
Abstract
Abstract
Phillips, Lara, Buddha Basnyat, Yuchiao Chang, Erik R. Swenson, and N. Stuart Harris. Findings of cognitive impairment at high altitude: relationships to acetazolamide use and acute mountain sickness. High Alt Med Biol. 18:121–127, 2017.
Objective:
Acute mountain sickness (AMS) is defined by patient-reported symptoms using the Lake Louise Score (LLS), which provides limited insight into any possible underlying central nervous system (CNS) dysfunction. Some evidence suggests AMS might coexist with altered neural functioning. Cognitive impairment (CI) may go undetected unless a sensitive test is applied. Our hypothesis was that a standardized test for mild CI would provide an objective measure of CNS dysfunction, which may correlate with the symptoms of AMS and so provide a potential new tool to better characterize altitude-related CNS dysfunction. We compared a cognitive screening tool with the LLS to see if it correlated with CNS dysfunction.
Methods:
Adult native English-speaking subjects visiting Himalayan Rescue Association aid stations in Nepal at 3520 m (11,548 ft) and 4550 m (14,927 ft) were recruited. Subjects were administered the LLS and a slightly modified version of the environmental Quick mild cognitive impairment screen (eQmci). Medication use for altitude illness was recorded. Scores were compared using the Spearman's correlation coefficient. Data also included medication use.
Results:
Seventy-nine subjects were enrolled. A cut-off of three or greater was used for the LLS to diagnose AMS and 67 or less for the eQmci to diagnose CI. There were 22 (28%) subjects who met criteria for AMS and 17 (22%) subjects who met criteria for CI. There was a weak correlation (r2 = 0.06, p = 0.04) between eQmci score and LLS. In matched subjects with identical LLS, recent acetazolamide use was associated with significantly more CI.
Conclusion:
Field assessment of CI using a rapid standardized tool demonstrated that a substantial number of subjects were found to have mild CI following rapid ascent to 3520–4550 m (11,548–14,927 ft). The weak correlation between the LLS and eQmci suggests that AMS does not result in CI. Use of acetazolamide appears to be associated with CI at all levels of AMS severity.
Introduction
A
Previous work has suggested there might be cognitive impairment (CI) in AMS, although data are not very convincing. While it is known that high-altitude conditions can impair cognition, and alter executive, memory, and language processes (Kramer et al., 1993; McCarthy et al., 1995; Wu et al., 1998; Du et al., 1999; Li et al., 2000; Virues-Ortega et al., 2004; Petrassi et al., 2012; Asmaro et al., 2013; Turner et al., 2015), generally, it does not appear that AMS is necessary to have CI (Kramer et al., 1993; Virues-Ortega et al., 2004). However, some studies do suggest that CI and AMS are linked (Forster, 1985; Regard et al., 1991; Shukitt-Hale et al., 1991; Bian et al., 2015; Issa et al., 2016). AMS is thought to be due to early, mild cerebral edema and increased intracranial pressure (Lawley et al., 2016; Sagoo et al., 2017), although other theories exist. Cerebral manifestations of acute altitude illness span from common, benign AMS to potentially fatal high-altitude cerebral edema (HACE). More obvious clinical neurological findings (e.g., ataxia, alterations in consciousness, and confusion) are found in HACE, but not in AMS. Because high-altitude cerebral illnesses appear to be a continuum from the mild central nervous system (CNS) symptoms of AMS to severe symptoms with overt CNS findings of HACE, our hypothesis was that a sensitive objective test for high-altitude-related mild CI using an easily available field technique would correlate closely with the presence and severity of AMS.
The Quick mild cognitive impairment screen (Qmci) has potential to detect mild CI in the field at high altitude. The Qmci screen rapidly and reliably detects early mild CI and is more sensitive when compared with the Standardized Mini Mental State exam (Molloy et al., 2005; O'Caoimh et al., 2012). We tested a slightly modified version of the Qmci [which we refer to as the environmental Qmci (eQmci)] and sought to determine that if AMS causes CI, the eQmci might serve as a possible screening test for AMS. We compared these data to the LLS and use of concomitant drugs for prophylaxis of AMS.
Methods
Study population
All of our subjects had recently and rapidly ascended by vehicle and foot to the two testing sites in the Annapurna region of the Nepalese Himalayas. Those adult native English-speaking subjects visiting the Himalayan Rescue Association aid station in Manang at 3520 m (11,548 ft) or at a temporary aid station in Thorong Phedi at 4550 m (14,927 ft) were offered enrollment into the study. Surveys were only offered to clinically stable subjects at the end of their medical visit after clearance from the health professional caring for them. Inclusion criteria included native English-speaking adults between the ages of 18 and 65 years trekking through Manang or Thorong Phedi. This included asymptomatic subjects who presented themselves to the clinic for education and prevention of illness. Subjects were not excluded for having symptoms of AMS or minor ailments, including joint pain, blisters, rashes, diarrhea, and cough. Exclusion criteria included a history of dementia, a lack of native fluency in English, recreational drug or alcohol use, and outside the age range. The discriminating power of the Qmci for detecting CI is influenced by age; specifically it is less accurate for subjects older than 75 years (O'Caoimh et al., 2014). We chose a more conservative threshold of 65 years to reduce the potential confounding influence of age on CI. All recruited subjects were trekkers who had acutely ascended within 1 week. No permanent residents of high altitude were recruited.
Study procedures
A convenience sample of subjects who presented to the aid stations was enrolled. A consent document with information about the study was presented to each volunteer and written consent was obtained. Information collected from each subject included age, years of education, history of dementia, fluency in English, rate of ascent, medication use, and self-rated high-altitude experience. Subjects were asked about prophylactic and treatment medications for high-altitude illness, analgesics, and any potentially sedating drugs during their trek through the Annapurna region. Medications for general medical problems (e.g., antihypertensives, oral contraceptives, thyroid replacement, etc.) were not recorded. Each subject enrolled was administered the LLS and eQmci by a single investigator. This study was approved (Protocol No. 2014P001803) by the Partners Institutional Review Board (Boston, MA) and the Nepali Health Research Council.
Screening tests
The LLS uses a 5-item scale, which surveys a subject's assessment of headache, dizziness or lightheadedness, fatigue or weakness, gastrointestinal distress, and difficulty sleeping. Each symptom is graded on a scale of 0 (not present) to 3 (severe). The presence of a headache (score at least 1 for headache) and a total score of ≥3 is required to diagnose AMS (Roach et al., 1993).
The Qmci consists of 6 subtests, including orientation, registration, clock drawing, delayed recall, verbal fluency, and logical memory. It has a median administration time of 4.24 minutes (O'Caoimh et al., 2013). The range of score is 0 to 100. Two modifications were made to better apply this screen in high-altitude wilderness settings. We removed the clock drawing task, given the practical concern of needing to remove gloves to perform the test in a very cold environment. The clock drawing test is useful to assess visuospatial cognition, but is clinically a less useful subtest when compared with other elements in the Qmci (O'Caoimh et al., 2013). Instead, to maintain a distracting task before the verbal recall exam, subjects were asked to count backwards from 100 by 7. A second modification was made in which proper names replaced common names for repetition and recall testing. Proper names were matched for frequency of occurrence in the English language. High altitude seems to have a more dramatic effect on the recall of proper names, whereas recall of common names is relatively resistant to hypoxia (Pelamatti et al., 2003). The remaining subtests were unchanged. Subjects with normal cognition have a median score of 75 (O'Caoimh et al., 2014). Subjects who score ≤67 out of 100 meet criteria for mild CI and those who score ≤53 out of 100 meet criteria for dementia (O'Caoimh et al., 2014). These cut-offs are influenced by age and education and are recommended for younger adults (≤75 years) with more education (≥high school). At this cut-off, the Qmci has an 86% sensitivity and 89% specificity for detecting the presence of mild CI. CI is not seen in a young, healthy, and educated population (D.W. Molloy, 2015. pers. comm.). Sex does not significantly affect cut-off scores (O'Caoimh et al., 2014).
Statistical analyses
Continuous variables were summarized using mean with SD and compared using two-sample t-tests, whereas categorical variables were summarized using frequency and percentage and compared using chi-square tests. The relationship between the two measures was summarized using a Spearman's correlation coefficient. Two-sided p ≤ 0.05 was considered as statistically significant. All analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Seventy-nine subjects were enrolled in the study. All subjects who enrolled completed the surveys. Twenty-two subjects (28%) met criteria for AMS and 17 subjects (22%) met criteria for mild CI.
Table 1 presents demographic subject information stratified by the presence of AMS and CI. We found a significant difference in recent acetazolamide use between groups with and without AMS. Twenty-three out of 79 (29%) took acetazolamide in the last 24 hours. Of these subjects, 10 (43%) had AMS and 11 (48%) had CI. A higher percentage of subjects diagnosed with AMS had taken acetazolamide in the last 24 hours compared with those without AMS (45% vs. 23%, p = 0.047). Similarly, a higher percentage of subjects with CI had taken acetazolamide in the last 24 hours compared with those without CI (65% vs. 19%, p = 0.0003). Subjects with CI were slightly older (37 ± 14 vs. 29 ± 9, p = 0.058) and there were no other meaningful or significant differences in group characteristics (e.g., age, sex, nationality, education, days above 8000 ft, self-rated experience at high altitude, and paracetamol and nonsteroidal anti-inflammatory use) in subjects with and without AMS, or with and without CI.
Percentages are reported with respect to different subgroups (LLS <3, LLS ≥3, eQmci >67, eQmci ≤67).
eQmci, environmental Quick mild cognitive impairment screen; LLS, Lake Louise Score; NSAID, nonsteroidal anti-inflammatory drugs; SD, standard deviation.
As this study tested subjects at two different altitudes, we also analyzed the results from only Manang, where the majority of subjects were recruited (n = 62). When subjects from Thorong Phedi were excluded, there was still a significant difference in recent acetazolamide use between groups with and without AMS. Specifically, a higher percentage of subjects diagnosed with AMS had taken acetazolamide in the last 24 hours compared with those without AMS (44% vs. 13%, p = 0.009). Similarly, a higher percentage of subjects with CI had taken acetazolamide in the last 24 hours compared with those without CI (54% vs. 12%, p = 0.001). There were no other significant differences in group characteristics.
There was a very weak correlation between the eQmci score and LLS based on the Spearman's correlation coefficient (r = −0.24, p = 0.04) as only 5% of the variance in the eQmci can be attributed to LLS (Fig. 1). Among the 79 subjects, 6 (8%) tested positive for both AMS and CI and 46 (58%) tested negative for both. Sixteen subjects (20%) met the LLS criteria for AMS, but had no CI. The remaining 11 subjects (14%) were cognitively impaired, but did not have AMS. Those with concordance between the eQmci and LLS were more likely to be male (69% vs. 41%, p = 0.014) and there was no other significant difference in subject demographic characteristics between those with and without concordance between the eQmci and LLS.

A scatter plot was created between LLS and eQmci scores. There was poor correlation between the eQmci score and the LLS based on the Spearman's (−0.24) correlation coefficients. eQmci, environmental Quick mild cognitive impairment screen; LLS, Lake Louise Score.
Components of the LLS were also analyzed as presented in Table 2. There was no strong correlation between the eQmci score and any of the LLS components, including headache. The strongest correlation was seen in gastrointestinal symptoms, which was still relatively weak (r = −0.28, p = 0.011).
Analysis is demonstrated with relatively weak correlation.
We conducted a further analysis to examine the effect of acetazolamide on eQmci score. Figure 2 shows the distribution of eQmci from those subjects with and without acetazolamide use in the last 24 hours. The overall mean eQmci scores were lower in subjects who took acetazolamide (69 vs. 77, p = 0.0007). The finding was consistent when limited to subjects with the same LLS score. Table 3 compares the prevalence of CI from subjects with and without acetazolamide use in the last 24 hours. Overall, CI were more common among subjects with acetazolamide use (47.8% vs. 10.7%, p = 0.0006). When stratified by AMS status, the finding remained consistent. Among those without AMS, CI was significantly more frequent in subjects who took acetazolamide than in subjects who had not taken the drug (46.2% vs. 11.4%, p = 0.011). Similarly, among subjects with AMS, those who took acetazolamide had more CI (50.0% vs. 8.3%, p = 0.056) than those who had not taken the drug.
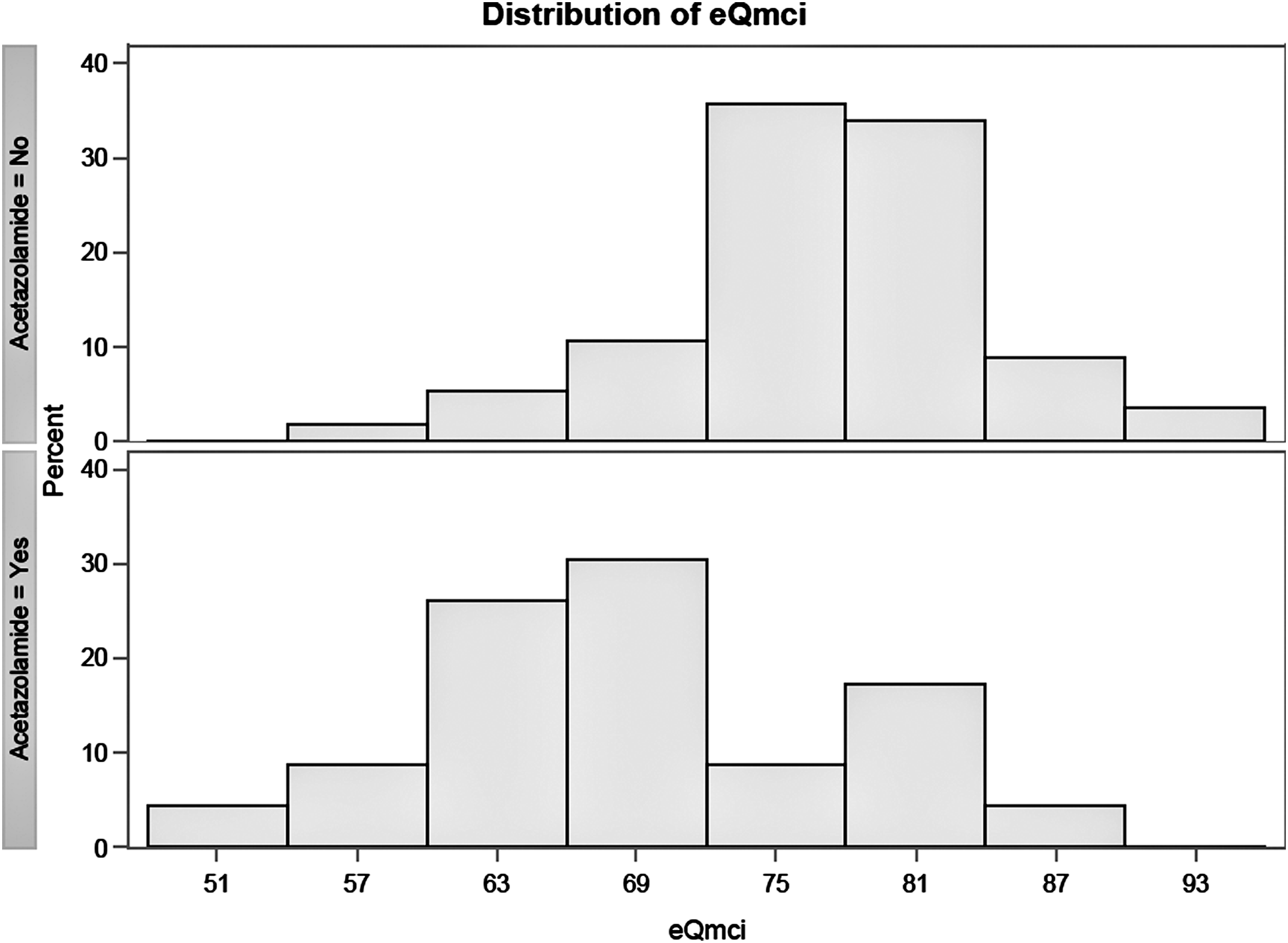
A graphic display of the range of values for the eQmci in subjects with and without acetazolamide use in the last 24 hours. eQmci scores were lower in subjects who took acetazolamide (p < 0.001).
The overall mean eQmci scores were significantly lower in subjects who took acetazolamide.
AMS, acute mountain sickness.
Discussion
Acute ascent to high altitude can impair CNS function, including short-term memory, working memory, and executive functioning (Petiet et al., 1988; Hornbein et al., 1989; Kennedy et al., 1989; Kramer et al., 1993; Shukitt-Hale et al., 1994; Virues-Ortega et al., 2004; de Aquino Lemos et al., 2012; Petrassi et al., 2012; Asmaro et al., 2013; Turner et al., 2015). We hypothesized that an easily performed field test for mild CI would provide an objective measure of altitude-related CNS dysfunction, which would correlate closely with the presence and severity of AMS. Our results do not suggest a significant correlation between the eQmci and LLS to support this hypothesis.
Our study found a surprisingly high prevalence of CI: 17 subjects (22%) met criteria for mild CI. In subjects with a similar age range to our study, no subjects tested at sea-level were found to have CI (D.W. Molloy, 2015. pers. comm.). Incidentally, we found that acetazolamide use, independent of the severity of AMS, was associated with CI at high altitude.
Lack of relationship between CI and AMS
The lack of correlation between the LLS and eQmci suggests that CI occurs independently of AMS. This is consistent with previous research (Virues-Ortega et al., 2004). Kramer et al. (1993) tested 20 climbers at 4360 m (14,304 ft) ascending Denali. While they demonstrated deficits in learning and retention in perceptual and memory tasks, they did not correlate with AMS. In one study that tested mental capacity, subjects with AMS were worse in pursuit aiming compared with subjects without AMS, but in the remaining battery of cognitive tests, no significant differences were found (Bian et al., 2015). It is possible that there is a difference in the aspects of cognitive deficits seen with and without AMS. In the study by Regard et al. (1991), subjects simulated ascent to 4500 m (14,734 ft) over 24 hours in a hypobaric chamber. Those with AMS were deficient in short-term memory, but improved in conceptual tasks, whereas those without AMS had improved short-term memory, but no improvement in conceptual tasks (Regard et al., 1991).
Acetazolamide and CI
In subjects taking acetazolamide, we found a high incidence of AMS and of CI. Acetazolamide has been associated with confusion (Swenson, 2014). In a randomized study of subjects at high altitude, subjects who received prophylactic acetazolamide (125 mg twice per day) had impaired neuropsychological measures of concentration, cognitive processing speed, reaction time, short-term memory, and working memory (Wang et al., 2013). In a similar study, subjects who took acetazolamide (500 mg slow release, once per day) actually showed improvement in certain psychological tests (White, 1984). In addition to higher daily acetazolamide dosing, this second study differed from the former in that subjects traveled on foot rather than being airlifted to a higher altitude, which may be a confounding factor. A more recent study found that at sea level, acetazolamide use is associated in a dose-dependent fashion with a spectrum of psychometric impairments, including poor concentration, imbalance, and slower reaction time responses (Collier, 2016). Our study did not differentiate between prophylactic or treatment doses, but a future study can be designed to match groups with regard to this variable. Carbonic anhydrase (CA) plays a role in signal processing, synaptic plasticity, memory, nerve conduction, and cerebral oxygenation and consumption (Brechue et al., 1997; Sun and Alkon, 2002; Wang et al., 2015). Given these findings, CA inhibition is likely responsible for the deficits in cognition. Whether CI arises from the drug-induced metabolic acidosis that partially relieves the magnitude of the respiratory alkalosis (hypocapnia) or from more direct effects in the CNS is not easily resolved, but both may be likely. At sea level only 50% of patients taking acetazolamide (250 mg, 4 times a day) have relief of common CNS side effects with concurrent bicarbonate supplementation sufficient to correct the metabolic acidosis (Lichter, 1981).
Limitations of the study
There are several limitations in this investigation. First, we made modifications to the eQmci (the clock drawing task was replaced by reciting serial 7 and the repetition and recall of names were changed from common to proper). Although the Qmci has been validated against the Montreal Cognitive Assessment and Standardized Mini-Mental State Exam, the two minor changes in the eQmci were not validated before testing. This potentially could have an effect on the cut-off values originally tested for the Qmci. Second, traveling to a distant, culturally different location may alter one's performance on a cognitive test. Third, given the relatively small subject recruitment, other trends may be seen with a more robust sample. Unfortunately, our recruitment was limited as a result of the devastating 2015 earthquake in Nepal, which resulted in termination of the study. Fourth, there may be several secondary influences on neuropsychological function, including fatigue, hypothermia, desynchronosis, upper respiratory infections, and exposure to a new environment. An individual diagnosis was not recorded for every patient; however, most presentations to the clinic that were unrelated to altitude were quite minor (e.g., blisters) and would not be expected to affect cognitive function. Fifth, there was neither a low-altitude control group, nor were our subjects tested at low altitude to examine baseline scores. Sixth, there were no measurements of arterial oxygenation saturation by pulse oximetry. In future studies, this would be a better indicator of cerebral hypoxic stress than the actual altitude. Seventh, there were no longitudinal data to determine if low eQmci scores correlate with the development of HACE. Future research is needed to define the clinical significance of mild CI and to determine whether it can it be used to predict those that will develop HACE or experience other clinically relevant sequelae. In addition, there were no longitudinal data on the discontinuation of acetazolamide. Eighth, subjects were studied at two different altitudes. However, the results were not significantly changed when data were limited to Manang, where most subjects were tested. Ninth, in a convenience sample, in which subject self-selection exists (researchers have no control or insight in subjects' decisions to continue to ascend or not), unmeasured confounding variables may exist that could reduce the validity of our conclusions.
Future studies
Regardless of AMS, screening of mild CI may be useful for early detection of impaired cognition and poor decisional judgment at high altitude. Our study, however, does not demonstrate any clinical significance of having mild CI diagnosed by a cognitive function test, since we did not measure rates of adverse health events or poor decision making, but this is a potential area of future research. Cognitive tests are sensitive and have the potential to screen for hypoxic impairment at early stages before subjects develop symptoms or demonstrate poor judgment (Stepanek et al., 2013). Other cognitive tests have been employed at high altitude such as clock drawing (Quigley and Zafren, 2016). The eQmci can be administered in <5 minutes, does not require any special equipment, and has multiple versions available to minimize a learning effect when administered to the same subject over different points in time (Cunje et al., 2007). Future longitudinal studies in trekkers, as well as validation of the eQmci and comparison to other cognitive tests, may be useful to investigate the clinical relevance of mild CI. Further study of secondary influences on CI at high altitude (e.g., exercise, medications, and sleep quality) is also needed. Finally, the comparison of CI with other objective measures (e.g., optic nerve sheath diameter, magnetic resonance imaging, and serum biomarkers) might help advance a better understanding of acute altitude-related CNS disease.
In summary, our data demonstrate only a weak correlation between the LLS and eQmci, but a surprising prevalence of CI, an objective measure of CNS dysfunction, at high altitude. CI was prevalent in subjects both with and without AMS. The presence of CI in otherwise asymptomatic trekkers raises concerns for unrecognized CI at altitude. Furthermore, we found that acetazolamide use, independent of the severity of AMS may also contribute to the presence of CI at high altitude. Further research using CI testing may help define objective measures of early CNS dysfunction at altitude.
Footnotes
Acknowledgments
The authors are grateful to Dr. Willie Molloy, Dr. Ronan O'Caoimh, Anthony Brohan, Dr. Marjorie Nicolas, Dr. Remi Drozd, Dr. Allison Mulcahy, and Emily Ledingham for their contributions to the success of this study.
Author Disclosure Statement
No competing financial interests exist.