
Abstract
Abstract
Healy, Katherine, Alain B. Labrique, J. Jaime Miranda, Robert H. Gilman, David Danz, Victor G. Davila-Roman, Luis Huicho, Fabiola León-Velarde, and William Checkley. Dark adaptation at high altitude: an unexpected pupillary response to chronic hypoxia in Andean highlanders. High Alt Med Biol. 17:208—213, 2016.—Chronic mountain sickness is a maladaptive response to high altitude (>2500 m above sea level) and is characterized by excessive erythrocytosis and hypoxemia resulting from long-term hypobaric hypoxia. There is no known early predictor of chronic mountain sickness and the diagnosis is based on the presence of excessive erythrocytosis and clinical features. Impaired dark adaptation, or an inability to visually adjust from high- to low-light settings, occurs in response to mild hypoxia and may serve as an early predictor of hypoxemia and chronic mountain sickness. We aimed to evaluate the association between pupillary response assessed by dark adaptometry and daytime hypoxemia in resident Andean highlanders aged ≥35 years living in Puno, Peru. Oxyhemoglobin saturation (SpO2) was recorded using a handheld pulse oximeter. Dark adaptation was quantitatively assessed as the magnitude of pupillary contraction to light stimuli of varying intensities (−2.9 to 0.1 log-cd/m2) using a portable dark adaptometer. Individual- and stimulus-specific multilevel analyses were conducted using mixed-effect models to elicit the relationship between SpO2 and pupillary responsiveness. Among 93 participants, mean age was 54.9 ± 11.0 years, 48% were male, 44% were night blind, and mean SpO2 was 89.3% ± 3.4%. The magnitude of pupillary contraction was greater with lower SpO2 (p < 0.01), and this dose relationship remained significant in multiple variable analyses (p = 0.047). Pupillary responsiveness to light stimuli under dark-adapted conditions was exaggerated with hypoxemia and may serve as an early predictor of chronic mountain sickness. This unexpected association is potentially explained as an excessive and unregulated sympathetic response to hypoxemia at altitude.
Introduction
O
Dysautonomia, an abnormality of function of the autonomic nervous system, is a well-established pathogenic aspect of chronic mountain sickness (Hainsworth, 2007; Rivera-Ch et al., 2007; León-Velarde et al., 2014). Past studies conducted in the Andes have found higher levels of sympathoexcitation on dynamic cerebrovascular autoregulation and reactivity and ventilatory control in high-altitude natives with chronic mountain sickness (Moore et al., 2006; Ainslie, 2012; Lewis et al., 2014). We postulate that individuals with chronic mountain sickness may have dysautonomia even in early stages of the disease. Evaluation of pupillary response can be used as a noninvasive technique to evaluate autonomic function (Bremner, 2009) and as such, if validated, could serve as a screening method for preclinical chronic mountain sickness. Pupillary responsiveness relies on a balance between the sympathetic and parasympathetic nervous systems (Heller et al., 1990). A study conducted by Bär et al. (2009) found that pupillary light reflex correlates with autonomic modulation of heart rate and blood pressure. Abnormal pupillary functioning has also been found in patients with heart failure that exhibit generalized adrenergic activation and parasympathetic withdrawal (Keivanidou, 2010).
Night vision is a highly oxygen-dependent process and can be compromised in even mildly hypoxic individuals (National Research Council, 1987). Dark adaptation, the visual adjustment that takes place when transitioning from high to low light, is characterized by dilation of the pupil and a shift from a cone- to rod-mediated visual process (Havelius et al., 1997). There is a well-characterized relationship between impaired dark adaptation and oxygen deficiency (Havelius et al., 1997; Havelius and Hansen, 2005). Past studies investigating the direct effect of insufficient oxygen on dark adaptation found that when participants were exposed to a low-oxygen environment, they had a marked decrease in light sensitivity and higher visual threshold than when under normobaric conditions (McFarland and Forbes, 1940; Wilson et al., 2008). In addition, acute altitude exposure is associated with decreased pupillary responsiveness to light in healthy humans (Cymerman et al., 2005; Wilson et al., 2008) and is likely due to the inhibitory effect of hypoxia on certain parts of the central nervous system. Little is known, however, about the effects of chronic hypoxic exposure on the visual process under low-light conditions or the potential impact of sympathoexcitation on autonomic function.
We aimed to evaluate the association between daytime oxyhemoglobin saturation (SpO2) and pupillary response to dark adaptation, assessed using a previously validated portable dark adaptometer (Labrique, 2015), in Peruvian adults permanently residing at high altitude.
Materials and Methods
Study sample
We conducted a cross-sectional study of dark adaptometry in Andean natives in the southeastern city of Puno, Peru (3825 m above sea level). Located on the shores of Lake Titicaca, Puno is home to a population of ∼150,000 residents, the majority of whom are Andean natives of Aymaran or Quechuan descent. Despite a primarily indigenous population, a recent study conducted in the region reported a 4.5% prevalence of chronic mountain sickness (De Ferrari et al., 2014), although past research have reported rates as high as 15% (Beall et al., 1992). In addition, 80% of Andean natives are estimated to suffer from hypoxia-induced ischemia (Beall et al., 1998).
This research was carried out as an ancillary study to a well characterized, population-based cohort in Peru (Miranda et al., 2012), in which 1000 adults aged ≥35 years were enrolled in Puno. We aimed to perform dark adaptometry testing in a stratified subsample of 100 participants from the Puno cohort. To obtain a wide range of oxyhemoglobin values, subjects were randomly selected according to previously collected SpO2 data. We selected an equal number of participants from among four strata corresponding to the following SpO2 categories: 75%–84%, 85%–90%, 91%–93%, and ≥94%. Verbal informed consent was obtained from all participants. Study protocols were approved by the Institutional Review Boards of Johns Hopkins Bloomberg School of Public Health (Baltimore, MD), Universidad Peruana Cayetano Heredia (Lima, Peru), and A.B. PRISMA (Lima, Peru).
Field assessment
We used data collected as part of the ongoing CRONICAS project to ascertain demographic, socioeconomic, and medical information. Face-to-face interviews were carried out by trained field workers using a standardized questionnaire at baseline and follow-up. Participants also underwent a clinical and anthropometric assessment and spirometry testing as part of the cohort study. Pulse oximetry was measured using a handheld device (Rad-5v; Masimo, Irvine) while participants were awake, upright, and resting comfortably (Luks and Swenson, 2011). Oxyhemoglobin saturation was recorded after the reading stabilized for more than 10 seconds. The Rad-5v has an oxyhemoglobin saturation accuracy range of 70%–100% with ±3%. Anthropometric measurements were taken in triplicate using standard techniques, described in detail elsewhere (Miranda et al., 2012). Biospecimen collection was described elsewhere (Miranda et al., 2012). Briefly, certified phlebotomists visited participants in the early morning to collect ∼13.5 mL venous blood samples following 8–12 hours fast, and laboratory testing was carried out at a centralized testing facility.
Dark adaptometry testing
Dark adaptation was tested using a portable dark adaptometer, a device designed specifically for use in challenging field settings that consists of a pair of light-obscuring goggles, Ganzfeld light emitting diode, infrared digital camera, and flash units for retinal bleaching (Labrique et al., 2015). Testing was controlled using a custom-designed laptop-based software program and consisted of a baseline retinal bleaching flash followed by a 10-minute period of dark adaptation. The 10-minute adaptation period was based on previous studies of dark adaptation and pupillary responsiveness (Congdon et al., 1995). Once participants were fully dark-adapted, an infrared mini-camera embedded inside the right eyepiece recorded the contralateral pupillary response to a stepwise series of 0.4 log-candela/m2 increments over nine calibrated light stimuli (−2.9 to 0.1 log-candela/m2). Each stimulus was displayed for 1 second with a 10-second rest period between stimuli. Pupil diameter was measured immediately preceding and following each light stimulus using the dark adaptometer video telemetry. Pupillary responsiveness was calculated as the percent change in pupil diameter from pre- to poststimulus (Fig. 1).
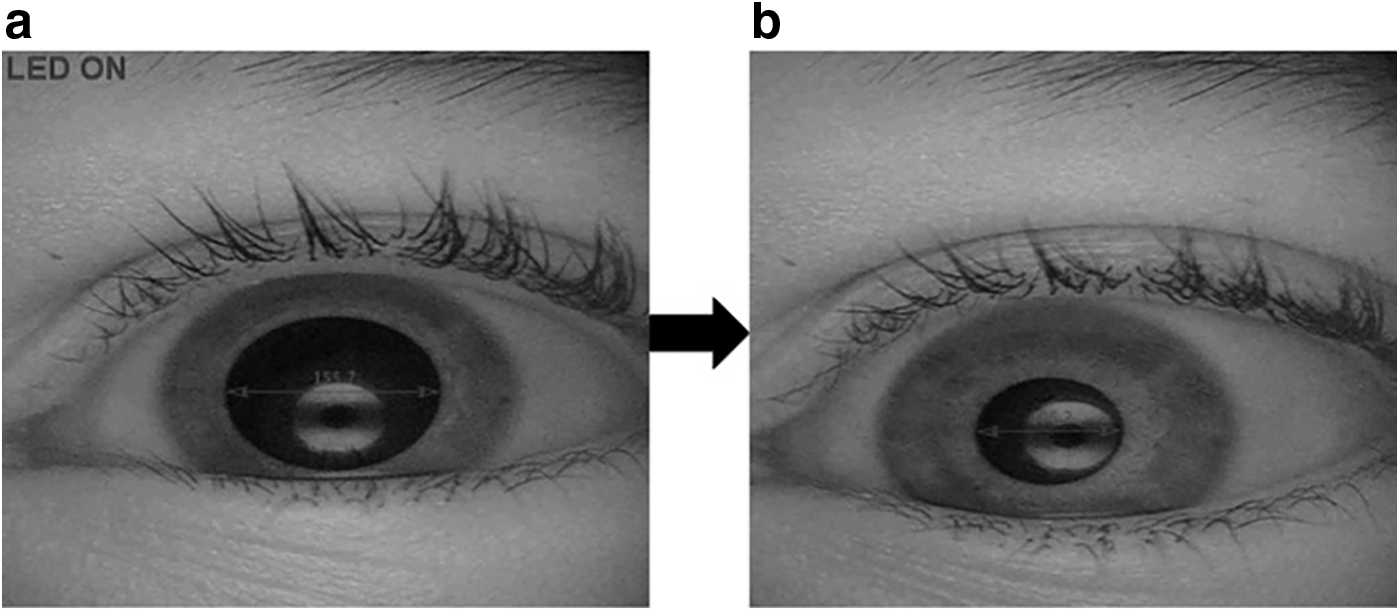
Infrared imaging allows the visualization of an eye in complete “dark-room” conditions and enhances pre
Biostatistical methods
The primary objective of this analysis was to evaluate the association between pupillary responsiveness and degree of hypoxemia in a dark-adapted state. Descriptive statistics were calculated for measured variables. Group differences were analyzed using the t-test or Wilcoxon rank sum test to compare differences for continuous variables and chi-square test for categorical variables. We defined pupillary response as the magnitude of pupillary contraction, calculated as the percent decrease in pupil diameter from pre- to poststimulus. Resting oxyhemoglobin saturation (SpO2) served as an indicator of hypoxemia and proxy for chronic mountain sickness. We used multilevel analyses to account for the hierarchical structure of the data, that is, repeated response measurements to light intensity nested within LED stimuli. We predicted pupillary responsiveness using linear mixed effects models. Fixed effects included SpO2 (as continuous variable), light intensity, age, sex, heart rate, and night blindness, and random effects accounted for individual- and stimulus-specific effects. Statistical analysis was carried out using Stata version 12 (Stata Corporation, College Station, TX).
Results
Participant characteristics
We successfully completed dark adaptometry testing in a total of 93 participants (48 urban vs. 45 rural residents). Mean (±standard deviation [SD]) age was 54.9 ± 11.0 years, 48.4% were male, and 44.1% self-reported night blindness. We summarized additional participant characteristics in Table 1 and found that rural participants were younger (p = 0.01), had a higher rate of night blindness (p = 0.01), higher SpO2 (p < 0.01), lower heart rate (p < 0.001), and lower body mass index (p < 0.01) compared to urban residents. Cigarette and alcohol use were uncommon in our sample. SpO2 ranged 78%–96% with a mean (±SD) of 89.3% ± 3.4% (Fig. 2).
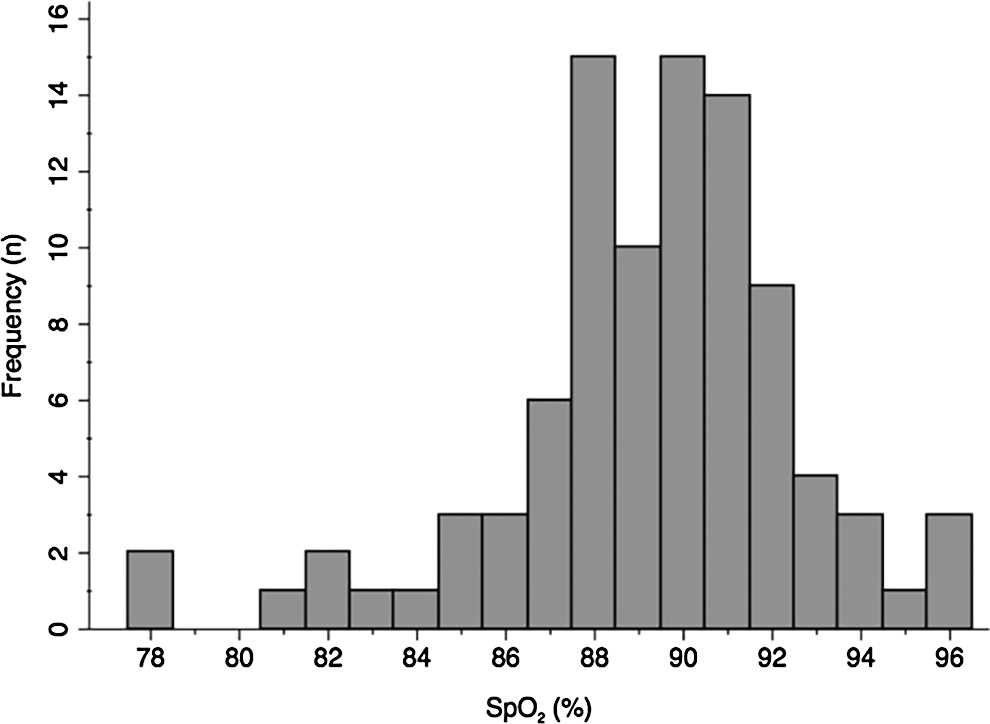
Distribution of SpO2 measurements among Peruvian adults (n = 93) permanently residing at high altitude.
Maximum of n = 13 missing values for any given variable.
BMI, body mass index.
Association between light intensity and pupillary responsiveness
We summarized pupillary responsiveness by stimulus intensity in Table 2. There was a significant increase in the magnitude of response associated with each stepwise increase in light intensity, ranging from −10.2 ± 7.6% at −2.9 log-cd/m2 to −34.7 ± 9.3% at 0.1 log-cd/m2 (Fig. 3). In unadjusted analysis, each stepwise increase of 0.4 log-cd/m2 in light intensity was associated with a 3.2% increase in the magnitude of pupillary response (Table 3). Rural residents showed greater pupillary responsiveness across all light stimuli than their urban counterparts (p < 0.001, data not shown). Heart rate and age were also found to be important factors for pupillary responsiveness in single variable analysis (Table 3). Light intensity remained positively associated with the magnitude of pupillary contraction (p < 0.001) following adjustment for heart rate, age, SpO2, sex, and night blindness, while older age was associated with decreased pupillary responsiveness (Table 3).
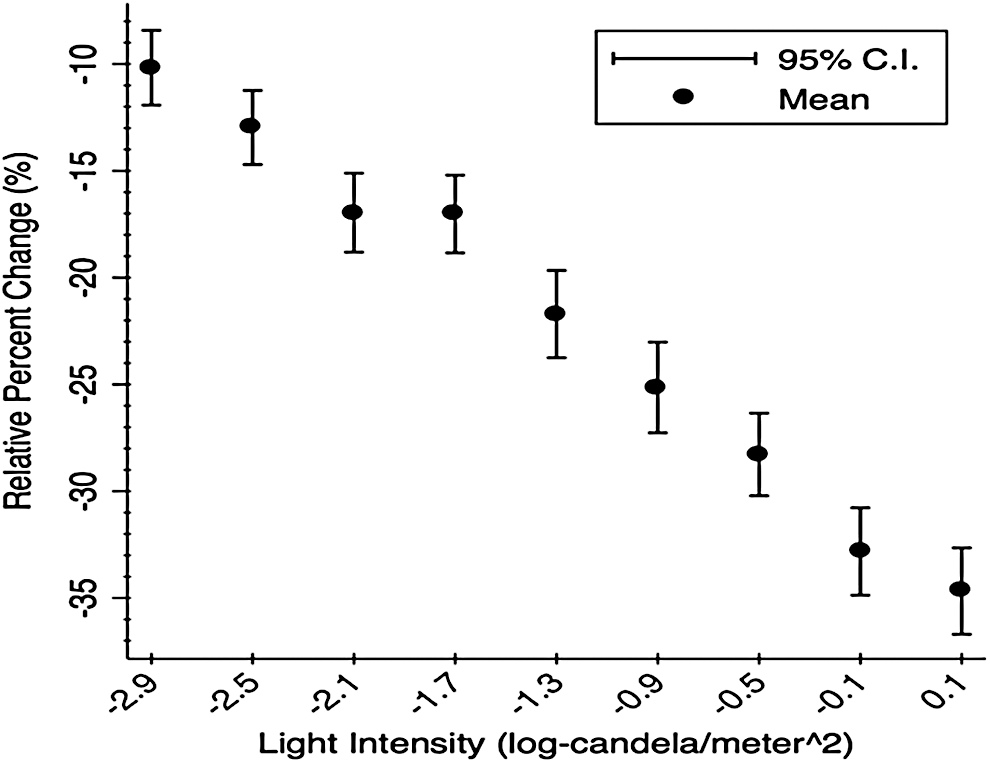
Relative percent change in pupil diameter from pre-to poststimulus among Peruvian highlanders (n = 93), by light intensity.
Data missing from a maximum of n = 18 subjects for any given variable.
Intensity reported in units of log-candela/m2.
Defined as relative percent change in pupil diameter from pre- to postlight stimulus.
SD, standard deviation.
Association between oxyhemoglobin saturation and pupillary responsiveness
We plotted fitted values of the average percent decrease in pupil diameter between stimuli intensities across a range of SpO2 values (Fig. 4). In single variable analysis, we found a significant, negative dose-dependent relationship between the magnitude of pupillary contraction and SpO2, irrespective of light intensity (Table 3; p < 0.01). This association was attenuated, but remained significant in a multivariable model adjusted for other independent factors, with a 0.46% decrease in the magnitude of pupillary contraction for every 1% increase in SpO2 (Table 3; p = 0.047).

Fitted values for pupillary response to light stimuli of varying intensity (log-cd/m2) across range of SpO2 values among Peruvian adults (n = 93).
Discussion
In this study, we found a negative association between hypoxemia and pupillary responsiveness, in which the worse the hypoxemia, the greater the magnitude of the pupillary contraction to light under dark-adapted conditions. We postulate that this exaggerated pupillary response was likely due to an overactive sympathetic nervous system in maladapted individuals. Hypoxemia was more common in urban living, male, and overweight participants, while impaired dark adaptation was most prevalent among rural residents. Elderly age was associated with both decreased pupillary responsiveness and SpO2. Self-reported night blindness was not associated with SpO2 or pupillary responsiveness.
Individuals with chronic mountain sickness are known to be maladapted to life at high altitude and are unable to maintain adequate oxygenation during long-term hypoxic exposure. This maladaptation may be indicative of dysautonomia (Keyl, 2003; Moore et al., 2006; Penaloza and Arias-Stella, 2007). A feasible interpretation considers that maladapted highlanders may evolve an overly sensitive sympathetic nervous system to address the problem of suboptimal oxygen. This would explain the heightened pupillary sensitivity to light seen in hypoxic study participants. A study conducted by Ainslie et al. (2012) found that chronic exposure to high altitude induced sympathoexcitation and, ultimately, led to impairment in dynamic cerebral auto regulation and increased cerebrovascular reactivity and ventilator control. In addition, research in Andean natives has shown that carotid baroreceptor control of vascular resistance is abnormal, and vasoconstrictor activity is greater in chronic mountain sickness patients compared to healthy highlanders (Moore et al., 2006). Sympathoexcitation in chronic mountain sickness patients would explain the extreme pupillary constriction magnitudes seen in individuals with low SpO2 values.
There are some potential shortcomings with our study. First, our sample size is small. Second, we did not collect a measure of autonomic balance, such as heart rate variability, at the time of testing. Third, there were several minor technical issues that arose with the dark adaptometer itself. The dark adaptometer had only one sized visor, which didn't fit all participants and, at times, may have resulted in light entering the goggles. This problem was particularly prevalent in women, who had smaller head circumferences. Fourth, the dark adaptometer only captured the contralateral pupillary response of the right eye. Only examining one eye prevented the detection of other visual abnormalities that may account for differences in pupillary contraction, although rare. Despite these minor technical challenges, our study has important strengths. The dark adaptometer is a novel device that addresses the need for a portable and field-friendly machine with a calibrated light source and its design creates a mobile dark room such that testing can be performed in a variety of settings (Labrique et al., 2015). In addition, testing is fast and noninvasive and can be carried out with minimal training, proving the device's ease of use for assessing dark adaptation (Labrique et al., 2015). Video recordings of the pupillary reaction to light stimuli allow for quantification of responsiveness, as well as the examination of subject-specific variability and trends over time.
Future research is needed on the topic of chronic mountain sickness and its association with autonomic functioning in Andean natives. Next steps include additional studies in Puno and other high altitude regions, with the assessment of heart rate variability and a larger sample size for increased power of the analytic methods, as well as comparison of healthy natives with those with chronic mountain sickness.
Conclusion
In this study, we found a negative relationship between hypoxemia and pupillary responsiveness, where the worse the hypoxemia, the greater the magnitude of the pupillary contraction to light stimuli under dark-adapted conditions. The exaggerated pupillary response to light stimuli under dark adapted conditions seen in individuals with severe hypoxemia is likely due to dysautonomia, characterized by an excessive and unregulated response to hypoxemia at altitude and manifested in the study as excessive sympathetic activation during the pupillary light reflex. There is a great need for further investigation into this newly identified relationship to better characterize the risks and predictive factors associated with the development of chronic mountain sickness in Andean natives. An early predictor would allow for early interventions focused on regulating the symptoms of chronic mountain sickness that are responsible for long-term development of chronic cardiopulmonary diseases.
Footnotes
Acknowledgments
The authors are indebted to all participants who kindly agreed to participate in the study. Special thanks to the field teams for their commitment and hard work.
Author Disclosure Statement
No competing financial interests exist.