
Abstract
Abstract
Semple, John L., G.W. Kent Moore, Petros Koutrakis, Jack M. Wolfson, Paolo Cristofanelli, and Paolo Bonasoni. High concentrations of ozone air pollution on Mount Everest: health implications for Sherpa communities and mountaineers. High Alt Med Biol. 17:365–369, 2016.—
Materials and Methods:
Surface ozone measurements were collected during ascending transects in the Mount Everest region of Nepal with passive nitrite-coated Ogawa filter samplers to obtain 8-hour personal exposures (2860–5364 m asl). In addition, the Nepal Climate Observatory-Pyramid, a GAW-WMO Global Station sited in the Khumbu Valley (5079 m asl), collected ozone mixing ratios with photometric gas analyzer.
Results:
Surface ozone measurements increased with altitude with concentrations that exceed 100 ppb (8-hour exposure). Highest values were during the spring season and the result of diverse contributions: hemispheric background values, the descent of ozone-rich stratospheric air, and the transport of tropospheric pollutants occurring at different spatial scales.
Discussion:
Multiple climate factors, including descending stratospheric ozone and imported anthropogenic air masses from the Indo-Gangetic Plain, contribute to ambient ozone exposure levels in the vicinity of Mount Everest that are similar to if not higher than those reported in industrialized cities.
Introduction
R
Global tropospheric ozone mixing ratios have doubled since preindustrial times, with current annual averages in the range of 30 ppb (UNEP/WHO, 2011). Major sources responsible for this increase are the combustion of fossil fuels and methane emissions, which is predicted to continue as developing countries industrialize (Ren and Tong, 2008; Silva et al., 2013). In addition to its geophysical properties, ozone is the most important oxidant in the troposphere where it is a major air pollutant (Ren and Tong, 2008; Silva et al., 2013). Ozone has been shown to be harmful to human health and has been associated with bronchitis, emphysema, asthma, and an increase in mortality (World Health Organization, 2006; UNEP/WHO, 2011).
Nepal is a mountainous country with an extreme variation in topography, including 8000 m high mountains and deep valleys, often with more than 2000 m altitude differences between the two (Egger et al., 2000). This unique terrain and the ensuing complex valley winds provide an efficient mechanism for the vertical uplift of air masses carrying pollutants from the heavily urbanized areas of South Asia and Indo-Gangetic Plain (IGP) (Egger et al., 2000; Engardt, 2008). Figure 1 shows a satellite image during the winter/premonsoon months, in which pollution from the industrialized lowlands of IGP can be seen to encroach upon the Himalaya. In addition, the cold temperatures and snow-covered terrain of the Himalaya can lead to an increased lifetime of ozone (Egger et al., 2000; Musselman and Korfmacher, 2014). Compounding the transport of ozone within the vertical uplift of pollutants from the lowlands is the downward transport of ozone in the form of stratospheric intrusions or tropopause folds associated with high-impact weather events (Bonasoni et al., 2008; Bracci et al., 2012). These intrusions can transport significant amounts of ozone-rich stratospheric air reaching down through the free troposphere toward the surface in mountain regions (Stohl et al., 1999; Zhu et al., 2006; Semple and Moore, 2008; Moore and Semple, 2009). The vertical distribution of ozone increasing with altitude in European and Asian mountain ranges has been reported as exceeding WHO standards and a potential health risk to those engaging in tourism and sport in those high altitude regions (Zhu et al., 2006). Air quality in mountainous regions has been reported to worsen with increasing elevation. In the Himalayas, wood and yak-dung stoves are common heat sources and so the air quality in villages is often poor, both indoor and outdoor, in the early morning and evening (Luks and Swenson, 2007; Ayres et al., 2009). Increasing elevation also leads to more intense solar radiation, which produces more accelerated photochemistry and greater ozone production from precursor elements. Finally, many mountain areas have extensive valley systems, in which frequent temperature inversions trap pollutants (Stohl et al., 1999; Luks and Swenson, 2007; Ayres et al., 2009; Ezzati et al., 2012).
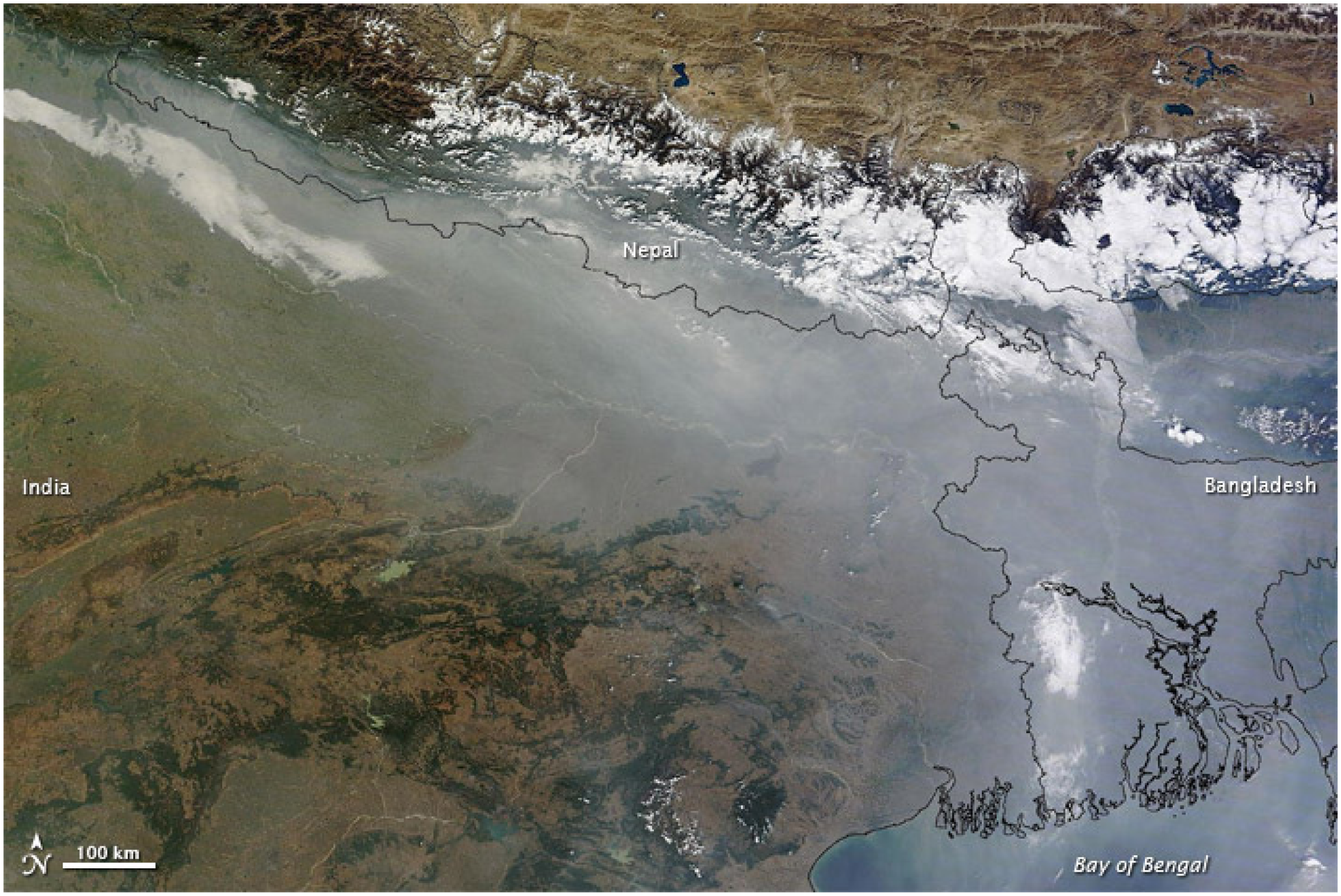
Modis true-color satellite image from December 5, 2011 showing pollution from the lowlands of India encroaching on the Himalaya. Clouds can be seen to penetrate up the steep valleys of Nepal toward Tibet. These cloud systems help transport pollutants, including ozone, up through these valley systems (image courtesy of NASA).
Materials and Methods
Two distinct measurement methods were used to measure ozone in the Khumbu Valley region. The first was fixed-site ozone mixing ratio data collected with an active photometric gas analyzer at the Nepal Climate Observatory-Pyramid WMO/GAW global station situated in the Khumbu Valley close to Mount Everest at an elevation of 5079 m asl for the period 2006–2011 (Bonasoni et al., 2008; Bonasoni et al., 2010; Bracci et al., 2012). In addition to the fixed location ozone measurements made at the Pyramid site, three ascending transects up the Khumbu Valley have been made in the Mount Everest region of Nepal during which portable passive nitrite-coated Ogawa filter samplers were used to obtain 8-hour personal exposures to ozone (2860–5364 m asl) (Koutrakis et al; 1993; Semple and Moore, 2008; Moore and Semple, 2009).
Results
The annual cycle in daily 8-hour ozone exposure at the Pyramid station is shown in Figure 2. The highest levels occur in the premonsoon, that is, spring, period with monthly mean 8-hour exposures from March through June exceeding the WHO guideline of 50 ppb (World Health Organization, 2006; EPA NAAQS, 2008; Moore and Semple, 2009). During April, the monthly mean exposure is 64 ± 8 ppb with a 95th percentile exposure of 78 ppb. The higher exposures during the spring are presumably the result of the contribution from the hemispheric background values, the increase in the occurrence and strength of pollution transport from the South Asia and Himalaya foothills, as well as stratospheric–tropospheric transport of ozone associated with the more frequent occurrence of tropopause folds during this period of the year (Zhu et al., 2006; Moore and Semple, 2009; Bracci et al., 2012). The lowest exposures occur in the monsoon, that is, summer period. During August, the monthly mean exposure is approximately half of that during April at 33 ± 6 ppb with a 95th percentile exposure of 43 ppb. These levels are the result of the monsoon circulation that limits stratospheric intrusions, as well as the meteorological conditions that are not favorable for photochemical production during the wet and cloudy summer season (Bracci et al., 2012). The ozone exposure values recover during the fall and winter with monthly mean 8-hour exposures approaching the maximum of the WHO guidelines (World Health Organization, 2006; EPA NAAQS, 2008).
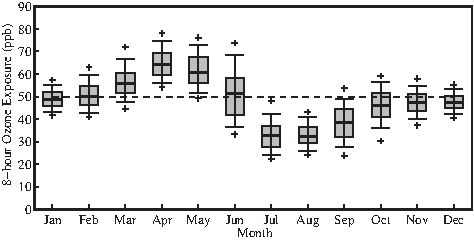
The annual cycle in 8-hour ozone exposure (ppb) at the Pyramid Laboratory at 5079 m asl based on hourly data from March 1, 2006 to December 31, 2010. The thick lines indicate the median values for each month. The boxes indicate the 25 and 75 percentile values for each month. The whiskers and the “+” represent the 10, 90, 5, and 95 percentile values for each month. Also indicated by the dashed line is the WHO guideline for 8-hour ozone exposure.
All measurements were recorded during ascending transects in the spring (premonsoon) period when the background ozone concentrations in the region are highest. The results of these transects are shown in Figure 3 and clearly indicate an increase in 8-hour ozone exposure with height with a linear least square fit of 22 ± 17 ppb/km and a correlation coefficient of 0.54 (p < 0.01). Above a height of ∼3500 m asl, the ozone exposures exceed the WHO guidelines (Cherrie, 2004; World Health Organization, 2006; EPA NAAQS, 2008).

The 8-hour ozone exposure (ppb) versus height on three transects in the Khumbu region (indicated by the three different colors of crosses), as well as the linear least square fit to the data. Also indicated by the dashed line is the WHO guideline for 8-hour ozone exposure.
Discussion
Previous studies have reported ozone concentrations on mountain ranges in the northern hemisphere as high as 100 ppb, including the Alps, the Rockies, and the Appalachians that have a vertical distribution, which increases with altitude in a similar profile to our findings on Mount Everest (Stohl et al., 1999; Moore and Semple, 2009; Musselman and Korfmacher, 2014). Several known factors favor persistent O3 levels at high elevation, including up valley transport downwind of urban industrialized areas, snow cover in high elevation ecosystems, and limited amounts of soil and plant surface area available to assist in the degradation of ozone (Stohl et al., 1999; Moore and Semple, 2009; Musselman and Korfmacher, 2014). Although reports have identified the potential toxic effects of high ozone levels to alpine forests and vegetation, few studies have investigated the potential negative health outcomes on populations that work and reside in mountain communities. The acute health effects of ambient ozone exposures have been examined in many low-elevation geographic regions. Potential adverse effects reported include decrements in lung function, airway inflammation, symptoms of asthma, increased rates of hospitalization, and mortality for those with preexisting respiratory disease (Cherrie, 2004; Luks and Swenson, 2007; Ezzati et al., 2012; Silva et al., 2013).
Mountaineers and High Altitude Exposure to Increased Ozone Levels
Exercise increases breathing rate, and thus, ozone dose which has been shown to significantly decrease lung function (McDonnell et al., 1983). Trekkers and hikers climbing at lower altitudes in the presence of increased ozone levels have been shown to have changes in lung function (McDonnell et al., 1983; Korrick et al., 1998; Demin and Beloglazov, 2008). Although ozone pollution has been shown to decrease lung function and potentiate pulmonary problems at sea level, currently, there is no evidence to suggest that visitors to high altitude with preexisting clinical conditions such as asthma and chronic obstructive pulmonary disease (COPD) would have compounded effects when exposed to these levels of ozone. Indeed, in general, short-term sojourners to the Everest region with these conditions have not been shown to be at a disadvantage (Huismans et al., 2010). Extreme exertion at high altitude already has multiple factors that potentially contribute to adverse pulmonary effects, including cold, dryness, hypoxia, and decreased barometric pressure. In high mountain areas, symptoms of ozone exposure are similar to those of acute mountain sickness. In addition, normobaric hypoxia, that is, a hypoxic state attained at sea level through the reduction in the concentration of oxygen, in the presence of ozone, has been shown experimentally to lead to increased exposure-related lung damage (Damji and Sherwin, 1989). The levels of ozone observed at these high altitudes in this study are significant even at sea level. The presence of ozone-rich air at above 5000 m by two different sampling methods revealed levels greater than 100 ppb (Ogawa samplers) and 63 ± 8 ppb at Pyramid for the corresponding time. Both values exceed the WHO guideline of 50 ppb for 8-hour exposures from the March through June period and are sufficiently high as to have a physiological impact on residents and visitors to the region (Stohl et al., 1999; Ayres et al., 2009; Moore and Semple, 2009).
The three sources of ozone that contributes to the overall annual total level in the high mountain areas of Nepal include: (1) local background sources (5%–10%), (2) descending stratospheric ozone-rich air (20%), and (3) the long distance transport of anthropogenic ozone pollution from the IGP of Northern India and other regions of Southeast Asia (70%) (Davies and Schuepbach, 1994; Bonasoni et al., 2008; Cristofanelli et al., 2010; Bracci et al., 2012; Fuzzi and Bonasoni, 2013). High-quality continuous measurements of trace gases, aerosols, and meteorological parameters have been previously conducted to obtain a detailed characterization of the background ozone composition of the polluted air-mass transport and variability in this Himalayan region (Davies and Schuepbach, 1994; Stohl et al., 1999; Moore and Semple, 2009). This is in contrast to the relatively “clean” stratospheric inputs, which are identifiable by having a clear fingerprint of their stratospheric origin (Davies and Schuepbach, 1994; Stohl et al., 1999; Moore and Semple, 2009). The annual peak level of ozone is observed to be highest during the spring climbing/trekking season (April–June). This spring period also represents the transition into the monsoon season when atmospheric modeling suggests that the primary source of this percentage increase of ozone is from the stratosphere (Davies and Schuepbach, 1994; Bonasoni et al., 2008; Cristofanelli et al., 2010; Bracci et al., 2012; Fuzzi and Bonasoni, 2013). The up valley winds associated with the monsoon are effective long distance transporters of anthropogenic pollution from industrialized cities of the IGP, which provide the largest proportion of annual ozone budget overall,11,12 and this source is the most concerning and the one that is most likely the major contributor to the future increasing ozone burden in the Mount Everest region (Egger et al., 2000; Bonasoni et al., 2008; Bracci et al., 2012). The rapid industrial growth in Asia and the anticipated increase in precursor emissions may continue to prove to be the most significant in health outcomes and ecosystems in remote regions (Semple and Moore, 2009; Fuzzi and Bonasoni, 2013). Indeed, it has been estimated that if the current global warming legislative environment remains in place, by 2030 surface ozone mixing ratios in the South Asia region will increase by ∼15% (Ren and Tong, 2008; UNEP/WMO, 2011). Recent future trend study indicated that substantial annual mean surface O3 reductions are expected by 2050 over most world regions, with the exception of South Asia where increases may be as large as 5 ppb (Wild et al., 2012).
Tropospheric ozone, under certain conditions, can have a prolonged lifetime and once above the boundary layer, can be transported over long distances, that is, intercontinental transport (Semple and Moore, 2009; Bonasoni et al., 2010).
Sherpa Communities and High Altitude Exposure to Increased Ozone Levels
Approximately, one-third of Nepal's adult population migrates internally or externally to find work. In the Everest Region of Nepal, this results in a heavy economic dependency on foreign money and a relatively mobile work population that must migrate to higher altitudes during the climbing and trekking seasons to participate in this new economy (Stevens, 1993; Law and Rodway, 2008). Perhaps the most vulnerable populations in Nepal are the Sherpa high altitude guides and lowland porters who are highly specialized in seasonal work. Indeed, these communities are undergoing a rapid social change by transitioning from a traditional agricultural subsistence to a remittance-based economy (Stevens, 1993; Law and Rodway, 2008). The premonsoon season coincides with the peak tourist/climbing season where the majority of Sherpas, porters, and visitors/trekkers/mountaineers are migrating to the higher altitudes and, therefore, are at a greater risk of exposure to the highest levels of ozone annually. Despite the increased ambient levels of ozone at high altitude, currently, there is no evidence that this additional toxic exposure has a compounding effect on preexisting disease attributed to indoor pollution (biomass burning and cooking) and smoking. Indoor pollution and smoking are considered to be the dominant factors implicated in the significant prevalence of COPD bronchitis, in Nepal, which increases with altitude in mountain communities (Pandey, 1984).
In this study, we draw attention to the multiple climatic factors and potential health risks compounded by the migrating patterns of indigenous Nepalese to very high altitudes (>3500 m) on or near Mount Everest where they are exposed to significant levels of ozone air pollution (well above WHO standards). These high concentrations are the result of the downward push of stratospheric ozone-rich air and the vertical uplift of air masses carrying pollutants from the heavily urbanized areas of South Asia and IGP.
Within the context of improving global health and health equity, we feel it is important to identify and advocate for those who work and reside in unique ecosystems that are currently invisible in the overall assessment of the global burden of climate-sensitive health outcomes.
The challenge for future research capacity in air pollution is to address mechanisms that directly affect population groups remote from the primary source of the pollution especially those exposed to multiple environmental hazards.
Footnotes
Acknowledgments
G.W.K.M. was supported by the Natural Science and Engineering Research Council of Canada. The authors thank Extreme Everest Research and the Italian National Research Council.
Author Disclosure Statement
No competing financial interests exist.