
Abstract
Abstract
Dobashi, Shohei, Masahiro Horiuchi, Junko Endo, Masataka Kiuchi, and Katsuhiro Koyama. Cognitive function and cerebral oxygenation during prolonged exercise under hypoxia in healthy young males. High Alt Med Biol. 17:214–221, 2016.—The present study examined the effect of prolonged hypoxic exercise on cognitive function. Eight healthy male volunteers were required to complete exercise trials (four 30-minute cycling sessions with a 15-minute rest interval) at an intensity corresponding to 50% of their altitude-adjusted peak oxygen uptake under two different conditions: normoxia (room air at 400 m) and hypoxia (fraction of inspired oxygen: 0.141). Cognitive function was evaluated before, during, and 60 minutes after completion of the exercise trial. The color-word Stroop task (CWST) was used to assess cognitive function, with regard to the number of achievements, accuracy rate, and the number of correct responses made within 60 seconds. Cerebral oxygenation was monitored throughout the experimental period using near-infrared spectroscopy. The accuracy rate did not significantly differ between the two trials. A significant reduction in the number of correct responses during simple CWST tasks was detected in the hypoxic condition 60 minutes after exercise (p < 0.05), wherein a significant correlation was identified between reduced task performance on simple CWST and cerebral oxygenation (p < 0.01). These results demonstrate that prolonged exercise under hypoxic conditions induces a reduction in cerebral oxygenation partly associated with impairment of cognitive function.
Introduction
I
Oxygen availability is typically compromised in hypoxic environments, particularly at high altitude. Exposure to hypoxic conditions induces oxygen desaturation (de Aquino Lemos et al., 2012) and a decline in cerebral oxygenation, as assessed by near-infrared spectroscopy (NIRS) (Subudhi et al., 2009; Vogiatzis et al., 2011; Wilson et al., 2011). Recent studies have indicated that hypoxia impairs neural function, affecting cognitive processes, such as selective attention, response inhibition, and interference control (Hornbein, 2001; Virués-Ortega et al., 2004, 2006; Wilson et al., 2009; Yan, 2014). Accordingly, the effects of hypoxia on cognitive function might be determined with regard to the balance between the beneficial effects of acute exercise, and the detrimental effects of hypoxic exposure (Komiyama et al., 2015).
Previous studies concerning the influence of hypoxia on cognitive function during exercise are limited. Ando et al. (2013) investigated the effects of short-term exercise (∼10 minutes) on response time and task accuracy under moderate hypoxia [fraction of inspired oxygen (FiO2) = 0.15] using the Go/No-Go (GNG) task. Following task completion, GNG reaction time was reduced under both normoxic (FiO2 = 0.209) and hypoxic conditions, but no significant difference in reaction time was detected between the two. Moreover, Komiyama et al. (2015) examined the influence of moderate hypoxia (FiO2 = 0.15) on working memory and executive function during a 30-minute cycling exercise using a combination of the spatial delayed response and GNG tasks. No significant differences were detected with regard to accuracy or reaction time between the normoxic and moderately hypoxic conditions. Such results indicate that moderate hypoxia did not significantly influence working memory and executive function during a 30-minute exercise period (Ando et al., 2013; Komiyama et al., 2015). This suggests that the beneficial effects of exercise appear to persist even under moderate hypoxia, despite a reduction in cerebral oxygenation (Ando et al., 2013; Komiyama et al., 2015). However, previous studies have only considered the effects of short-term hypoxia on cognitive function. Accordingly, cerebral oxygenation was found to increase between the baseline and 2.5 km time points during a 5 km running trial, but decrease between 4.5 and 5 km (Billaut et al., 2010), indicating that prolonged exercise induced a relative decrease in cerebral oxygenation. In addition, Imray et al. (1998) found a negative correlation between the degree of acute mountain sickness (AMS) and cerebral oxygenation. Furthermore, incidence and severity of AMS were accelerated after prolonged hypoxic exercise (Roach et al., 2000). Given these results, prolonged hypoxic exercise may have enough stimulus to exacerbate the AMS that might impair cognitive performance, possibly, due to a reduction in cerebral oxygenation. Since the number of individuals pursuing high altitude sports, or engaging in hypoxic training has increased in recent years (Honigman et al., 1993; Levine and Stray-Gundersen, 1997), investigation of the cognitive and physiological effects of hypoxia during prolonged physical activity is important from a practical perspective, for example, prevention of AMS, and/or falling accidents.
With regard to the influence of hypoxia, the present study aimed to investigate whether prolonged exercise under hypoxic conditions might impair cognitive function. We hypothesized that prolonged exercise within a hypoxic environment might exacerbate cognitive impairment, potentially as a function of reduced cerebral oxygenation. To test this hypothesis, prolonged hypoxic exercise trials were performed based on a previous study, to simulate the level of physical activity that typically accompanies ascent to high altitude, which has been shown to exacerbate the symptoms of AMS (Roach et al., 2000).
Materials and Methods
Participants
Nine healthy males with a mean age of 23.7 ± 2.1 years (mean ± SD), who were able to perform high-intensity cycling were recruited for the present study through an advertisement at the University of Yamanashi. None of the participants had any history of cardiovascular, cerebrovascular, or respiratory disease. Participants had not smoked, taken medication, or performed exercise training in the 6 months before the study. Each participant was informed of the purpose, experimental procedures, and the possible risks involved in the present study. Written informed consent was provided before the start of experimentation. All subjects were asked to refrain from intensive physical activity 2 days before the study, and to avoid drinking any alcohol and caffeinated beverages for 24 hours beforehand. Data obtained from eight participants (age: 23.5 ± 2.2 years, height: 173.0 ± 8.1 cm, body weight: 74.1 ± 19.0 kg, mean ± standard deviation) was used for further analysis, as one participant was unable to complete the experimental procedure under hypoxia due to an intense headache thought to be associated with AMS. All experimental procedures were approved by the Human Research Ethics Committee of the University of Yamanashi in Japan, and performed in accordance with the guidelines of the Declaration of Helsinki.
Aerobic capacity tests
First, to determine both peak oxygen uptake (peak VO2) and workload during prolonged exercise trials, each participant was required to complete two incremental cycling exercise tests under normoxic (room air, at 400 m above sea level) and normobaric hypoxic conditions (FiO2 = 14.1%, corresponding to 3200 m). The tests were performed using a cycle ergometer (828E; Monark, Stockholm, Sweden) in an upright position until the participant was exhausted. Exercise trials were performed at least 2 days apart, in a random order. A hypoxic control system (YHS-B05S; YKS, Nara, Japan), and an air compressor (0.75LP-7SO; Hitachi, Chiba, Japan) were used to maintain hypoxic conditions during the trials. Respiratory gases were collected using a breath-by-breath method with an automatic gas analyzer (AE-300S; Minato Medical Science Co., Ltd., Osaka, Japan). The participants breathed through a facemask attached to a low-resistance one-way valve with a flow meter. The valve mechanism allowed participants to inspire either room air (normoxic condition) or a predetermined gas mixture from a 2000-L custom-made cuboid chamber (1 × 1 × 2 m) containing 14.1% O2, in 0.05% CO2 with an N2 balance (hypoxic condition). The criteria for exhaustion were as follows: (1) No increase in VO2 despite a further increase in work rate; (2) Heart rate (HR) at 90% of the age-predicted maximal value (220-participant's age) (Howley et al., 1995); (3) A rating of 19 on the Borg's scale of perceived exertion (Borg, 1982); or (4) Failure to maintain pedaling frequency of 60 rpm despite strong verbal encouragement. When participants met at least two of the above criteria, the aerobic capacity test was terminated.
Prolonged exercise trials
At least 1 week after the aerobic capacity test, participants completed the two experimental trials. After a 15-minute rest period on the bicycle ergometer, subjects participated in a prolonged exercise session consisting of four 30-minute cycling sets (at 50% of the participant's altitude-adjusted peak VO2) with a 15-minute interval between each set under both normoxic (room air) and normobaric hypoxic (FiO2 = 14.1%) conditions. This was followed by a 1-hour recovery period. At each interval and during the recovery period, participants left the cycle ergometer and sat in a chair. Cognitive function was assessed before (Pre), immediately after the second (Ex 2) and fourth sets (Ex 4), and 60 minutes after the exercise trial (Post 1 hour), at a desk in an upright seated position (Fig. 1). Each trial was conducted over different days with an interval of more than 2 weeks between them. The order of hypoxic and normoxic trials was counterbalanced across the participants. In the present study, the protocol exacerbating AMS proposed by Roach et al. (2000) was modified to simulate physical activity in the severe condition that may impair cognitive function (Virués-Ortega et al., 2004).

Illustration of the experimental protocol. FiO2, fraction of inspired oxygen; SpO2, arterial saturation.
Physiological measurements
Arterial saturation (SpO2) and HR were measured using a pulse oximeter (PULSOX-3; Minolta, Tokyo, Japan) placed on the left index finger and a wireless HR monitor (RS800CX; Polar Electro Oy, Kempele, Finland), respectively. SpO2 and HR were monitored continuously throughout the exercise trial, and recorded every 5 minutes.
Cerebral oxygenation was evaluated using a NIRS system (BOM-L1TRW; Omegawave, Tokyo, Japan), as previously described (Ando et al., 2010, 2013; Horiuchi et al., 2014; Komiyama et al., 2015). This instrument used three laser diodes (at 780, 810, and 830 nm) to calculate the relative tissue levels of oxygenated hemoglobin (HbO2) and deoxygenated hemoglobin (HHb) according to the modified Beer-Lambert Law (Kashima, 2003). Total Hb was defined as the sum of HbO2 and HHb. Cerebral oxygenation was calculated by dividing HbO2 by total Hb × 100, and represented as a percentage. Optodes were placed over the participant's left frontal lobe, and a black cloth was wrapped around the probe holder to shield it from ambient light. The participant's entire head was wrapped in an elastic bandage. The probe holder contained one light source probe, and two detectors were placed 2 cm (detector 1) and 4 cm (detector 2) away from the source. This procedure minimized the influence of skin blood flow on data collection (Ando et al., 2010, 2013; Horiuchi et al., 2014). After the initial stage of cognitive assessment (Pre), baseline cerebral oxygenation was measured for 5 minutes during the 15-minute resting period. Analog outputs were digitized at a sampling rate of 1 Hz using a field data recorder (es8; TEAC, Tokyo, Japan). Landmarks on the forehead, including the nasion, eyebrow, and hairline, were used to ensure that the probe holder was set at the same position on both experimental days (Ando et al., 2010; Komiyama et al., 2015). This allowed cerebral oxygenation to be compared across different days.
Cognitive task
Hakoda and Sasaki's version of the color-word Stroop task (CWST) (New Stroop test II; Toyo Physical, Fukuoka, Japan) was used to evaluate cognitive function in the present study (Hakoda and Sasaki, 1990; Takeuchi et al., 2012; Fig. 2). The CWST presented five color-word associations (Red, Blue, Yellow, Green, and Black) in Japanese notation, with color patches corresponding to the words. For this test, participants were required to select appropriate answers from five options, which took the form of either color or word panels. The CWST was composed of the following four tasks. In Task 1 (reverse-Stroop control task), the name of a color was presented in the leftmost column. Adjacent to this, five columns were printed with five different colors, and participants were required to check the column with a color corresponding to the word in the leftmost column. For Task 2 (reverse-Stroop interference task), participants were required to check the color column corresponding to a word in the leftmost column, which was printed in another color (e.g., “Red” was printed in “Blue”). In Task 3 (Stroop control task), participants were required to select a color name from one of five columns, which corresponded to a color in the leftmost column. For Task 4 (Stroop interference task), a color name was printed in a different color in the leftmost column, whereas the five other columns contained color names. Each task sheet contained 100 tests. Participants were instructed to perform the tasks as fast and accurately as possible in 60 seconds. Each task was preceded by a practice task consisting of a maximum of 10 problems to be completed in 10 seconds. The four tasks were performed in a fixed order, but the order of the tasks did not affect performance (Hakoda and Sasaki, 1990). In addition, these four tasks featured a high-retest reliability (r = 0.695–0.824) (Hakoda and Sasaki, 1990). In the present study, participants completed the CWST at the Pre, Ex 2, Ex 4, and Post 1 hour stages, respectively (Fig. 1). To minimize the practice effect, participants visited the laboratory before experimentation, and performed practice sessions to familiarize themselves with the testing style.
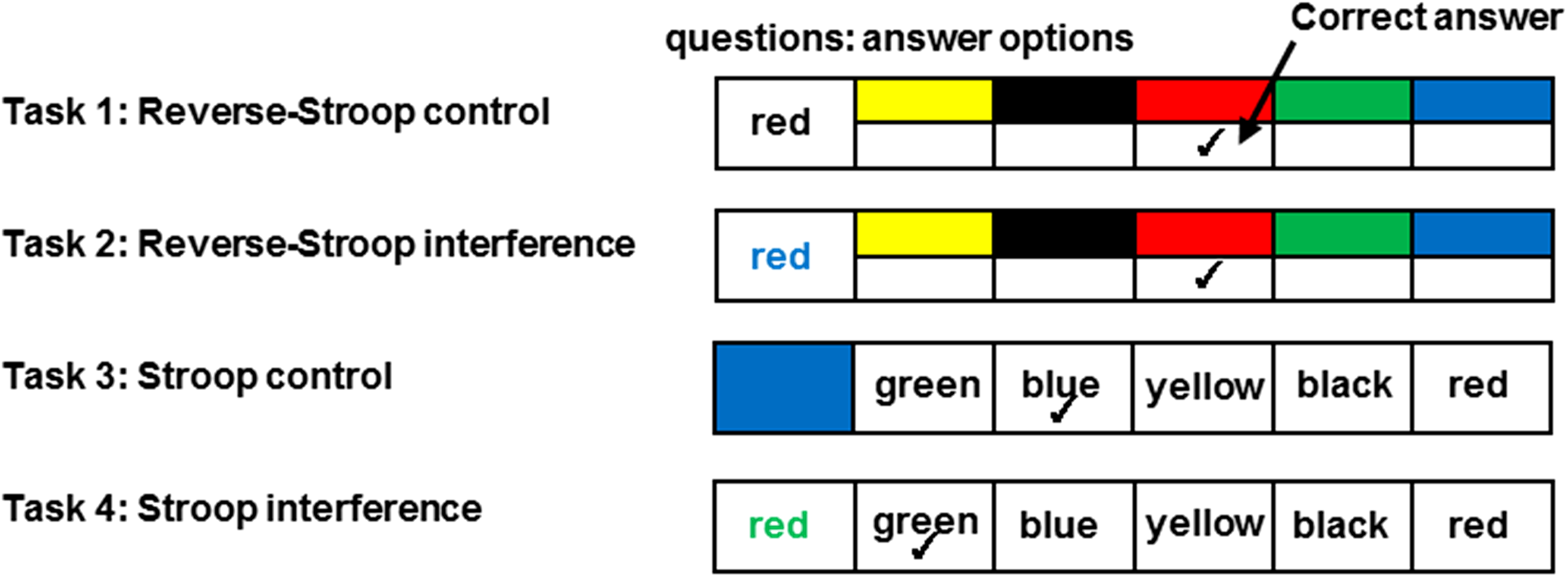
Schema of cognitive tasks used in this study (modified from Hakoda and Sasaki [1990]). The task consists of two control tasks (Task 1 and Task 3), and two interference tasks (Task 2 and Task 4).
Data analysis
Cerebral oxygenation values recorded during cognitive assessment were expressed relative to the baseline value obtained during the normoxic trial. Changes in the number of correct responses were expressed as a function of changes at each time point (Pre, Ex 2, Ex 4, and Post 1 hour, respectively).
Pearson's correlation coefficient was used to examine the relationship between the changing number of correct CWST responses relative to the Pre value baseline, and cerebral oxygenation when data were partly pooled. Briefly, in this study, four tasks of the CWST were evaluated at three points (Ex 2, Ex 4, and Post 1 hour) in two conditions (normoxia and hypoxia) for eight participants, thus the total number of plotted data would be 192 (4 tasks × 3 time points × 2 conditions × 8 participants). However, we separated by control (Task 1, 3) and interference (Task 2, 4) tasks, because it has been suggested that cerebral oxygen consumption might be different by the task difficulties (Verner et al., 2013). Data analysis was performed to investigate the effects of changes in cerebral oxygenation on cognitive function, based on a previous study (Yanagisawa et al., 2010; Endo et al., 2013; Byun et al., 2014).
Statistics
All physiological data were expressed as mean ± standard error of the mean (SE). With regard to comparisons of SpO2, cerebral oxygenation, and CWST score, a two-way (condition × time) ANOVA with repeated measures was used to assess interactions between condition and time, with condition and time as the main effects. If the F value was significant, a Bonferroni test was performed for post hoc analysis to elucidate the differences. A Pearson's correlation coefficient test was performed to analyze the relationship between changes in the number of correct CWST responses and cerebral oxygenation over the same period. All statistical analyses were performed using R ver. 3. 0. 2 (R Core Team, 2014). For all statistical tests, p < 0.05 was considered significant.
Results
Physiological measurements
Figure 3A displays SpO2 values under normoxic and hypoxic conditions. No significant interactions were detected with regard to condition and time [F (2, 14) = 0.40, p > 0.05, η2 = 0.05]. A significant main effect was observed for condition [F (1, 7) = 189.08, p < 0.001, η2 = 0.96] on SpO2; however, time was not significant [F (2, 14) = 1.02, p > 0.05, η2 = 0.13].
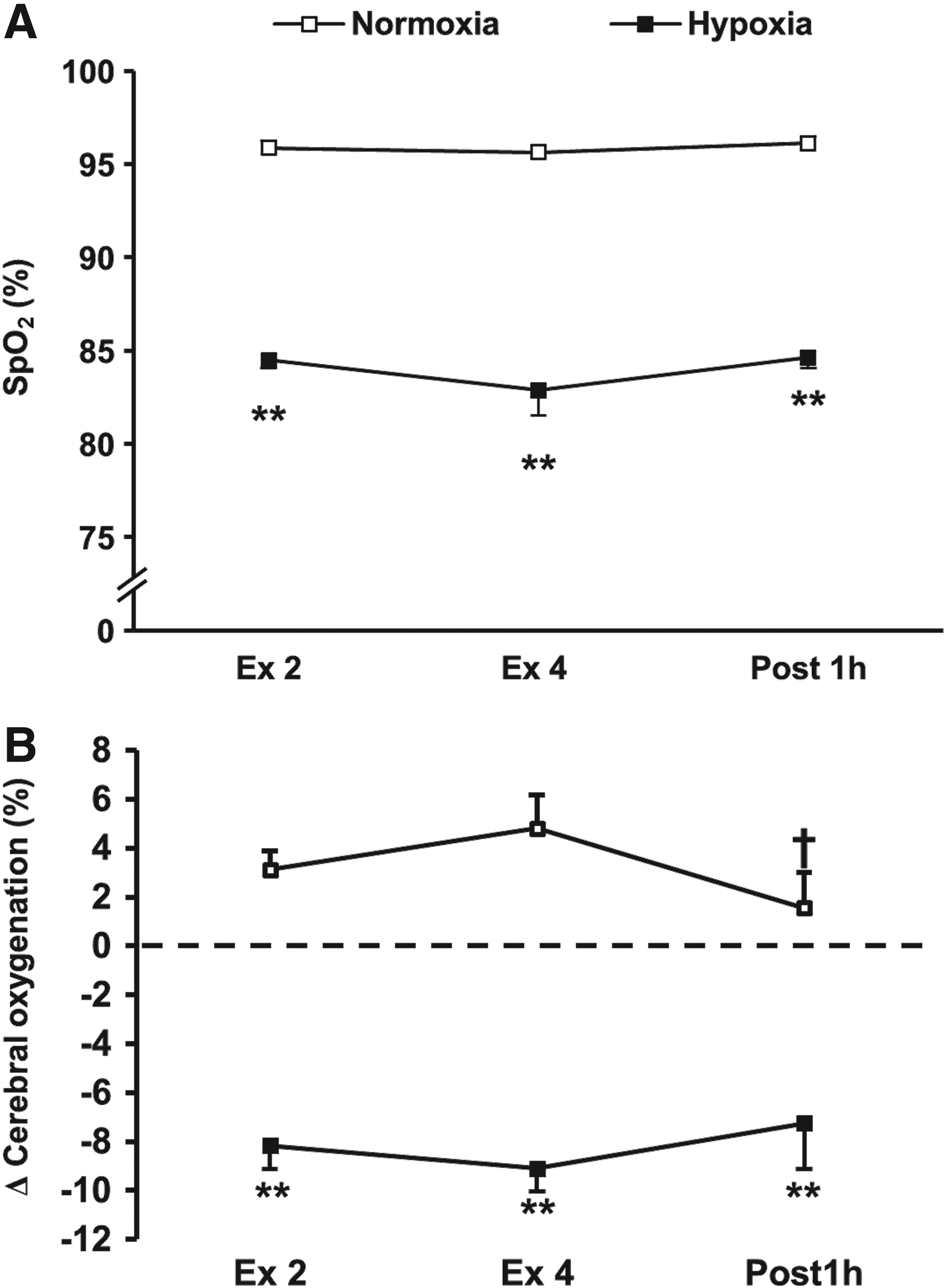
Time course of changes in SpO2
Relative to the normoxic condition, SpO2 values were significantly lower during the hypoxic condition at the Ex 2, Ex 4, and Post 1 hour stages (p < 0.01, respectively, Fig. 3A). Cerebral oxygenation values were expressed relative to changes from the baseline obtained for both trials (Fig. 3B). A significant interaction was detected with regard to the effects of both condition and time on cerebral oxygenation [F (2, 14) = 4.96, p < 0.05, η2 = 0.41]. The reduction in cerebral oxygenation was significantly greater under hypoxic conditions compared with normoxic conditions at the Ex 2, Ex 4, and Post 1 hour time points (p < 0.01, respectively, Fig. 3B).
Cognitive function
Table 1 displays the number of achievements and accuracy rate for each task of the CWST. In Task 1, a significant interaction was detected between condition and time with regard to the number of achievements [F (3, 21) = 4.53, p < 0.05, η2 = 0.39]. In Task 3, no significant interaction was identified between condition and time for the number of achievements [F (3, 21) = 2.97, p > 0.05, η2 = 0.30], however, a significant main effect for time was detected [F (3, 14) = 4.09, p < 0.05, η2 = 0.37] without condition [F (3, 21) = 0.24, p > 0.05, η2 = 0.03]. The number of achievements within control tasks was significantly lower (Task 1 and 3) at the Post 1 hour stage under hypoxic conditions compared with normoxic conditions (p < 0.05, respectively). During the interference tasks (Task 2 and 4), no significant interactions were detected between condition and time (p > 0.05, respectively). With regard to CWST accuracy, no significant interactions were detected between condition and time, and no main effects were identified (p > 0.05, respectively).
Pre refers to the before exercise trial. Ex 2 and Ex 4 are immediately after second and fourth sets of exercise, respectively. Post 1 hour is 60 minutes after exercise trial.
p < 0.05 versus Pre within the same condition and task. †p < 0.05 versus normoxia within the same task.
CWST, color-word Stroop task.
Figure 4 illustrates the changing number of correct responses at the Ex 2, Ex 4, and Post 1 hour stages compared with the CWST Pre-value baseline (before the exercise trial). A significant interaction was detected between condition and time in Task 1 [F (2, 14) = 5.63, p < 0.05, η2 = 0.45].

Changes in the number of correct responses in CWST (Y axis) immediately after the second and fourth exercise sets (Ex 2, Ex 4), and 60 minutes after exercise trial (Post 1 hour) from those at Pre (before exercise trial).
In Task 3, no significant interactions were detected between condition and time [F (2, 14) = 1.77, p > 0.05, η2 = 0.20]. A significant main effect was identified with regard to condition for the number of correct responses [F (1, 8) = 9.10, p < 0.05, η2 = 0.57], whereas time failed to reach statistical significance [F (2, 14) = 3.20, p > 0.05, η2 = 0.31]. A significant reduction in the number of correct responses was detected for the control tasks (Task 1 and 3) at the Post 1 hour stage under hypoxic compared with normoxic conditions (p < 0.05, respectively, Fig. 4A, C). Comparatively, no significant interactions or main effects were identified with regard to condition or time during interference tasks (Task 2 and 4) (p > 0.05, respectively, Fig. 4B, D).
A significant correlation was identified between the changing number of correct CWST responses relative to the Pre-value baseline and cerebral oxygenation in control (r = 0.350, n = 96, p < 0.01, Fig. 5A), but not in interference tasks (r = 0.081, n = 96, p = 0.428, Fig. 5B).
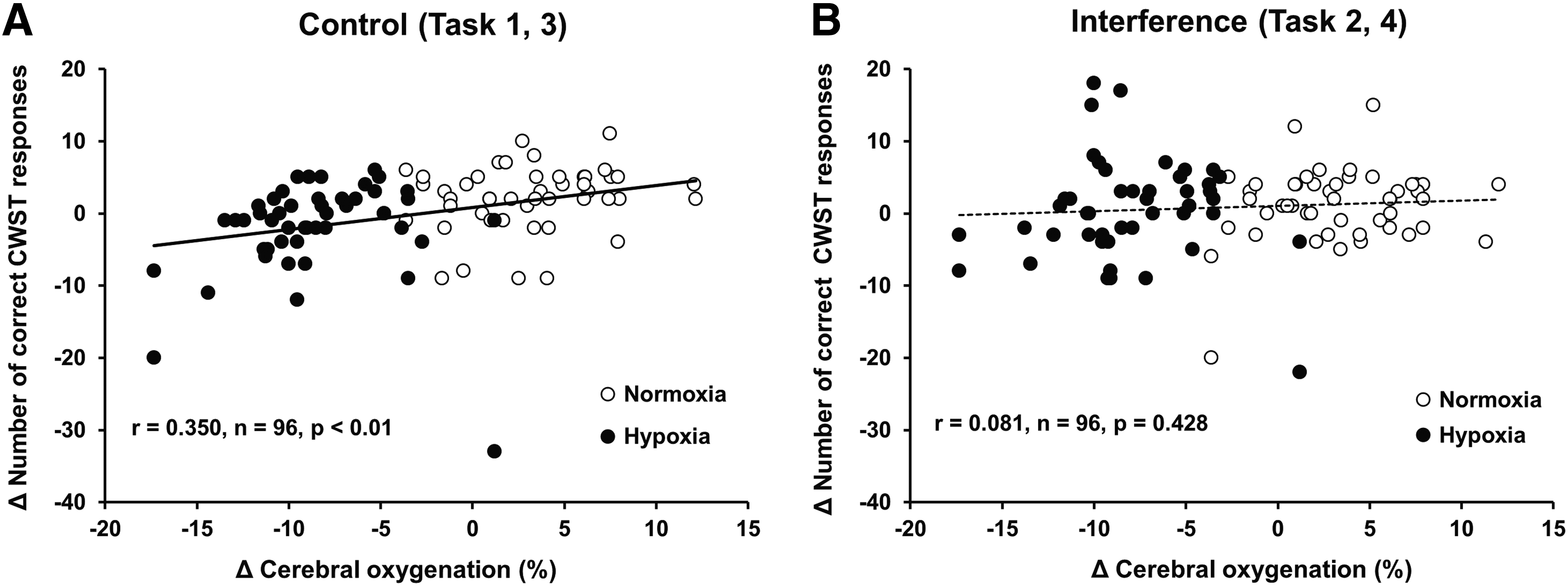
The relationship between Δ number of correct responses in CWST and Δ cerebral oxygenation from those at Pre (before exercise trial).
Discussion
To the best of the authors' knowledge, this is the first study to examine the effects of prolonged hypoxic exercise on cognitive function. The main finding of this study was that the number of correct CWST responses was significantly reduced by prolonged exercise in control tasks (Task 1 and 3) in the hypoxic condition. Moreover, we also found that the changes in cerebral oxygenation were associated with task performance on CWST control (Task 1 and 3), but not with interference (Task 2 and 4) tasks.
In the present study, participants were instructed to perform the test trials as fast and accurately as possible within the allotted time. Accordingly, while CWST accuracy did not differ between the normoxic and hypoxic conditions, the number of achievements in control tasks (Task 1 and 3) significantly decreased in the hypoxic condition (Table 1). Moreover, a significant reduction in the number of correct responses was detected during the control tasks (Task 1 and 3) at the Post 1 hour stage under hypoxic, but not normoxic conditions (Fig. 4A, C). However, no significant differences were detected during complex interference tasks (Task 2 and 4) for both conditions (Fig. 4B, D). The present results are consistent with previous studies, in that Stroop reaction time was decreased in hypoxic compared with normoxic conditions (de Aquino Lemos et al., 2012), whereas task accuracy was unaffected by hypoxic exercise (Ando et al., 2013; Komiyama et al., 2015). Therefore, the delay in response time identified during cognitive assessment might reflect a compensatory effect to maintain task performance and/or accuracy under hypoxic conditions. Taken together, further studies will be required to examine the relationship between response time and task accuracy in more detail.
A significant correlation was identified between the changing number of correct CWST responses and cerebral oxygenation in only control tasks (Fig. 5A). Recent studies have suggested that an increase in response time was closely linked to a progressive reduction in cerebral oxygenation during exercise (Ando et al., 2010; Mekkari et al., 2015). Cerebral oxygenation, which refers to the ratio of HbO2 to total-Hb, denotes the balance between oxygen availability and utilization (Boushel et al., 2001). Ando et al. (2010) suggested that the increase in reaction time, which was accompanied by a corresponding decrease in cerebral oxygenation, was a functional consequence of insufficient oxygen availability, resulting in an inability to meet metabolic demand in regions of the brain associated with responding to peripheral visual stimuli. While the reduction in cognitive performance observed in previous studies (Ando et al., 2010; Mekari et al., 2015) differed from the current, the impaired cognitive function detected during CWST testing might relate to decreased oxygen availability in the prefrontal cortex.
However, a question remains with regard to why prolonged hypoxic exercise impairs task performance on CWST control, but not interference tasks, accompanied with the reduction in cerebral oxygenation. One potential explanation might relate to the variable role of the dorsolateral prefrontal cortex (DLPFC) in cognitive and executive control (MacDonald et al., 2000). A previous study examined the activation of distinct neural regions in the human brain during a task-switching version of the Stroop task, using event-related functional magnetic resonance imaging (MacDonald et al., 2000). In this context, the DLPFC demonstrated a stronger degree of activation in response to the performance of simple tasks. Since functional brain activity is heavily linked to cerebral blood flow and oxygenation (Villringer and Dirnagl, 1995), the reduction in simple cognitive performance observed in the present study might relate to impaired DLPFC activity under hypoxic conditions. However, these explanations are highly speculative, as neural activity was not assessed in the present study.
The findings of this study differed from those previous, which found no evidence of cognitive impairment under normobaric hypoxia, despite a significant decline in cerebral oxygenation during exercise (Ando et al., 2013; Komiyama et al., 2015). Compared with the present study, previous experiments assessed cognitive function during exercise, rather than in the resting state. In addition, it was reported that CWST response time differed significantly with regard to between, during, and after physical exercise in depressed elderly subjects (Vasques et al., 2011). Furthermore, exercise-induced changes in neural activity appear to normalize within a few minutes (Dietrich and Sparling, 2004). Therefore, the beneficial effects of exercise on cognitive function (Ando et al., 2013; Komiyama et al., 2015) might disappear immediately after exercise, and subsequently, a reduction in cognitive performance due to hypoxic exposure might be reversed in a similar fashion. Furthermore, the type of cognitive task utilized is an important factor underlying the influence of hypoxic exercise on cognitive performance (Lamborne and Tomporowski, 2010). Previous studies utilized the GNG task to evaluate cognitive function (Ando et al., 2013; Komiyama et al., 2015), whereas the present study adopted a matching-type CWST. Moreover, the differential timing of cognitive assessment and the style of task used might underlie such discrepancies. In future studies, researchers should consider using a greater range of methods to assess cognitive function both during and after exercise in the hypoxic condition.
Another influencing factor might relate to a reduction in brain glucose metabolism, resulting in the impairment of cognitive function. Hypoxia also influences the levels of brain glycogen, an important energy source for neural activity; therefore, a reduction in cerebral oxygenation might also reduce the availability of neural glycogen and subsequently glucose (Vannucci et al., 1998). Executive functions, which use glycogen as a fuel, are typically impaired under low glycogen conditions (Gailliot, 2008). Moreover, prolonged exercise decreases the availability of brain glycogen in rodent models (Matsui et al., 2011). Taken together, prolonged exercise under hypoxic conditions might decrease both cerebral oxygenation and brain glycogen levels, producing the decline in cognitive function identified in the present study. However, cerebral oxygenation was only assessed using NIRS during the experimental trial; therefore, further studies will be required to elucidate the relationship between impaired cognitive function and neural activity under prolonged hypoxic exercise.
Methodological considerations
Several limitations should be considered to interpret our results. First, participants completed four sets of 30-minute cycling, at the intensity corresponding to 50% of the participant's altitude-adjusted peak VO2 in the present study. Peak VO2 under normoxia was significantly higher than hypoxia (46.8 ± 3.7 mL/kg/min vs. 36.5 ± 2.2 mL/kg/min, mean ± SE, p < 0.01, dz = 1.4), indicating that absolute exercise intensity of 50% peak VO2 was greater during prolonged exercise trial in normoxia than hypoxia. Therefore, it is necessary to consider the exercise intensity as an influencing factor on the results, in addition to the experimental condition (normoxia or hypoxia). Second, it should be noted that the practice effect produced by repeated CWST assessments might affect cognitive performance. Indeed, the number of correct responses for each task of the CWST was found to increase with repeated implementation (Hakoda and Sasaki, 1990). However, participants were provided with practice sessions to familiarize themselves with the CWST before participating in prolonged exercise trials, and no significant increase was identified in the number of correct responses with regard to repetition in either the normoxic or hypoxic condition (Fig. 4). Therefore, the changes in cognitive performance detected in the present study might be influenced by environmental condition (normoxia vs. hypoxia), but not by the practice effect. Finally, sample size (n = 8) in the present study was relatively small. Although our results clearly demonstrated significant differences in the number of correct CWST responses in control tasks, future studies are required with a larger population.
Conclusion
In summary, the present findings demonstrate that prolonged hypoxic exercise reduces cerebral oxygenation and impairs cognitive performance on simple CWST tasks. Moreover, the observed changes in cognitive performance were correlated with cerebral oxygenation levels.
Footnotes
Author Disclosure Statement
No competing financial interests exist.