
Abstract
Abstract
West, John B. Cognitive impairment of school children at high altitude: the case for oxygen conditioning in schools. High Alt Med Biol. 17:203–207, 2016.—The hypoxia of high altitude frequently affects cognitive function. Recent work has shown that high altitude impairs the neuropsychological function of children of school age when compared with a similar control group of children at low altitude. This implies that the learning process is compromised at high altitude. One option is to bus children down to a lower altitude for schooling, but this is generally impracticable. Recently the new technique of oxygen conditioning has been introduced. The procedure is similar to air conditioning except that instead of altering the temperature of the air, the oxygen concentration is increased, thus raising the PO2 in the inspired air of classrooms. The result is that the children are physiologically at a lower altitude. Just as in very hot or cold climates, it is now unacceptable to have schools that are not air conditioned; in the future the same may apply to schools at high altitude that are not oxygen conditioned.
The Effects of High Altitude on Neuropsychological Function
A
Since then, very extensive neuropsychological studies have been carried out at high altitude, for a review see Yan (2014). These include psychomotor performance emphasizing accuracy and speed, perceptive functioning such as reaction times and color perception, memory including learning, retrieval versus storage functions, spatial memory, and short-term memory, and frontal lobe functions, for example, verbal fluency. Many of these measurements are very technical and need to be carried out under the supervision of professional psychologists.
In general, the degree of neuropsychological impairment is closely related to altitude (Yan, 2014). For example, at low altitudes, complex perception may be the only abnormality, whereas at very high altitudes some subjects even develop hallucinations (Brugger et al., 1999). The lowest altitude at which some neuropsychological impairment has been noted is about 1500 m, where alterations in complex perception have been described (Denison et al., 1966). Typically some cognitive impairment is seen above about 2500 m, but this becomes more marked above about 3500 m. In general, the changes are reversible on returning to low altitude, but residual impairment of neuropsychological function has been reported in climbers after ascent to extremely high altitudes such as 8000 m (Townes et al., 1984; Hornbein et al., 1989). Table 1 shows the altitudes of some of the highest cities in the world with their populations.
Recent Studies of Neuropsychological Function in Children at High Altitude
The majority of measurements of neuropsychological function that have been made are in adults. Only recently have children attracted much attention. There is a considerable literature on the physical development of children at high altitude, but the number of studies on neuropsychological function is very limited.
Hogan et al. (2010) described the physiological, cognitive, and behavioral profiles of 168 children and adolescents at three different altitudes in Bolivia. The subjects consisted of infants (6–12 months), children (6–10 years), and adolescents (13–16 years). These three groups were studied at altitudes of ∼500, 2500, and 3700 m, the last altitude being that of La Paz. The most important finding was a reduction in psychomotor speed with increasing altitude. Specifically, a finger-tapping test recorded the number of taps that could be made by the dominant hand in a given time, and it was found that this decreased with increasing altitude. The same result was found for a Processing Speed Index involving the matching and copying of figures. This also showed a decline with increasing altitude. The authors attributed the changes to an adaptive process that allowed the subjects to maintain accuracy of their mental processes in hypoxic conditions by reducing the speed of the response.
These measurements were extended in another study that compared neuropsychological function in 62 Bolivian children living either in La Paz, altitude 3700 m, or in El Alto, altitude 4100 m (Virués-Ortega et al., 2011). The results showed that at the higher altitude, there was the same reduction in neuropsychomotor speed compared with a lower altitude as had been measured previously in La Paz. However, in addition, executive functions including complex perceptual skills, reasoning, and verbal fluency were also impaired by the additional ascent of 400 m. Cerebral blood flow velocity was measured using a transcranial Doppler technique in the previous study (Hogan et al., 2010), and the additional changes caused by the higher altitude were ascribed to a loss of cerebral autoregulation. A possible alternative explanation is simply that the more severe cerebral hypoxia associated with the higher altitude caused additional impairment of brain function.
Recently an extensive study was carried out by a Swiss group (Rimoldi et al., 2016). This was in two parts. In the first, 48 children and adolescents aged between 10 and 17 years were studied first at the low altitude of 568 m in Lausanne, and the second after traveling by train to a high-altitude research station on the Jungfraujoch, altitude 3450 m. Studies were carried out 24 hours after arrival at high altitude, and a large battery of neuropsychological tests was used. These included executive function (inhibition, shifting, and working memory), memory (verbal short term, visuospatial, and verbal episodic memory), as well as verbal speed processing ability. These tests are part of well-established protocols and the original publication should be consulted for details.
The results showed that the short-term hypoxia associated with ascent from 568 to 3450 m caused significant impairment of five of the seven abilities that were tested. Only visuospatial memory (Corsi Block) and processing speed (TMT part A) were not significantly altered. Repeat measurements were then made 3 months after returning to the lower altitude of 568 m and it was found that the changes caused by high altitude were reversed and that the measurements were normal.
In the second part of the study, another set of measurements were made on 21 healthy European children and adolescents aged between 11 and 17 years who were born at sea level but had been living permanently in La Paz, Bolivia (3500 m) for over 3 years. The high-altitude exposure of this group began between the ages of 6 months and 6 years. The parents of the children were businessmen and engineers working in La Paz, and it was claimed that this high-altitude group of children had a similar education level and cultural and socioeconomic background as the group tested on the Jungfraujoch.
It was found that these children with the long-term high-altitude exposure had comparable or even more severe neuropsychological impairment than the group exposed to short-term hypoxia in Switzerland. For example, the alteration of visuospatial memory ability was significantly more severe after the long-term altitude exposure than the short-term altitude exposure, although this was not the case for digit span. Figure 1 shows some of the results from both the short-term and long-term altitude exposures.
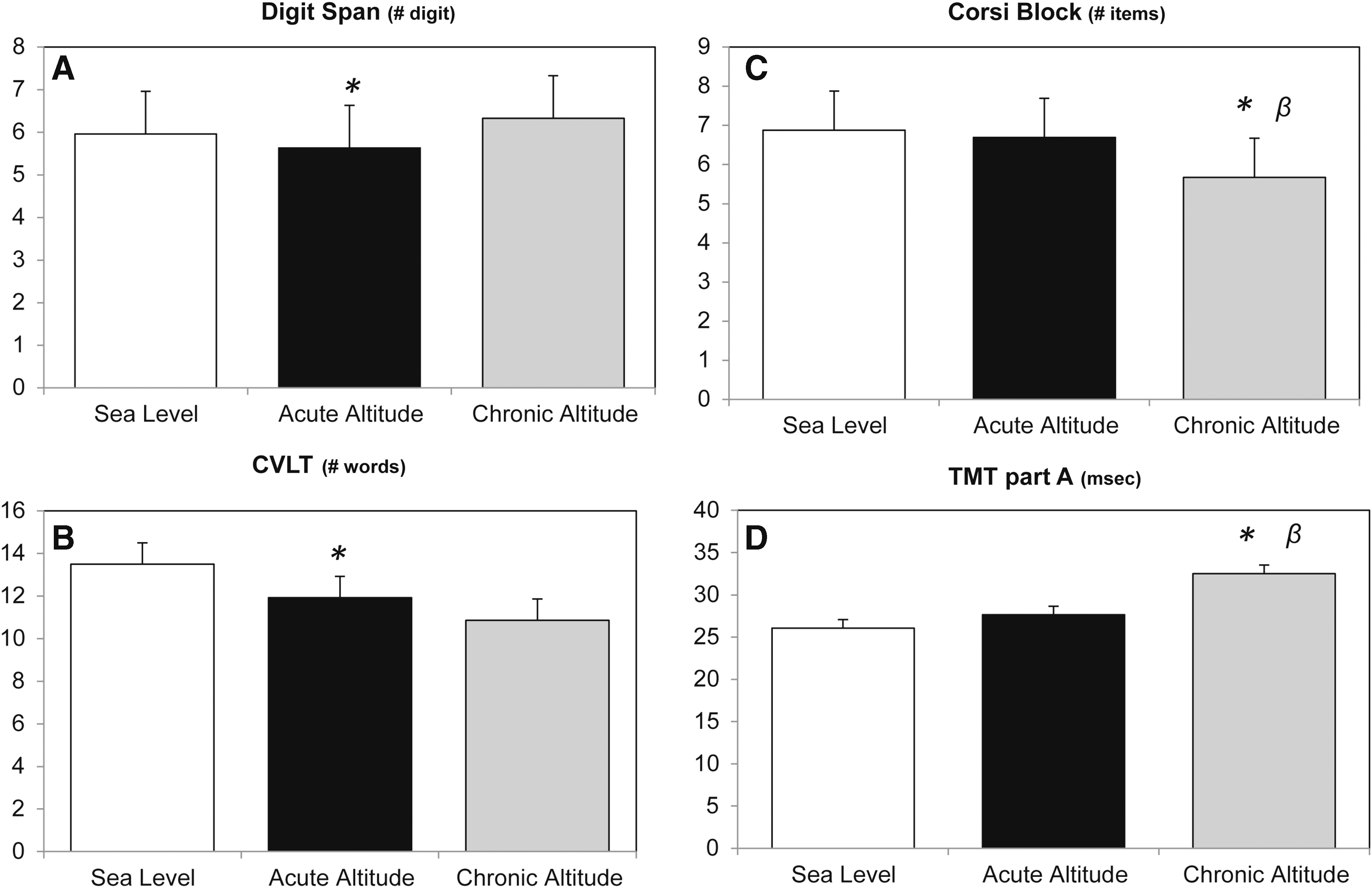
Results of neuropsychological tests in children of school age following both acute and chronic exposure to high altitude. Acute exposure was on the Jungfraujoch, altitude 3450 m, and chronic exposure was in La Paz, Bolivia, altitude 3500 m.
These provocative findings need to be confirmed but the results are consistent with those of the other studies already discussed. It should also be noted that abnormal neuropsychological function has also been described in children with chronic hypoxemia caused by lung or heart disease (Bass et al., 2004; Raman et al., 2006; Matos et al., 2014).
Changing Attitudes Toward the Physical and Mental Function of People at High Altitude
It is generally accepted that many visitors to high altitude have impaired neuropsychological function. The same is true of so-called sojourners, that is, people who are originally from low altitude but are living and working at high altitude for several years. However, the traditional view has been that most permanent residents are well adapted to their high-altitude environment. For example, many have been there for generations, and they apparently live and work as effectively as people at low altitudes. It is true that some permanent residents develop chronic mountain sickness but these are a minority. In fact, medical students are often taught that high altitude is a classical example of how the human body successfully adapts to a potentially hostile environment. For example, in a study of residents of Morococha in the South American Andes at the very high altitude of 4600 m, the arterial PO2 was found to be only 45 mmHg with an oxygen saturation of only 81%, but because of a combination of hyperventilation and polycythemia, the PO2 of mixed venous blood was calculated to be only about 7 mmHg below that of sea-level dwellers (Hurtado, 1964).
Recently, however, the degree of adaptation to high altitude has been increasingly questioned. Actually nearly 100 years ago, the British physiologist Barcroft (1925) famously stated that all dwellers at high altitude are persons of impaired physical and mental powers. At the time, the statement was fiercely criticized, notably by Monge (1948) who saw Barcroft's remarks as a slur on Peruvian highlanders, but much evidence now supports his assertion.
Here it is useful to divide people at high altitude into three groups. The first are visitors who come from low altitude and typically only spend a few weeks at high altitude. The next group are sojourners. These are people who originally came from low altitude but find themselves living or working at high altitude for several years. Finally there are the permanent residents who have typically been at high altitude for generations.
We now know that all three groups improve their work capacity as measured by their maximal oxygen consumption if they move to a lower altitude. Some people are surprised to learn that this is true of permanent residents but the evidence is overwhelming (Elsner et al., 1964; Favier et al., 1995). On physiological grounds, this is not surprising because moving to a lower altitude presumably increases the PO2 of all tissues in the body, including the exercising muscle.
When we turn to neuropsychological function, the situation is less clear. Certainly this is improved in visitors to high altitude if they go to a lower altitude. Also although there are relatively few measurements, the evidence is that the same is also true of sojourners. But what is fascinating is that recent studies also indicate that some permanent residents have reduced cognitive function compared with a comparable group at lower altitude. This somewhat contentious issue has been reviewed by Yan (2014) and is mainly based on measurements of neuropsychological function in matched groups of people living at low and high altitudes.
So the general conclusion is that Barcroft's bold assertion was essentially correct. All three groups, visitors, sojourners, and permanent residents improve their physical powers by moving to a lower altitude, and the first two groups have an improvement in mental power. The jury is still out on to what extent this last applies to permanent residents.
How Can We Counter the Negative Effects of High Altitude on Neuropsychological Function?
The impairment of neuropsychological function at high altitude is caused by the inevitable hypoxia resulting from the low barometric pressure. Few options are available to deal with this. In the context of improving the learning environment of school children, one option is to move the teaching to a lower altitude and this may be feasible in some parts of the world. For example, in the South American Andes, rapid changes in altitude can occur over short distances and it might be feasible in some instances to bus children down to classrooms at a lower altitude. However, this is only practicable in very selected areas.
For children who are required to remain at high altitude, it might be possible to raise the oxygen concentration in the air of some critical rooms by the technique of oxygen enrichment. This was first described about 20 years ago (West, 1995) and is now used in many parts of the world, particularly in dormitories, offices of very high-altitude telescopes, and even in some upscale hotels. In addition, some people have arranged to have the bedrooms of their houses oxygen enriched in high altitude ski resorts to improve sleep.
However, the most promising technique for improving neuropsychological function of children in schools is to oxygen condition the whole school. This raises the oxygen concentration of the air throughout the institution and, in effect, transports everybody to a lower altitude. Initially this may be regarded as a very ambitious undertaking. However, air conditioning of schools in hot climates is a well established procedure. It would be inconceivable to have schools in parts of Texas, for example, that were not air conditioned during the summer. Oxygen conditioning can be regarded in a similar way. Whereas the hot climate interferes with the well-being and work efficiency of students in some areas, high altitude does the same in principle. And the solution can be the same except that rather than cooling the air, oxygen is added to it. Advances in technology have now made this feasible.
Principles of Oxygen Conditioning
Oxygen conditioning increases the PO2 in the inspired air of a building and, in effect, reduces the altitude to which people are exposed. The term oxygen conditioning emphasizes the analogy with air conditioning. Although the latter reduces the temperature of the air in a hot climate and thus improves working conditions, oxygen conditioning raises the PO2 of the air and, therefore, the living and working environment of people at high altitude. The effectiveness of oxygen conditioning is remarkable. For example, increasing the oxygen concentration in the air by 1%, for example, from 21% to 22%, reduces the equivalent altitude by about 300 m. The equivalent altitude is that which gives the same inspired PO2 for air breathing. As an example, children in a school in La Paz, altitude 3650 m, can have the effective altitude reduced to that of Denver, altitude 1610 m, by raising the oxygen concentration of the rooms by only 6%. Closer to home, schoolchildren in Leadville, CO, who are at an altitude of 3094 m can be effectively transported to the altitude of Denver by increasing the oxygen concentration by only 3%. Figure 2 shows the extent to which the equivalent altitude can be reduced by various oxygen concentrations in rooms for various actual altitudes.
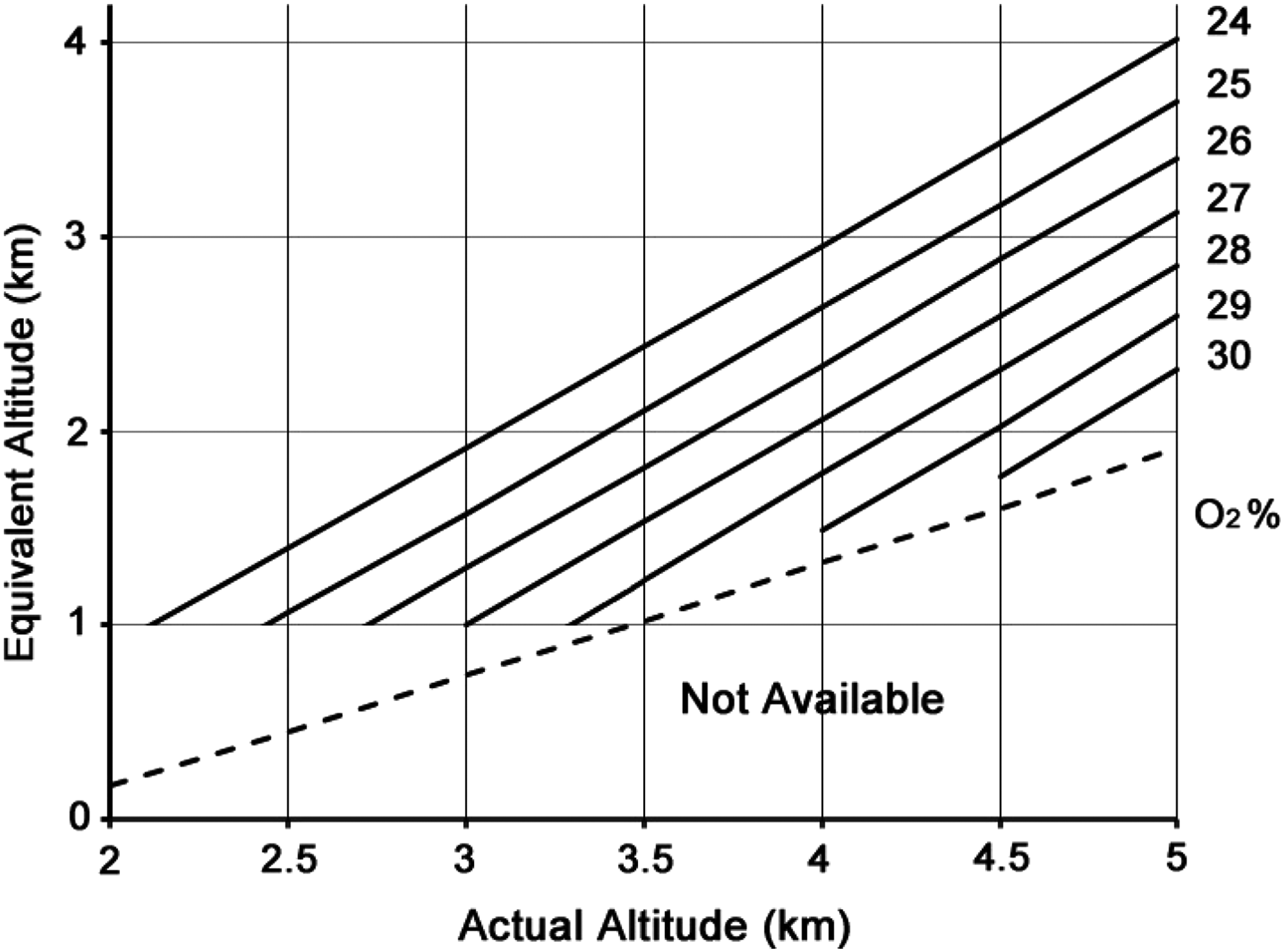
Equivalent altitudes are shown for the actual altitudes and the oxygen concentration in the air. Equivalent altitude is that which gives the same inspired PO2 during air breathing. Note that the bottom section of the diagram under the broken line is not available because of the National Fire Protection Agency guidelines. Modified from West (2015).
An issue that is often raised by people when they first hear of this technique is the fire hazard. This is certainly an important topic, and it has been thoroughly studied by the National Fire Protection Association (1999). The important conclusion is that the equivalent altitude can be substantially reduced without incurring a fire hazard. In this context, it should be emphasized that oxygen conditioning never raises the PO2 in the air above the normal sea level value. In other words the equivalent altitude is never reduced all the way to sea level, but the reduction that does occur greatly reduces the physiological problems associated with high altitude.
Oxygen conditioning of a large facility such as a school requires the generation of large amounts of oxygen. However, the technology to do this is now available. Many industries use very large amounts of oxygen. Examples are the paper pulp industry, fish farming, wastewater treatment, and many industrial chemistry processes. The oxygen is obtained from the air using a synthetic zeolite that preferentially adsorbs the nitrogen when the air is compressed, thus producing large amounts of almost pure oxygen. As an example, generators that produce 5000 L/min of 93% oxygen are now available (PCI Gases, Riverside, CA). In many institutions, the ducting that is in place for normal ventilation and air conditioning can be used.
In summary, there is increasing evidence that schoolchildren at high altitude have some cognitive impairment because of hypoxia, and presumably this interferes with the learning process. The solution proposed here is to effectively reduce the altitude of the schoolroom by adding oxygen to the air. Although at first sight this may appear to be an extreme solution, it is no different in principle from what is done in all very hot and cold climates, which is to change the temperature of the air by air conditioning.
Footnotes
Author Disclosure Statement
No competing financial interests exist.