antioxidant is a molecule that inhibits the oxidation of other molecules. To terminate the process of oxidative photodegradation, antioxidants remove free radical intermediates by being oxidized themselves. Therefore, antioxidants are often reducing agents.
An important factor in protecting the cornea from UVR insult is the corneal crystalline aldehyde dehydrogenase, ALDH3A1 (Chen et al., 2013). It comprises a large portion of soluble proteins of the cornea and acts through metabolism of toxic aldehydes, generation of reduced nicotinamide adenine dinucleotide phosphate (NADPH), scavenging of ROS, and chaperone-like activity (Estey et al., 2007). It may even absorb UV light directly. Another important small-molecule antioxidant is glutathione, which is differentially distributed within the cornea with highest levels reaching in the epithelium (Dalton et al., 2004). In conditions of oxidative stress, it can counteract against free radicals as well as regenerate other antioxidants, such as vitamin C and E, and protect the integrity of cellular membranes (Watson et al., 2003). Ascorbic acid itself (vitamin C) is known to promote healing of damaged corneal tissue by serving as a cofactor for collagen synthesis (Piatigorsky, 2001; Pappa et al., 2003). Other important antioxidants of the cornea include L cysteine, L-tyrosine, α-tocopherol, retinol, albumin, ferritin, superoxide dismutase, and catalase (Marchitti et al., 2011).
Prevention and Clinical Management
Prevention
UVR generally poses a risk for the eye throughout life. However, when acute high ocular UV exposure is encountered during high altitude mountaineering or skiing, one is at great risk of developing UV keratitis unless preventative measures are in place. Less than two hours of UV radiation reflected from snow has been reported to be enough to cause UV keratitis (Dolin and Johnson, 1994).
Individual predisposition factors such as orbital anatomy, corneal thickness, or pupil size also determine the overall UV burden to the eye. Photosensitizing drugs such as tetracyclines or chloroquine may also increase the susceptibility to UVR damage and should be avoided. General prevention strategies to avoid the risk of UV keratitis include wearing a hat to block exposure from above and more importantly the use of sunglasses or contact lenses, also to block low-angle and reflected UV radiation (Sasaki et al., 2011).
While all sunglasses have at least some UV-blocking characteristics, the amount of UV absorption varies widely (Borgwardt et al., 1981). In one study, 75% of all lenses tested failed to provide the 95% UV-A protection recommended by the US Food and Drug Administration (Velpandian et al., 2005). In addition, neither brand nor price seems to predict the quality of UV protection available in sunglasses (Bazzazi et al., 2015). The type of sunglass should be chosen according to the environmental terrain and planned activity (Butler, 1999). Respective dark lens sunglasses, which transmit much less visible light in combination with side shields, should be used in snowy conditions or at high altitude. However, dark lens sunglasses may also cause pupil dilation and have been shown to actually increase UV transmission into the eye (Pitts and Tredici, 1971; Sliney, 2011). Nevertheless, sunglasses without side shields significantly increase UV exposure as UVR coming in from the sides is not blocked and therefore back reflection from the antireflective coatings of the sunglasses is increased (Rosenthal et al., 1988; Sliney, 2001). This increase in back reflection adds to the overall UVR burden. Finally, under extreme environmental conditions (wind, cold), snow goggles with respective UV filters may also be useful and can be recommended.
UV-blocking soft contact lenses that completely cover the pupil and limbus seem to be a particularly good option to prevent UV rays from damaging the cornea and reaching internal structures of the eye (Walsh and Bergmanson, 2011). UVR coming in from the sides is totally blocked and back reflection is not an issue (Kwok et al., 2003). The initial development of contact lenses years ago showed variable UV absorption in respect to UV-A (Anstey et al., 1999). However, the characteristics of newer soft contact lenses available today are much improved and some even exhibit enhanced UV-filtering capabilities up to a wavelength of about 390 nm. One example of a soft contact lens capable of filtering all of UV-B and a major portion of UV-A is the Acuvue® Advanve® (Lira et al., 2009). Nevertheless, the use of contact lenses has to be carefully assessed in remote wilderness areas or at high altitude as these conditions provide a challenge for appropriate contact lens wear and care with a potential risk of infections (Bauer, 2015).
Clinical manifestation and management
In the event of UV keratitis, the primary strategy is to avoid further exposure to UVR. One should reassess if all measures of appropriate prevention have been applied and avoid any further exposure to damaging UVR. It is important to note that all symptoms usually resolve within 24–72 hours depending on the degree of UV damage (Dolin and Johnson, 1994; McIntosh et al., 2011).
The clinical manifestation of the typically bilateral occurring UV keratitis ranges from a mild superficial punctate keratitis to severe cases with total epithelial desquamation. Severity may also vary between individuals as light- versus dark-skinned humans or individuals with pre-existing ocular conditions, such as dry eye syndrome, keratokonus, or postoperative refractive surgery (e.g., LASIK), may even be more likely to develop severe forms of UV keratitis. While mild forms may only present with a red eye and increased foreign body sensation, severe cases usually have significant ocular pain, lacrimation, chemosis, blepharospasm, and decreased visual acuity. Interestingly, the clinical syndrome is characterized by a lag time between exposure and beginning of clinical symptoms. While increased redness of the conjunctiva, chemosis, foreign body sensation, and lacrimation may occur quite rapidly after exposure, the absence of ocular pain for about 6–12 hours is characteristic for UV keratitis. This phenomenon has been attributed to the loss and return of corneal sensitivity in an experimental study (Millodot and Earlam, 1984). Due to the fast reepithelialization of the cornea, the resolution of clinical symptoms is often rapid and permanent damage is extremely rare.
Apart from the primary strategy of avoiding further UV exposure, there are several therapeutic approaches to aid clinical symptoms and gain faster recovery. Vision is usually blurred due to epithelial trauma, resulting in constant tearing. Moreover, uncontrollable blinking over the exposed corneal surface causes pain and blepharospasm. The frequent use of topical lubrication, ideally with preservative artificial tears containing antioxidative properties such as Artelac EDO® (Bausch+Lomb, Bridgewater, NJ), is recommended (Rieger, 2001). Indeed, artificial tears should also be used as a measure of prevention, especially when at high attitude, as tear film stability due to increased evaporation is significantly reduced (Willmann et al., 2014). Topical anesthetics should not be used as they delay and prevent corneal reepithelialization (Burstein, 1980; Patel and Fraunfelder, 2013). However, in emergency situations, for example, when a stricken climber at high altitude needs to descend to safety, short-term application of topical anesthetics may be considered to stop the crucial pain and constant blinking (Sliney, 2001). Otherwise, for comfort and relief of pain, a bandage contact lens in addition to lubrication is usually sufficient. In addition, topical antibiotic ointment (e.g., erythromycin drops) should be used in moderate and severe cases to prevent infection. In severe cases, additional nonsteroidal anti-inflammatory eye drops and oral acetaminophen or other narcotic analgesics can be used to alleviate symptoms of discomfort and redness of conjunctival tissue. Cycloplegic eye drops (cyclopentolate 1%) may also be considered for pain relief, but result in a wide pupil, altering visual acuity and increasing glare. Although very efficient for pain relief, they may not be appropriate for use in a wilderness setting.
People at risk, particularly mountaineers travelling to remote snow-covered areas or to high altitude, should be familiar with the prevention and clinical management of UV keratitis as this usually benign condition may result in incapacitation, requiring assistance in severe cases. Therefore, a first aid kit should always contain at least spare sunglasses and/or contact lenses, artificial tears for lubrication, and a topical antibiotic ointment. In Addition, a topical anesthetic for emergency use only may be considered.
Conclusion
Acute suprathreshold UVR ultimately leads to UV keratitis unless appropriate protective measures are applied. With a diminishing ozone layer, preventing the eye from UVR becomes even more important. When wearing sunglasses, side shields should be used to avoid back reflection caused by antireflective coatings and dark versus light lenses should be chosen depending on environmental conditions. UV-filtering contact lenses might be a particularly good option as they automatically filter light from all angles. When being outdoors, it is important to keep in mind that the UV burden on the eye might peak at hours different to the skin due to the increase in direct and reflected sunlight to the eye at lower solar angles. Due to the antioxidant defense mechanism of the cornea and the ability for fast reepithelialization, clinical symptoms are often self-limiting within a few days. For effective relief of the clinical symptoms encountered, relatively easy-to-follow treatment regimes are available.
Footnotes
Author Disclosure Statement
No competing financial interests exist.