
Abstract
Abstract
Otero, Liliana, Patricia Hidalgo, Rafael González, and Carlos A. Morillo. Association of cardiovascular disease and sleep apnea at different altitudes. High Alt Med Biol. 17:336–341, 2016.—We evaluated the prevalence of sleep apnea (SA) in patients with cardiovascular disease (CVD) at different altitudes. A total of 398 subjects with coronary artery disease (CAD), 144 subjects with atrial fibrillation (AF), and 292 controls (without CVD) were recruited in three cities at sea level, moderate altitude, and high altitude. All participants underwent polysomnography. Multinomial logistic regression, X2, and Hosmer and Lemeshow tests were used to determine interactions among CVD, SA, and altitude. Men and women with CVD at high altitude had a higher risk for SA than men and women living at lower altitudes. The highest risk of SA was observed in men with AF and men with CAD living at high altitude. Obstructive SA (OSA) prevalence was significantly increased in CVD subjects living at high altitude (OR: 5.52; p < 0.0001). Central SA (CSA) was more frequent in subjects with CVD than control group (OR: 2.44; p < 0.021). OSA was the most frequent type of SA in subjects with CVD and overweight subjects, and in control individuals with obesity or being overweight. Significant differences in the prevalence of SA associated with altitude and gender were noted in subjects with CAD and AF.
Introduction
C
Sleep-disordered breathing may be classified in obstructive sleep apnea (OSA) and central sleep apnea (CSA). OSA is a frequent sleep disorder characterized by repetitive interruption of ventilation caused by partial or complete collapse of the upper airway during sleep and affects an estimated 9% of adult women and 24% of adult men (Peppard et al., 2013). In contrast, in CSA the cessation of respiratory muscle activity and airflow is produced by the temporary withdrawal of central (brainstem-driven) respiratory drive.
This entity is less frequent and is usually associated with heart failure (HF) and neurological disorders, or also described in patients being administered high-dose opiates (Muza, 2015). CSA has also been reported in normal people who acutely acclimatized to high altitude during light sleep and in the presence of relative hypocapnia and alkalosis (Burgess et al., 2014).
Sleep apnea (SA) contributes to an increase in morbidity and mortality in patients with CVD (Fonseca et al., 2015). The risk of SA appears to be unrelated to traditional risk factors for CVD and may involve unrecognized variables that directly affect cardiac function and arrhythmogenesis. The pathogenesis of SA in subjects with CVD is complex and remains incompletely understood. Apneas may induce severe intermittent hypoxemia and CO2 retention with oxygen desaturation, resulting in increased autonomic activity and vasoconstriction of peripheral blood vessels. Hemodynamic stress occurs at a time of severe hypoxemia, hypercapnia, and adrenergic activation (Somers et al., 1989, 1995). These events activate mechanisms such as increased sympathetic activity, metabolic dysregulation, left atrial enlargement, endothelial dysfunction, ischemic inflammation, and hypercoagulability. The consequences of activation of these mechanisms are hypertension, HF, arrhythmias, renal disease, stroke, and myocardial infarction (Somers et al., 2008).
Sleep disturbances are also frequent in individuals who ascend to high altitudes. At high altitude, the normal cyclical breathing is lost during sleep and the number of periodic breathing cycles increased. Hypoxic exposure activates peripheral and central chemoreceptors, increasing the partial pressure of alveolar oxygen and declining partial carbon dioxide pressure (Bloch et al., 2010; Nespoulet et al., 2012). Hypobaric hypoxia stimulates central apneas in patients with OSA at high altitude, inducing sympathetic activation resulting in higher heart rate, cardiac arrhythmias, and hypertension. It has been suggested that hypoxia-inducible factor pathways play an important role in the adaptive response to chronic hypoxia observed in high altitude and the intermittent hypoxia observed in SA producing vasoactive peptides and inflammatory cytokines expressed by the carotid body. The upregulation of the local renin–angiotensin system and the inflammation in carotid body result in maladaptive response of the carotid chemoreceptor functions, contributing to the pathophysiology of SA and its cardiovascular consequences (Fung et al., 2014). However, the role of altitude in patients with SA and CVD has not been established (Bloch et al., 2015).
Based on this, we hypothesize that the prevalence of SA is higher in patients with CVD who live at high altitude. The purpose of this study was to evaluate the prevalence of SA in patients with CVD in three cities located at different altitudes in Colombia.
Methods
Study design
This is a prospective cross-sectional study of the prevalence of SA in subjects with CVD with either coronary artery disease (CAD) or atrial fibrillation (AF). Patients with both disorders were not included. The study was approved by the ethics committees of the Faculty of Medicine at the Pontificia Universidad Javeriana, Hospital Universitario San Ignacio and the Instituto del Corazón de Bucaramanga/Bogotá. Adults 40 years of age and older were recruited from the Instituto del Corazón in Bucaramanga and Bogotá and from a cardiologist private practice in Santa Marta. Bogotá is located at ∼2640 m (8861 ft) above sea level with a population around 8.8 million people. Bucaramanga is located at 950 m (3116 ft) with a population of about 1,022,341 people. The altitude of Santa Marta is 4 m (13 ft) and has ∼500,000 inhabitants. Subjects with CAD and AF were recruited in Bogotá, Bucaramanga, and Santa Marta. To include patients with CAD, we selected patients 40 years of age and older who had obstruction of at least one main coronary artery of 50% or more, diagnosed by coronary angiography. The diagnosis of AF was confirmed by 12-lead ECG.
The control group was composed of women and men 40 years of age or older with similar origin (ethnically, socially, and geographically) and socioeconomic status to the case group without history or presence of CVD. Individuals with similar origin were included in the control group if they showed a high suspicion of sleep disturbances. Informed consent was obtained from all subjects participating. All participants in control and case groups completed questionnaires on sleep habits (STOP-BANG; Epworth, Pittsburg, Berlin) and general health; body mass index (BMI) and blood pressure were measured before in-hospital overnight polysomnography. BMI was measured using a standardized protocol.
Study sample
The sample size was calculated based on population of each city and prevalence of CVD and SA in adults. Case group subjects were selected according to the already described inclusion criteria. Individuals younger than 40 years, with congenital cardiomyopathies, mental illnesses, or syndromes were excluded. Subjects older than 80 years of age were also excluded. All in-hospital patients underwent overnight polysomnography in the three cities and were distributed as follows: 235 subjects with CAD and 76 subjects with AF (60 permanent AF, 16 paroxysmal AF) from Bogotá (high altitude); 134 subjects with CAD and 75 subjects with AF (64 permanent AF, 11 paroxysmal AF) from Bucaramanga (moderate altitude); 50 CAD subjects and 30 AF subjects (19 permanent AF, 11 paroxysmal AF) from Santa Marta (sea level). A total of 300 subjects with a high probability of SA determined by the sleep questionnaires and without CVD or family history of CVDs were selected as controls and underwent overnight in-hospital polysomnography. Of the 600 subjects with CVD and 300 controls selected, 40 patients with HF, 18 with CVD, and 8 control subjects were excluded from the statistical analysis due to low sleep efficiency (patients who did not sleep for more than 3 hours during the entire night) from cities with high and moderate altitudes.
Polysomnography
All participants underwent in-hospital polysomnography using an Alice Diagnostic Sleep System (Phillips Respironics®). The following channels were recorded: electroencephalogram, electrocardiogram, electrooculogram, chin electromyogram, pulse oximetry, chest and abdominal excursion by inductance plethysmography, leg movement scoring, airflow, and body position. Polysomnograms were blindly interpreted by the same pulmonologist, according to the American academy of sleep medicine criteria. These criteria included hypopneas associated with an oxyhemoglobin desaturation of 4%.
Statistical analysis
Descriptive statistics were performed by categories of SA (sensitivity analysis according to CSA/OSA). Subjects who had mixed events with 70% or more obstructive events were classified as OSA. Similarly, subjects who had mixed events with 70% or more central events were classified as CSA, CVDs (CAD and AF), and altitude (Bogotá—high, Bucaramanga—moderate, Santa Marta—low). Multinomial logistic regression, X2, and Hosmer and Lemeshow tests were used to determine interactions among variables (CVD, CAD, AF, OSA, CSA, BMI, gender, and altitude), and a p < 0.05 was considered statistically significant for the coefficients in the multinomial logistic regression determined by the Wald X2 statistic. All statistical analyses were performed with IBM SPSS Statistics Version 22.0 software (license Pontificia Universidad Javeriana).
Results
Overall, 542 subjects with CVD and 292 controls in three cities in Colombia (Bogotá, Bucaramanga, and Santa Marta) were included. The distribution of 542 CVD subjects in each city is shown in Figure 1. A total of 78% of subjects with CVD had SA and the highest prevalence of SA was observed in patients who lived at high altitude (91%). The distribution of the types of apnea according to CVD in each city demonstrated that OSA was the most frequent type of apnea in CVD (55.6%) and control group (49.7%) in all cities, whereas CSA was more frequent in subjects with CVD (24.2%) than in the control group (7.9%). Subjects with CVD had a significant association with OSA and CSA at high altitude (OR: 5.52; 95% CI 2.9–10.7, p < 0.0001 for OSA and OR: 2.44; 95% CI 1.2–5.2, p < 0.021 for CSA, Table 1 and Fig. 2).
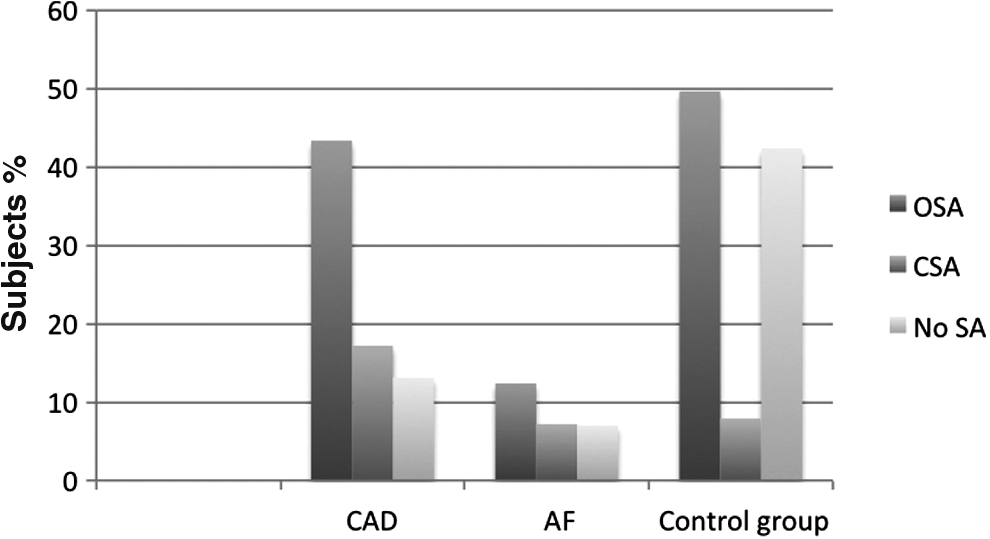
Distribution of SA in CVD and control groups. SA, sleep apnea.
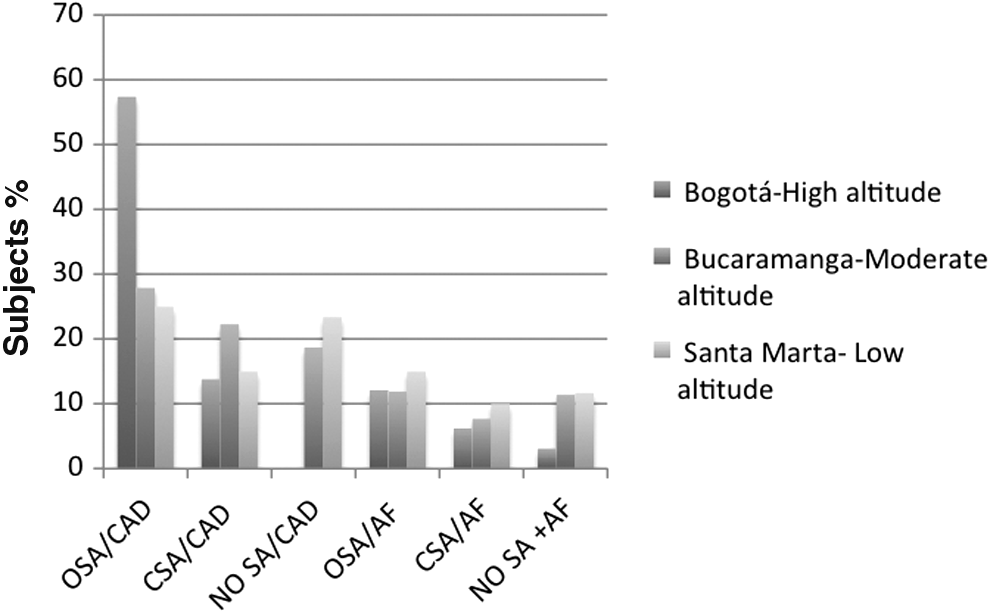
Distribution of SA in subjects with CAD and AF at different altitudes. AF, atrial fibrillation; CAD, coronary artery disease.
AF, atrial fibrillation; CAD, coronary artery disease; CI, confidence interval; CSA, central sleep apnea; CVD, cardiovascular disease; OR, odds ratio; OSA, obstructive sleep apnea; SA, sleep apnea.
Further analysis was performed by gender in the three cities. CSA was highly significant in men with AF in all cities (OR: 5.25; 95% CI 2.8–9.9, p < 0.0001). Men and women with CVD at high altitude had a higher risk than men and women living at lower altitudes for SA (OR: 6.01: 95% CI 2.4–15, p < 0.0001 for men compared with women OR: 3.02; 95% CI 1.3–7.1, p < 0.011, Table 1 and Fig. 3). SA was associated with CAD in men more frequently than in women in the three cities, but SA was higher in women than in men with AF at sea level (Fig. 3). Although the highest risk of SA was observed in men with AF (OR: 8; 95% CI 1.3–14.5 p < 0.002) and women with CAD (OR: 9.5; 95% CI 2.5–15.7 p < 0.001) living at high altitude, the risk for men with CAD living at high altitude (OR: 4.61; 95% CI 1.7–12.5 p < 0.003) and women with CAD living at moderate altitude (OR: 4.9; 95% CI 1.2–9.45 p < 0.024) was also increased.
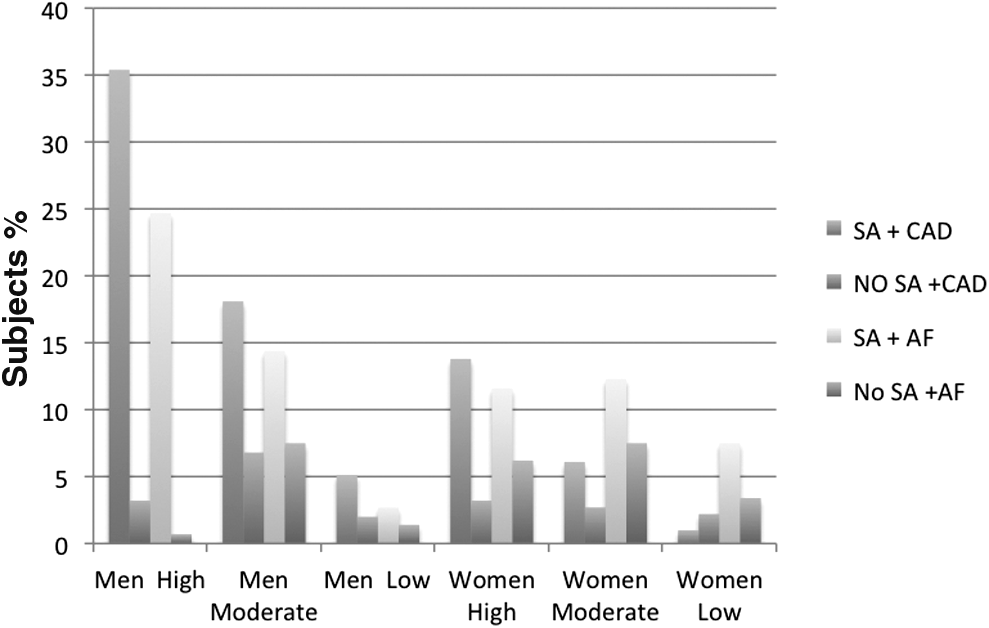
Distribution of SA in subjects with AF and CAD by gender and altitude.
BMI was calculated for all patients. The majority of subjects with CVD in the three cities were overweight (49%), normal weight in 28%, and obesity in 23%. Thirty-eight percent of the control subjects were overweight, 36% having a normal weight, and 26% being obese. This distribution was similar in both genders in each city. In high and moderate altitude, OSA was the predominant type of SA in subjects with CVD and in either obesity or overweight. In contrast, subjects with CVD and overweight at sea level did not have a significant incidence of SA. Absence of SA was more common in subjects with CVD and normal weight at low and moderate altitude but not at high altitude. Similarly, SA was rarely observed in both genders with normal weight. When subjects of the three cities were pooled by BMI and presence of CVD, OSA was the most frequent type of SA in subjects with CVD and overweight, and in subjects of the control group with overweight and obesity (Fig. 4). Obesity even in the control group was associated with OSA (OR: 10.6; 95% CI 5–16.2, p < 0.0001). Overweight individuals with CVD and in the control group also had a significant association with OSA (CVD: OR:10; 95% CI 5.5–18.5, p < 0.0001, and OR: 6; 95% CI 2.9–12.3, p < 0.0001, respectively).

Distribution of SA in CVD by BMI and altitude. BMI, body mass index; CVD, cardiovascular disease.
Discussion
This study showed an overall increased prevalence of sleep-disordered breathing in a cohort of both matched controls and individuals with CVD in three urban areas from a middle-income country in South America. The main finding was the documentation of a significant association between CVD and SA at high altitude, observed in 91% of the subjects living 8000 ft. above the sea level. Similarly a sixfold increase in risk of SA was primarily observed in male obese or overweight subjects with documented CVD living at high altitude compared with individuals living below 3000 ft.
Although acute hypoxia observed in climbers at high altitude has been well studied (Tseng et al., 2015; Guan et al., 2015), the effect of chronic hypoxia observed in sleep disturbances remains unclear and the effect of altitude in patients with CVD and SA has not been fully studied. Hypoxic pulmonary vasoconstriction increases the pressure in pulmonary artery with atrial and ventricular ectopic activity that is observed as morphological changes in the electrocardiogram. These events may produce ischemia and sudden cardiac death in patients with cardiac disease who ascend to high altitude (Windsor et al., 2010; Levine, 2015). Likewise, other acclimatization effects (Vearrier and Greenberg, 2011) and cardiovascular events in mountain activities (Lo et al., 2013) have been well documented. However, the outcomes of interaction between chronic constant hypoxia observed at high altitude and chronic intermittent hypoxia present in SA in subjects with CAD and AF have not been sufficiently investigated. Therefore, it is important to elucidate the role of hypoxia in patients with CVD and SA at high altitude.
High altitude determines more hypopnea and apnea due to the fact that at high altitude the normal cyclic breathing pattern is lost, thereby causing arousals (Windsor and Rodway, 2012). Oxygen saturation drops to 60%, during sleep at high altitude, disrupting the autonomic and hemodynamic responses to sleep (Burgess et al., 2006).
To investigate possible differences in the association between CVD and SA due to gender and obesity, we analyzed these variables in relation to altitude. We observed that men with CAD living at high altitude had an almost fivefold increase in risk of SA, in contrast, women with CAD living at high and moderate altitudes had a 5 to 10-fold increase in risk of SA.
We observed differences in the frequency of SA and AF in women compared with that in men. Women with AF had a significantly higher rate of SA (CSA and OSA) in the three cities than the control group. In contrast, men with AF, living at high altitude, had an eightfold increase in SA. Lombardi et al. (2013) studied the effect of altitude in healthy subjects and showed a lower CSA prevalence in women than in men at high altitude exclusively during acute exposure. It is unclear why our findings are not concordant with Lombardi et al's., this may be related to the effects of chronic exposure to high altitude. Popovic and White (1998) suggested that female hormones act on the upper airway dilator muscle, protecting females to have OSA. We have previously reported that the prevalence of OSA is increased in postmenopausal women with and without CVD, but the prevalence of CSA did not change with the age (Krishnan and Collop, 2006). The mechanisms involved in the development of CSA at high altitude in healthy subjects remain unclear.
Being overweight was frequent in the three cities. However, at low and moderate altitudes, subjects with CVD rarely had SA, whereas at high altitude, OSA was more common in overweight subjects with CVD (20.5%). Being overweight carried a 10-fold risk of OSA in subjects with CVD and a 6-fold increase in risk of OSA in the control groups. Interestingly, obesity was only significantly associated in individuals belonging to the control group. These findings suggest that in subjects with CVD, other mechanisms additional to airway obstruction may be related to the development of SA.
Although the CVD group showed a high prevalence of OSA and CSA, the higher prevalence of CSA in patients with CVD compared with controls seems to be more related to the presence of CVD and altitude than BMI. Men with AF represented the group of the highest risk for CSA. Muscle sympathetic nerve activity and blood pressure increase due to acute hypoxia at high altitude and in OSA (Dempsey et al., 2014). However, the effects of intermittent hypoxemia on the cardiovascular system and in patients with CVD remain to be determined. OSA has been associated with CAD and AF (Xie et al., 2014). In contrast, CSA occurs in 30%–50% of patients with HF (Costanzo et al., 2015). The presence of CSA in CVD patients can be potentially explained by conversion of obstructive events to predominantly central events possibly related to hypoxemia and hypercapnia at high altitude.
The mechanisms that determine the development of CSA at high altitude include dysregulation of CO2 homeostasis and subsequent hypocapnia (Wellman et al., 2004). Hypoxemia, respiratory alkalosis, and chronic hypocapnia observed in individuals exposed to high altitude might result in instability of the ventilation system during sleep (Day and Wilson, 2008). Although central respiratory output contributes to narrowing of the upper airway during sleeping state, interaction between decreased activation of upper airway musculature, hypocapnia, and ventilator responsiveness in OSA is unclear (Dempsey, 2005). Moreover, it remains uncertain whether the mechanisms determining the conversion of OSA to CSA at high altitude are related to an interaction between narrowing of the upper airway, hypocapnia, and ventilator responsiveness or whether high altitude simulates the pathophysiology of CSA in HF (Pagel et al., 2011). Burgess et al. (2004) assessed the occurrence of CSA in 13 subjects during acclimatization to high altitude and the interaction between ventilatory responsiveness, hypoxic stimulus, and hypercapnic drive at high altitude. In contrast, in our study the prevalence of CSA increased in patients with CVD at high altitude but not in the control group at high altitude, suggesting that chronic adaptation to altitude may play a role.
An important limitation in our study was that we did not adjust for other comorbidities commonly associated with both SA and CVD (hypertension, diabetes, metabolic, and renal disease). In addition, difference in mean age between the subjects at different altitudes, genetic, and ethnic factors should be considered before applying these findings more broadly.
Conclusion
In this prospective cohort study that assessed the frequency of sleep-disordered breathing in subjects with CVD (CAD, AF) and matched controls at different altitudes in three urban cities within Colombia, significant differences in the frequency of SA associated with altitude, gender, and type of CVD were observed.
Footnotes
Acknowledgment
This work was funded by COLCIENCIAS through Grant 369 Project 501953731808.
Author Disclosure Statement
No competing financial interests exist.