
Abstract
Abstract
Saugy, Jonas J., Laurent Schmitt, Sibylle Fallet, Raphael Faiss, Jean-Marc Vesin, Mattia Bertschi, Raphaël Heinzer, and Grégoire P. Millet. Sleep disordered breathing during live high-train low in normobaric versus hypobaric hypoxia. High Alt Med Biol. 17:233–238, 2016.—The present study aimed to compare sleep disordered breathing during live high-train low (LHTL) altitude camp using normobaric hypoxia (NH) and hypobaric hypoxia (HH). Sixteen highly trained triathletes completed two 18-day LHTL camps in a crossover designed study. They trained at 1100–1200 m while they slept either in NH at a simulated altitude of 2250 m or in HH. Breathing frequency and oxygen saturation (SpO2) were recorded continuously during all nights and oxygen desaturation index (ODI 3%) calculated. Breathing frequency was lower for NH than HH during the camps (14.6 ± 3.1 breath × min−1 vs. 17.2 ± 3.4 breath × min−1, p < 0.001). SpO2 was lower for HH than NH (90.8 ± 0.3 vs. 91.9 ± 0.2, p < 0.001) and ODI 3% was higher for HH than NH (15.1 ± 3.5 vs. 9.9 ± 1.6, p < 0.001). Sleep in moderate HH is more altered than in NH during a LHTL camp.
Introduction
T
Several possibilities to induce hypoxia could currently be used for LHTL. Simulated altitude, called normobaric hypoxia (NH), with reduction of the inspired fraction of oxygen (FIO2) can be used instead of the natural and terrestrial altitude, so called hypobaric hypoxia (e.g., a lower barometric pressure inducing a lower oxygen partial pressure, HH). Several slight physiological differences between NH and HH exposure have been reported (Millet et al., 2012; Richard and Koehle, 2012). Indeed, the minute ventilation (VE) is higher in NH than in HH with a combination of a higher tidal volume and lower respiratory frequency (Savourey et al., 2003; Conkin and Wessel, 2008).
Acute mountain sickness (AMS) symptoms have been shown to be less severe in NH than in HH (Loeppky et al., 2005) and the preacclimatization in “real” altitude (HH) resulted in significant decrease in severity of AMS when traveling to HH conditions, while it was not the case with NH preacclimatization (Fulco et al., 2013). Differences in fluid balance have also been observed with a higher diuresis and larger decrease in plasma volume for NH, while HH induced larger fluid retention (Loeppky et al., 2005; Conkin and Wessel, 2008). The nitric oxide (NO) in exhaled air or in plasma and the oxidative stress markers were also shown to be lower in NH than in HH after 10 hours of exposure (Ribon et al., 2016), 24 hours of exposure (Faiss et al., 2013), or 18 days of LHTL training (Debevec et al., 2015).
Taken together, these differences suggest different physiological responses to hypoxic exposure in “simulated” (NH) versus “real” altitude (HH) given similar inspired oxygen partial pressure (PIO2). Therefore, we can then speculate that the type of hypoxia (e.g., normobaric or hypobaric hypoxia) could influence the sleep in altitude in a different way between conditions, even with PIO2 strictly matched. Which could be the potential mechanisms underlying differences between sleep in normobaric and hypobaric hypoxia and their influence on the athletes' recovery? Several protocols have already studied the sleep disturbances either with NH (Fulco et al., 2011; Nespoulet et al., 2012; Hoshikawa et al., 2013) or HH (Latshang et al., 2013; Roach et al., 2013; Sargent et al., 2013), but never with a direct comparison on the same subjects.
The purpose of the present study was then to compare the sleep disordered breathing during a LHTL altitude training camp of 18 days either in NH or HH, with a crossover design, including a 1-year washout period between the two campaigns. Regarding all precedent studies on the differences between the two types of hypoxia, we hypothesized that HH would impair sleep breathing to a greater extent than NH.
Methods
Ethics statement
The study was approved by the regional medical ethics committee (Commission Cantonale Valaisanne d'Ethique Médicale, CCVEM; Agreement 051/09 and French National Conference of Research Ethics Committees; N°CPP EST I: 2014/33; Dijon, France). All experimental procedures conformed to the standards set by the Declaration of Helsinki. This study was part of a comprehensive research program investigating physiological, psychological, and performance adaptations of endurance athletes to normobaric and hypobaric LHTL protocol. Many methodological details are reported elsewhere (Saugy et al., 2014), but are also outlined in this study for the convenience of the reader.
Participants
Sixteen subjects participated in the study (data are mean ± standard deviation [SD]: age 24 ± 4 years, body height 179 ± 5 cm, body weight 70 ± 5 kg, and body mass index 21.8 ± 1.7 kg × m−2, VO2max 66.3 ± 7.5 mL × kg−1 × min−1, and Pmax 380 ± 48 W). All participants were informed about the experimental procedures and gave a written informed consent prior to start of the study. The participants were nonsmokers. They were living at or near sea level (i.e., <600 m) and were not exposed to altitudes above 2000 m for at least one month before the study.
Study design
This crossover designed study comprised two main experimental campaigns. Before the first campaign, the participants were equally assigned to either the NH or the HH LHTL protocol. A 1-year washout period was implemented between the campaigns to avoid any carryover effect from the first intervention. During the second campaign, the participants' conditions were crossed to complete the study crossover design. The intervention consisted of an 18-day LHTL phase performed in either NH or HH preceded by pretest and ending with posttest. During the LHTL phase, all participants performed supervised training sessions at altitudes between 1100 and 1200 m and resided at natural or simulated altitude of ∼2250 m. Peripheral oxygen saturation (SpO2) was measured during each night throughout the LHTL phase using a fingertip portable oximeter.
During the LHTL phase, the participants were asked to spend a minimum of 12 h/day in one to three person hypoxic rooms with conventional beds. The reduction of the O2 fraction (FIO2) was achieved and maintained using an oxygen extraction system (OBS, Husøysund, Norway) that delivered the oxygen-depleted air to the designated rooms. The system was calibrated before the start of the study using precision calibration gases. The levels of O2 and carbon dioxide were continuously monitored using designated probes in each room (OBS).
The simulated altitude in the rooms was kept constant throughout the protocol to maintain a simulated altitude of 2250 m (FIO2 = 18.05% ± 0.03%; Barometric pressure (PB) = 666.6 ± 3.6 mmHg; PIO2 =111.9 ± 0.6 mmHg; and simulated altitude ∼2250 m). The HH participants resided in a ski resort in the Swiss Alps (FIO2 = 20.9% ± 0.0%; PB = 580.2 ± 2.9 mmHg; PIO2 = 111.6 ± 0.6 mmHg; and altitude = 2250 m) throughout the terrestrial LHTL phase in one to five person rooms equipped with conventional beds (similar as in the NH rooms). On all nights, the fraction of inspired CO2 was between 0.25% and 0.45% and maintained below 0.5% (alarm set at 0.6%). There was no difference in CO2 level between the two conditions.
Measurements
Anthropometric values
Athletes' body weight and height were measured in the morning before the breakfast, and main body composition parameters were measured during pre- and posttests and twice per week during the LHTL camp.
Questionnaire
Daily Lake Louise questionnaires were filled directly after waking up in rooms (hypoxic rooms for NH and normal room in HH, but all in hypoxia) during the whole protocol.
Sleep breathing assessment
SpO2 and HR were recorded during all nights at 0.25 Hz with a wrist oximeter connected to a finger sensor (Wristox 3150 with 8000SM-WO Sensor; Nonin, Plymouth, MN). In addition, the number of times per hour of sleep that SpO2 level drops by 3% or more has been calculated throughout these night recordings (i.e., oxygen desaturation index = ODI 3%. The calculation is performed with a 60-second sliding window during the whole recording). Subjects were wearing an instrumented t-shirt (model SEW; CSEM, Neuchâtel, Switzerland) during all nights (including the two pre- and postnights). This device made of comfortable fabric measured the breathing frequency with an elastic sensor included in the textile and the sleeping position with accelerometers.
Data analysis and statistics
Data are reported as means and SDs. Data were tested for equality of variance (Fisher–Snedecor F-test) and for normality (Shapiro-Wilk test). When both conditions were met, a two-way ANOVA for repeated measures was performed with the two conditions (NH and HH). To determine the time effect for variables measured several times during the camps, all pairwise multiple comparison procedures were used (Holm-Sidak method). Differences between means in NH and HH were then compared using a paired t-test. Null hypothesis was rejected at p < 0.05. All analyses were made using SigmaPlot 11.0 software (Systat Software, San Jose, CA).
Results
Peripheral oxygen saturation
The peripheral oxygen saturation was higher for NH than HH during the whole camp (91.9 ± 0.2 vs. 90.8 ± 0.3, p < 0.001) and remained higher at post (94.4 ± 0.1 vs. 93.6 ± 0.2, p < 0.05). ODI 3% mean was significantly higher for HH than NH throughout the hypoxic nights (15.1 ± 3.5 vs. 9.9 ± 1.6, p < 0.001). The nightly ODI 3% was significantly higher in HH than NH from D2 to D14. No difference was found before and after the camp. The evolution of the ODI 3% during the camps is presented in Figure 1.
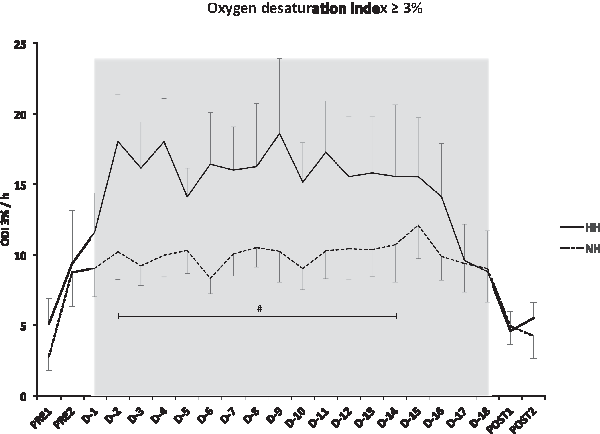
Values (mean ± standard error) of night oxygen desaturation index ≥3% per hour (ODI >3%). Pre1–Pre2: measurements before the camps (1150 m); D01–D18: measurement during the camps (NH: hypoxic room; HH: ski resort). #p < 0.05 for differences between conditions. ODI, oxygen desaturation index.
Heart rate
The mean nocturnal heart rate during the whole camp was higher for NH than HH (51 ± 1 bpm vs. 48 ± 2 bpm, p < 0.001).
Night breathing frequency
Although the night breathing frequencies were similar between the conditions during the two nights prior to the camps (14.4 ± 2.4 breath × min−1 vs. 15.1 ± 2.9 breath × min−1 for NH and HH, respectively), they were lower for NH than HH (14.6 ± 3.1 breath × min−1 vs. 17.2 ± 3.4 breath × min−1, p < 0.001) during the camps (D1–D18) and stayed lower the two nights following the camps (14.2 ± 3.4 breath × min−1 vs. 15.6 ± 3.1 breath × min−1, p < 0.01). These data are presented in Figure 2.
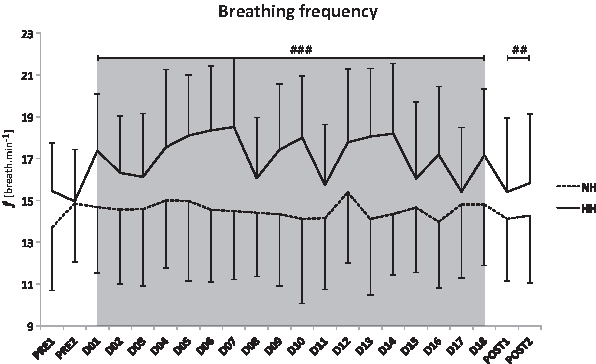
Values (mean ± standard error) of breathing frequency (f) measured during the night with instrumented t-shirts for NH and HH groups. Pre1–Pre2: measurements before the camps (1150 m); D01–D18: measurement during the camps (NH: hypoxic room; HH: ski resort). ##p < 0.01, ###p < 0.001 for differences between conditions.
Lake Louise Questionnaire
No positive Lake Louise score and no difference between conditions were found (1.2 ± 1.4 vs. 1.2 ± 1.6 for NH and HH, respectively).
Discussion
To our knowledge, this is the first crossover study comparing the sleep breathing during an 18-day LHTL altitude camp conducted either in NH or HH conditions. Lower night peripheral oxygen saturation levels and HR were noted in HH compared to NH. Moreover, a higher ODI 3% has been observed during the nights in HH. In addition, a lower nocturnal breathing frequency has been shown in NH compared to HH.
As stated before, sleep quality is known to be disturbed in hypoxia either with NH (Kinsman et al., 2003; Fulco et al., 2011; Nespoulet et al., 2012; Hoshikawa et al., 2013) or HH (Kinsman et al., 2003; Latshang et al., 2013; Roach et al., 2013; Sargent et al., 2013). The decreased oxygen fraction leads to hypoxemia, which is known to induce sleep perturbations (Fulco et al., 2011). In addition, Fulco et al. (2011) stated that sleep either in NH or HH characterized the altitude acclimatization as a result from numerous interrelated physiological adjustments that compensate hypoxemia. The progressive decrease in the end-tidal PCO2 (PETCO2) leads to an increase in peripheral oxygen level (SpO2) during the first days of moderate altitude residence in HH (Young and Reeves, 2002). A comparable degree of acclimatization was induced in NH with daily exposure to hypoxia (Muza, 2007).
Logically, SpO2 was lower in hypoxia than in the two control nights. Of interest is that SpO2 remained lower in HH compared to NH during and after the camps. These differences were also found at higher altitude with shorter expositions (Saugy et al., 2015). The reasons of this lower peripheral oxygen saturation in HH are still unclear. However, one may speculate that the barometric pressure modifies the fluid circulation and the transalveoli-capillary membrane flux, which might in turn induce greater pulmonary vasoconstriction in HH and then modify the oxygen diffusion by decreasing the pressure gradient between the alveoli and capillaries. In addition, the exaggerated oxidative stress generally reported in HH might affect NO bioavailability, which could impair oxygen unloading to tissues (Faiss et al., 2013; Ribon et al., 2016).
The oxygen desaturation index (ODI 3%) was significantly higher for HH compared to NH (Fig. 1) denoting a more disturbed sleep breathing than in NH. ODI 3% is considered as a reliable indicator of sleep apnea (Hang et al., 2015). This episodic breathing observed in HH might lead to intermittent hypoxia and, consequently, have clinical consequences: the desaturation–reoxygenation sequence is a typical pattern coupled with the majority of respiratory events defining intermittent hypoxia leading to oxidative stress with production of reactive oxygen species (ROS) (Lavie, 2003). This increase in ROS could generate vascular endothelial damage and dysfunction (Lavie, 2008). Altered baroreflex activity, increased pulmonary arterial pressure, and changes in heart structure are also potential deleterious causes of sleep disordered breathing induced by episodic breathing in intermittent hypoxia (Lavie, 2008).
The increase in ventilation is one of the first physiological adaptations when exposed to either normobaric or hypobaric hypoxia (Fulco et al., 2011; Dempsey and Morgan, 2015). This rise counteracts partly the reduction in oxygen transport induced by hypoxic environments. Ventilation and its associated parameters (i.e., PETO2, PETCO2, breathing frequency, and physiological alveolar dead space) have already been shown different between NH and HH (Savourey et al., 2003; Loeppky et al., 2005; Conkin and Wessel, 2008). In the present study, the breathing frequency was lower in NH compared to HH from the first to the last night in hypoxia and remained lower during the two following nights (14.6 breath × min−1 ± 3.1 vs. 17.2 ± 3.4 breath × min−1 for NH and HH, respectively, p < 0.001).
These later findings confirmed that NH is not a surrogate to HH (Conkin, 2016) and that NH and HH cannot be used interchangeably (Fulco et al., 2011; Saugy et al., 2014, 2015; Coppel et al., 2015; DiPasquale et al., 2015).
It can be assumed that these differences in nocturnal SpO2 and ventilation should have an influence on AMS, but no AMS has been reported. It is well known that AMS is not a problem for the majority of athletes between 2000 and 2500 m (Schommer et al., 2012) and that under 3000 m, the risk of developing acute altitude illness is very low (Luks et al., 2010).
The present study is unique: In a “real-world” setting, well-trained endurance athletes slept for two phases of 18-day in different hypoxia conditions, with a finger oximeter and an instrumented t-shirt to measure saturation and breathing frequency without disturbing the sleep quality and the training program. By signal analysis, ODI 3% was extracted. The use of polysomnography is not possible in these conditions because it would disturb the recovery of the athletes. Of interest is that the present results at a moderate altitude and with prolonged exposure confirm our results measured with polysomnography at higher altitude (3450 m) during one night where lower SpO2 and higher amount of ODI 3% were observed for HH compared to NH (Heinzer et al., 2016).
Nevertheless, it is important to note that despite the differences in night-time oxygenation, there were no resultant differences in performance outcomes (Saugy et al., 2016). In addition, one limitation is that subjective sleep quality assessment is not available. However, due to the slight differences in SpO2 and ODI 3%, one may question if these factors would impact the sleep quality that is known to be influenced by many environmental parameters (Bano et al., 2014).
Conclusion
Our results demonstrate for the first time with a crossover study that sleeping in moderate altitude during a LHTL altitude camp involved different physiological adaptations between NH and HH. First, HH induces lower nocturnal oxygen saturation compared to NH and a larger amount of ODI 3%. The present study adds elements to the growing body of evidences stating that NH and HH cannot be used interchangeably (Fulco et al., 2011; Millet et al., 2012; Saugy et al., 2014, 2015; Coppel et al., 2015). However, results should be handled with care considering the very individual side of altitude exposure responses (Chapman, 2013). Moreover, the ODI used is calculated from the raw SpO2 measurements and is an indicator of sleep apneas, but not as relevant as the parameters measured by polysomnography analysis.
Footnotes
Acknowledgments
This study was funded by grants from the Ministère des Sports, de la Jeunesse, de l'Education Populaire et de la Vie Associative (MSJEPVA)/Institut National du Sport, de l'Expertise et de la Performance (INSEP) and from Bundesamt für Sport (BASPO, Switzerland). The authors thank the director Vincent Jacquet and the staff of the National Ski-Nordic Centre (Prémanon, France), as well as the director Claudio Rossetti and the staff of the Feriendorf center (Fiesch, Switzerland), for their invaluable assistance and access to facilities. The authors also thank Swiss Center for Electronics and Micro technology (CSEM) for the use of the instrumented t-shirt and Olivier Girard for his help with the article.
Author Disclosure Statement
No competing financial interests exist.