
Abstract
Abstract
Brustia, Raffaele, Giulia Enrione, Bruna Catuzzo, Luca Cavoretto, Massimo Pesenti Compagnoni, Enrico Visetti, Emmanuel Cauchy, Stefanie Ziegler, and Guido Giardini. Results of a prospective observational study on mountaineering emergencies in Western Alps: mind your head. High Alt Med Biol. 17:116–121, 2016.—
Methods:
From 1st January 2012 to 31st December 2013 all patients admitted to the Aosta Regional Hospital Emergency Room for any event occurred above 2500 m were screened: all those affected by High Altitude Illness, Acute Illness in High Altitude, Trauma, or Cold disease were prospectively included. Activity incidence rate is expressed as the occurrence of mountain-related events per 1000 hours of mountain activity. Event Incidence rate is expressed as the occurrence of new cases per 1000 hours of mountain activity.
Results:
Two hundred two patients were included during the study period. Trauma (65.1% vs. 24.6%, p < 0.001) and head commotive injury (48.1% vs. 15.1%, p < 0.001) were more frequent during winter compared to the summer season. High altitude illness (36.9% vs. 9.3%, p < 0.001) and cold pathologies (15.1% vs. 0.1%, p < 0.001) occurred more frequently in summer than in winter. Patients (51.4%) were immediately discharged from emergency room, 8.4% after a 24-hour observation period, and 30.6% required hospitalization. During summer, the event risk is 0.013 per person and 1000 hours of mountain activity, while in winter, event risk amounts to 0.005 per person and 1000 hours of mountain activity.
Comments:
High altitude medical events or trauma represent <1% of pathologies observed in the emergency room department of a mountain district in the western Alps. Head commotive injury is the most observed mountain-related event in high altitude, in winter and during ski practice. High altitude illness and cold injuries are observed more frequently in summer, during trekking or climbing activities.
Background
A
Among trekkers, the rate of acute mountain sickness (AMS) at moderate altitudes is 25% and increases up to 50% for high altitudes. Even if the incidence of high altitude cerebral edema (HACE) and high altitude pulmonary edema (HAPE) is much lower (0.1%–4.0%) (Basnyat and Murdoch, 2003), consequences can be dramatic, including death. Common activities as mountain hiking or skiing are associated to a 4/100,000 death rate annually (Burtscher et al., 2007) and to a 60% rate of severe head injury (Jacquot et al., 2011). Simple measures as adequate training, pharmacological interventions (Burtscher et al., 2007), or the use of a helmet (Sulheim et al., 2006) can result in strong risk reduction.
The only regional hospital of the VdA region offers primary and specialized care, and difficult access—due to geographical and meteorological conditions—is supplied by the Territorial Emergency Service, by ambulances or helicopters.
The aim of this prospective monocentric observational study is to obtain a precise picture of mountain-related medical and trauma major events, their seasonal and activity-related risk, and to provide a better mountaineer education, guide recommendations for safety devices, and prevention.
Methods
Study period, design, and patient population
From 1st January 2012 to 31st December 2013, three physicians (G.E., R.B., and L.C.) held a prospective (electronic/paper) screening among patients admitted to the Aosta Regional Hospital Emergency Room (ER), for any event that occurred above 2500 m. Depending on clinical conditions and diagnoses, patients were discharged, kept for 24 hours clinical observation, or hospitalized.
If the altitude criterion was fulfilled, patients were prospectively included in a database if the final discharge diagnosis was any of the following: high altitude illness, acute illness in high altitude, trauma (head trauma or polytrauma), or cold disease.
Altitude was defined as follows (Bartsch and Saltin, 2008):
• Moderate altitude (2000–3000 m) • High altitude (3000–5500 m) • Extreme altitude (>5500 m) • Altitude cutoff was set at 2500 m, because high altitude illness is much more likely to occur above this level (Basnyat and Murdoch, 2003).
Diagnosis: We decided to focus on
(1) High Altitude Illness: as AMS, HAPE, HACE. Diagnosis was clinical and based on Lake Louise Score (LLS) questionnaire (Roach et al., 1993; Basnyat and Murdoch, 2003; Sulheim et al., 2006; Bartsch and Saltin, 2008; Jacquot et al., 2011; Luks et al., 2014).
(2) Acute Illness occurred in High Altitude:
• Any neurological major acute event: stroke, transitory ischemic attack (TIA), severe headache, and epileptic seizure. • Any cardiologic major acute event: myocardial infarction (MI), arrhythmias, symptomatic hypertensive peak, and syncope. • Diagnosis was established either by an emergency physician or a specialist expert opinion (neurologist or cardiologist).
(3) Trauma: Head commotive injury, and patients involved in severe polytrauma. Minor trauma (e.g., single bone fractures, contusions) was not included. Multiple fractures were considered part of polytrauma and, therefore, included under this definition.
(4) Cold diseases: (hypothermia, avalanche victims, frostbite).
Fatalities: any fatality that occurred in the hospital or during rescue operations was included. Vice versa, patients declared dead on-site, since not admitted to the ER, were not included.
Data collection: Age, gender, activity during the disease onset, essential past medical history, onset symptoms, and final diagnosis were prospectively recorded.
Statistical and epidemiological analysis: (Knowles et al., 2006; Schöffl et al., 2011; Blake et al., 2014).
Activity: mountain activity during which the event occurred. We considered the most popular and common activities, as ski, trekking, alpine climbing, and professional working activity.
Event: total number of medical illness in altitude, high altitude illness, trauma, or cold disease reported.
Activity incidence rate is expressed as the occurrence of new mountain-related events per person and 1000 hours of a specific occupational activity.
Event incidence rate is expressed as the occurrence of new cases of events per person and 1000 hours of activity.
Exposure days spent in altitude, per person, are calculated
• in summer season as the number of nights spent (per person) in a mountain refuge at >2500 m
• in winter by the daily number of skiers accessing ski resorts at >2500 m.
Daily (exposure) hours: mean number of hours per person (person hours) in altitude, and are considered per day and activity. Depending on the activity, the daily (exposure) hours were calculated as follows:
• Alpine climbing was considered as an alpine expedition, taking at least 2 days or more and calculated on the number of nights spent per person in a mountain refuge at >2500 m. For each day, an estimate of 16 hours per person was considered, based on 12 hours of climbing time, 4 hours of camp activity, and 8 hours of sleep. (Schöffl et al., 2011). • Trekking, was considered as hiking without climbing for 8 hours a day per person. • Ski was considered during 6 hours per day per person. • Working was considered an occupation during 8 hours of exposure per day per person.
Exposure time to calculate the event risk was calculated according to the mean hours spent per activity and person, per number of days at high altitude (Knowles et al., 2006; Schöffl et al., 2011; Blake et al., 2014).
Pearson chi-squared test was used for nominal variables, and exact Fisher's test when necessary. A p-value <0.05 was considered as significant.
Results
Study population, demographics
From 1st January 2012 to 31st December 2013, 102,714 patients were admitted to the Aosta ER. Of these, 102,512 (99.8%) did not meet the inclusion criteria and were therefore excluded; the remaining 202 (0.1%) represent our study cohort. Disease distribution is detailed in Figure 1, with trauma as the leading diagnosis (50.4%). Monthly distribution follows summer and winter seasonal peaks (Fig. 2), with 73 (35.6%) and 129 (63.8%) patients, respectively. When focusing on activity, climbing was significantly more practised in summer (32 of 73, 43.8%) than in winter (3 of 129, 2.3%, p < 0.01%), while skiing more frequently during the winter season (123 of 129, 95.3%) than the summer (16 of 73, 21.9%, p < 0.01). No seasonal difference was found with working activity (3 of 73, 4.1% vs. 1 of 129, 0.1%, p = 0.09) (Table 1).
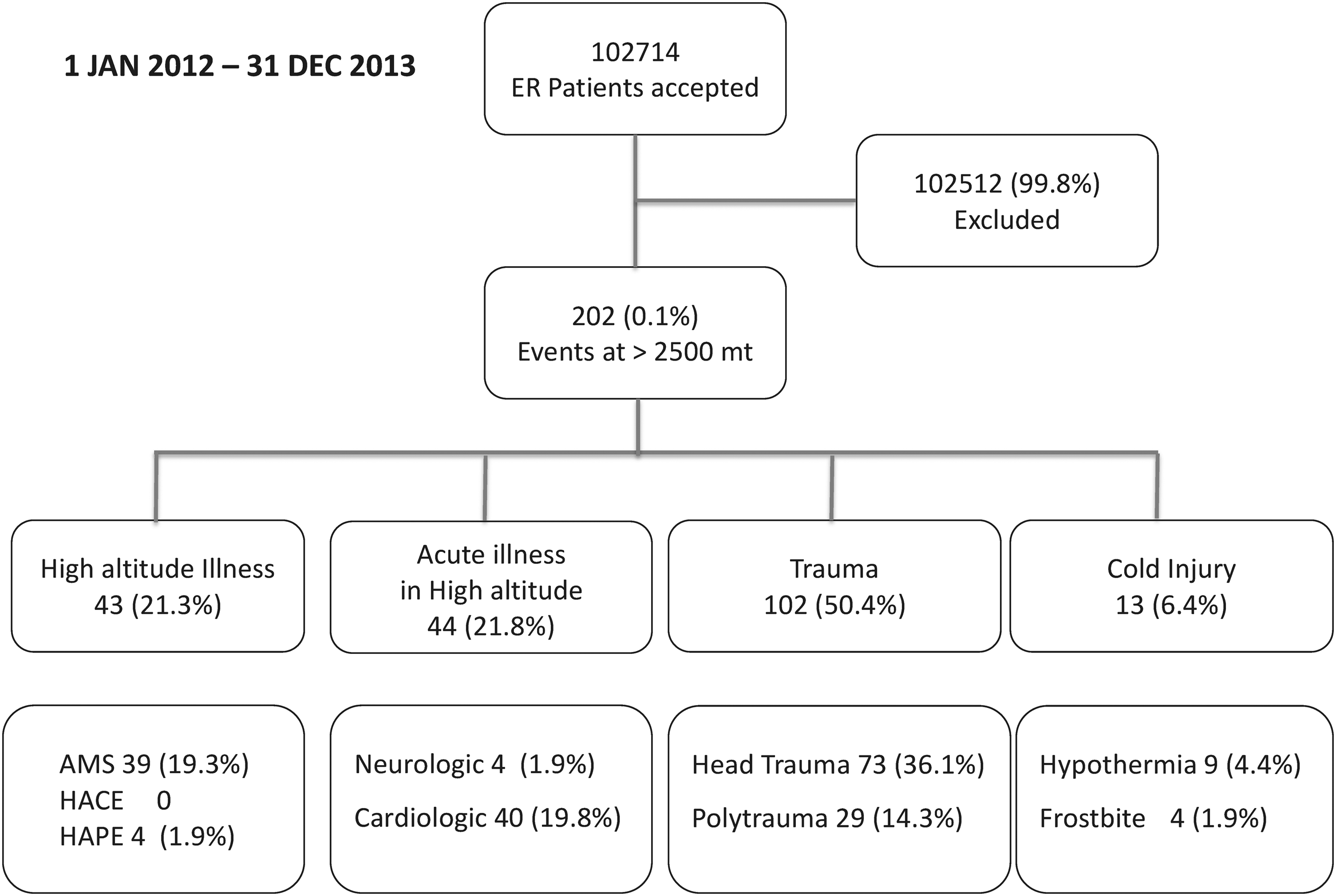
Patients flowchart, inclusion criteria.
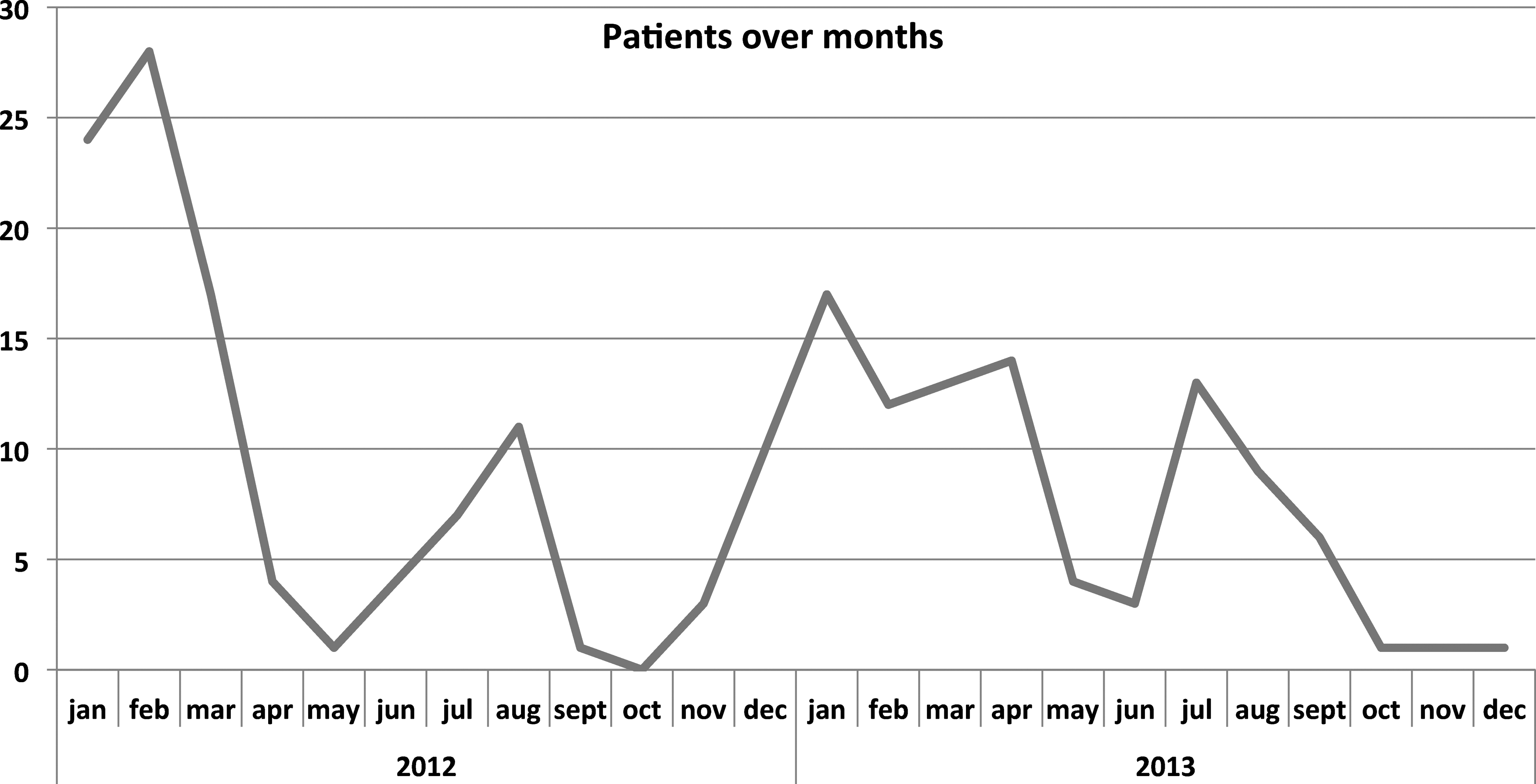
Patients distribution over months.
Activity represents the occupation in which patients were involved when the event in altitude appeared, and their relative seasonal distribution. One patient activity in summer is missing.
F, female; M, male.
Diagnosis
Trauma significantly accounts for the leading diagnosis during winter (84 of 129, 65.1%) compared to the summer season (18 of 73, 24.6%, p < 0.001). Subgroup analysis revealed head commotive injury to be more observed during winter (62 of 129, 48.1%) than in the summer season (11 of 73, 15.1%, p < 0.001), while no significant difference in seasonal distribution (7 of 73, 0.9% vs. 22 of 129, 17.1%) was observed in polytrauma (p = 0.14). Thirteen cold injuries (13 of 202, 6.4%) were recorded during the study period: eleven (11 of 73, 15.1%) during summer and two (2 of 129, 0.1%) during the winter season (p < 0.001), even if subgroup analysis failed to find any seasonal difference in hypothermia (4 of 73, 5.4% vs. 5 of 129, 3.8%, p = 0.72) or frostbite (3 of 73, 4.1% vs. 1 of 129, 0.7%, p = 0.13) distribution. High Altitude Illness was observed in 27 of 73 (36.9%) patients in summer and 12 of 129 (9.3) in winter (p < 0.001), and subgroup analysis found a strong difference between seasonal AMS distribution (summer n = 27 of 73, 36.9% vs. winter n = 8 of 129, 6.2%, p < 0.001). No HACE episodes were observed during the study period. Further diagnosis details are reported in Table 2.
AMS, acute mountain sickness; HACE, high altitude cerebral edema; HAPE, high altitude pulmonary edema; MI, myocardial infarction; TIA, transient ischemic attack.
Outcome
More than half of patients (n = 104 of 202, 51.4%) were immediately discharged from ER and 17 of 202 (8.4%) after a 24-hour observation, irrespective of the season. Sixty-two patients (62 of 202, 30.6%) were hospitalized during the study period, with no difference in seasonal distribution. Forty-one patients (41 of 202, 20.3%) required ward care, with 3.1 ± 2.7 mean days of hospital stay: 29 of 202 (14.3%) were discharged, one transferred to another hospital and one deceased. Among the 21 of 202 patients (10.4%) requiring an intensive care unit, 9 of 202 (4.4%) were discharged to the ward, 11 of 202 (5.4%) transferred to another hospital or rehabilitative structure, and one of 202 deceased (0.5%). In summer and winter, 7 of 73 (9.5%) and 12 of 129 (9.3%) patients refused care, respectively (p = 0.92). Details are reported in Table 3.
D, days; ICU, intensive care unit.
Activity incidence and events risk
In the two summer seasons during the study period, 35 of 202 (17.3%) patients reported mountain-related injuries or illness during climbing activities, considering 16 daily climbing hours (8,788,576 exposure hours), corresponding to 0.004 mountain-related events per 1000 hours of mountain activity. Trekking activities involved 23 of 202 patients (11.4%), considering 8 hours per day (4 394 288 exposure hours), resulting in 0.005 mountain-related events per 1000 hours of mountain activity. Working activity, considered in summer and involving 4 of 202 (1.9%) patients 8 hours per day, had a risk of 0.001 mountain-related events per 1000 hours of mountain activity. Skiing, practised in winter and involving 139 of 202 (68.8%) patients during 6 hours per day (25,723,320 exposure hours), resulted in 0.005 mountain-related events per 1000 hours of mountain activity.
Considering events per season, in the summer season, 73 of 202 (36.1%) patients reported 88 events in 549,286 days, with a mean of 12 daily activity hours (6,591,432 exposure hours), summer events risk is 0.013 per person and 1000 hours. In winter, 129 of 202 (63.9%) patients reported 165 events in 4,287,220 days with a mean of seven activity hours per day (30,010,540 exposure hours), winter events risk amounts to 0.005 per person and 1000 hours. For further details, see Table 4.
Activity incidence rate is expressed as the occurrence of mountain-related events per unit of person time. Event incidence rate is expressed as the occurrence of new cases per person and 1000 hours of activity (event/1000 hours). Event total number of medical events or traumatic injuries reported. Daily hours = mean number of person hours considered per activity. Exposure days are calculated in summer season as the number of nights spent per person in a mountain refuge at >2500 m and in winter by the daily number of skiers attending to ski resort at >2500 m. Exposure time hours to calculate the event risk are calculated according to the mean hours spent per activity per number of days in altitude.
Discussion
Ninety eight point eight percent of the VdA area is characterized by mountain reliefs (3): 50.7% of them exceed moderate altitude (2000–3000 m) and 8.3% high altitude (>3000 m) (ISTAT, 2011). As an example, in both Switzerland and Austria, mountain distribution accounts for 72% of the total area. This geographical feature, associated to a 170% seasonal population increase, makes the VdA district a unique point of view for mountaineering and high altitude illness. The analysis of our reported cohort reveals how, despite an intense sport activity, medical or trauma events represent only 0.196% of ER access. Moreover, hundreds of athletes competing for the world's most challenging mountain ultramarathon (Tor des Geants) every September have to be added to the population at risk (Mrakic-Sposta et al., 2015).
The analysis of the literature reveals how a considerable rate of diseases related to mountain activity is represented by traumatic injuries: downhill cycling, skiing, or mountaineering is often responsible for head commotive injury or severe multiple trauma (Kim et al., 2006; Smith et al., 2006; Gammons et al., 2011; Ashwell et al., 2012; Schöffl et al., 2012). An observational study held in the French Alps reported 114 traumas in 2 years; 60% of them were due to winter sports, with a high incidence of cerebral and spine lesions (Jacquot et al., 2011). Our study confirms this observation, being trauma the most represented event (50.4%) in High Altitude, particularly head commotive injury during winter compared to the summer season (p < 0.001), probably a consequence of ski activities.
The relationship between high altitude and AMS, HACE, or HAPE is known, as well as the evolution to death if unrecognized and not properly treated (Basnyat and Murdoch, 2003). In our study, during summer, we observed significantly more high altitude illnesses (p < 0.001) and cold injuries (p < 0.001) than in winter, probably because summer alpine climbers are exposed to higher altitudes for longer periods with less protection than among winter skiers.
When focusing on the subgroup of High Altitude Illness, most part of the patients was affected by AMS (19.3%) and only four by HAPE (1.9%): the prompt rescue and short ground-to-hospital time span can explain these observations. We suppose that for the same reason, patients did not have the time to develop HACE. The heterogeneous population involved in recreational or professional mountaineering is not necessarily young, athletic, trained, or competent. Cold, intensive exercise, and hypoxia can—alone or in combination with cerebrovascular history and cardiovascular history—be responsible for stroke or MI (Burtscher et al., 1993; Ponchia, 2000; Wilson et al., 2011; Chan et al., 2012). Burtscher and coll. (Burtscher et al., 1993) observed how the risk of sudden cardiac death in men over the age of 34 years was increased by a factor of 4.3 during hiking and 2.1 during skiing. In our cohort, 19.8% of the events observed had a cardiac relevance, with a 10:1 ratio toward neurologic events. The consequence of physical exercise in altitude is elevation of stroke volume and heart rate, followed by enhanced oxygen extraction; while subclinical cardiopathy is highly susceptible to decompensate, little is known about epileptic threshold or brain hemodynamics in these settings.
Last, but not least, high altitude disease should not be neglected among professional workers, especially in the presence of mountain dockyards.
Conclusion
High altitude medical events or trauma represent <1% of ER accesses, even in a high-flow touristic mountain district. Head commotive injury is the most observed mountain-related event at high altitude, in winter and during ski practice. High altitude illness and cold injuries, even if rare, are observed more frequently in summer, during trekking or climbing activities. An alpine, multicentric prospective study might confirm our findings on the European alpine territory.
Footnotes
Acknowledgment
The authors owe their most important thanks to the outstanding support of Fondazione Montagna Sicura: Fosson JP, Trucco M, and Franco “Pillola” D. Founding: RESAMONT 2 Program of transboundary cooperation, France-Italy 2007–2013, Alcotra.
Author Disclosure Statement
No competing financial interests exist.