
Abstract
Abstract
Luks, Andrew M., Colin Grissom, Luanne Freer, and Peter Hackett. Medication use among mount Everest climbers: practice and attitudes. High Alt Med Biol. 17:315–322, 2016.—The lay public, media, and medical experts have expressed concern about the ethics of climbers using medications to improve performance and increase the odds of summit success while climbing at high altitude, but the true incidence of this practice remains unclear. We conducted an anonymous survey of climbers who have attempted to climb Mt. Everest to gather information about medication use and attitudes toward medication and supplemental oxygen use while climbing the mountain. One hundred eighty-seven individuals completed the survey, providing information about medication and oxygen use for 262 expeditions to Mt. Everest between 1963 and 2015, the majority of which occurred after the year 2000. The majority of respondents were male (82%) and from English-speaking countries (75%). Medications were used on 43% of climbs, with acetazolamide being the most commonly used medication. Reported use of dexamethasone, nifedipine, sildenafil, or tadalafil was uncommon as was use of multiple medications at the same time. The majority of respondents indicated that it was acceptable for climbers to use medications and supplemental oxygen to prevent altitude illness while climbing Mt. Everest. Opinions were more mixed regarding whether summiting without the use of medications or oxygen carried the same value as reaching the summit using those interventions. Our data suggest that less than one-half of Mt. Everest climbers use medications during their expedition, with the primary medication used being acetazolamide, for prevention of altitude illness. Given the limitations of the study design and preliminary nature of these data, further research is warranted to further clarify these issues.
Introduction
M
One of the challenges in the discussion of these issues is that, at present, there is little to no systematic evidence about the extent to which Mt. Everest climbers are using medications in this manner. Anecdotal reports, including the case report and commentaries noted earlier, are evidence that medication use and abuse are occurring, but the true incidence is unknown and it remains unclear whether this is a widespread or sporadic practice. To further inform discussions on this question, we surveyed climbers who have attempted to climb Mt. Everest (8852 m) and inquired about their use of medications during their expeditions as well as their attitudes toward the use of medications and supplemental oxygen among climbers on the mountain.
Methods
After obtaining approval from the Institutional Review Board at the University of Washington, we conducted an anonymous survey of individuals who have attempted to climb Mt. Everest. The survey was conducted between November 2014 and July 2015.
Subjects
Men and women were eligible to participate if they attempted to climb the mountain on at least one occasion. Successfully reaching the summit was not required for participation. No restrictions were placed on the year in which the climbers made their attempt. Due to the abrupt cessation of climbing activities in 2014 and 2015 resulting from significant natural disasters, few climbers who attempted the mountain in those years participated in the survey.
We recruited subjects by several means, including posting survey announcements on websites, listservs and Internet discussion boards focused on mountain climbing, announcements in national and local mountaineering society newsletters, and through distribution of survey announcements by commercial guiding companies in the United States, the United Kingdom, and New Zealand to clients who had previously attempted to climb the mountain. Information about the survey was also sent to a list of climbers who had visited the Himalayan Rescue Association Medical Clinic at Everest Base Camp and provided their contact information. Survey respondents were free to forward the study information to other individuals at their discretion. The survey announcement included a URL for the anonymous on-line survey. Respondents who clicked on the URL were directed to a webpage, with further information about the study. Those who agreed to participate after reading that information were then directed to the start of the survey.
The survey
The survey was conducted via the Catalyst system, a web-based platform run from the University of Washington servers with multiple functions, including survey creation and administration. The survey took ∼15–20 minutes to complete and consisted of three sets of questions, including: (1) introductory questions regarding demographics and prior high altitude climbing history; (2) questions about their Mt. Everest climbs, including basic information about each climb (e.g., route, commercial vs. private expedition, highest altitude reached) and medication and oxygen use during the expedition; and (3) questions about their attitudes on the use of medications and supplemental oxygen by themselves and other climbers at high altitude. The survey was only available in English.
For the questions regarding medication use, respondents were asked whether they used acetazolamide, dexamethasone, nifedipine, sildenafil, tadalafil, salmeterol, or dextroamphetamine. The generic name for each medication was listed in the survey along with up to two English trade names. Respondents were asked to choose from a pre-specified list of reasons for why they took each medication, including prevention of altitude illness, treatment of altitude illness, increasing odds of summit success, and improving exercise capacity. Free responses to this question were not elicited. Climbers were allowed to report multiple reasons for using a particular medication.
Individuals who have made multiple attempts to climb Mt. Everest were allowed to provide information on up to three expeditions. Individuals who participated in >3 expeditions were asked to answer questions for their three most recent climbing attempts.
Attitudes regarding medication and supplemental oxygen use while climbing Mt. Everest and other 8000 m peaks were assessed by having respondents state their level of agreement to various statements by using a 5-point Likert scale.
Data analysis
Where applicable, data are presented as mean ± standard deviation. Due to the limitations of the study design, we did not make comparisons between subgroups of participants such as between guides and clients, between men and women, or between climbers of different nationalities. Because subjects were not required to answer all questions in the study, the total number of respondents to a particular question does not necessarily equal the total number of study participants.
Results
A total of 187 individuals completed the survey, providing information about medication use for 262 expeditions to Mt. Everest. Demographic data are provided in Table 1. More men than women completed the survey (82% vs. 18%), and the majority of respondents were from the United States (43.5%). Respondents participated in a total of 315 expeditions, with an average of 1.7 ± 1.6 attempts to climb the mountain and an average summit success rate of 69% ± 41%. The majority of survey respondents (70%) have participated in a single Everest expedition. The maximum number of summit attempts among survey respondents was 10. As noted earlier, respondents who participated in >3 expeditions were asked to answer questions for their three most recent climbing attempts, which explains why data are reported for 262 of the 315 expeditions. The majority of summit attempts for which data were provided took place after the year 2000 (Fig. 1).

The years in which survey respondents attempted to climb Mt. Everest. Each respondent could report data on up to three attempts to climb the mountain.
SD, standard deviation.
Table 2 displays basic information regarding the 262 expeditions for which survey respondents provided information about medication use during their expedition. The majority of climbers attempted the South Col route from Nepal (70%) and were clients on commercial guided expeditions (75%). Eighty-five percent of respondents used supplemental oxygen during their climb. Sixty-two percent reached the summit.
Survey respondents could provide information about medication use for up to three expeditions. Subjects providing information on more than one climb were asked to provide information on their three most recent attempts.
Table 3 displays information about medication use by survey respondents during their Everest expeditions. The reported percentages are calculated based on the climbers who provided a response as to whether they used or did not use medications. The majority of survey participants (57%) did not use any medications. Ninety-two climbers (35%) used only one medication, whereas 16 (6%) used two medications and 4 (2%) used three medications. Acetazolamide was the most commonly used medication, with 43% reporting use during an expedition. Figure 2 displays the percentage of climbers reporting use of the individual medications based on the time period in which they completed their climb.
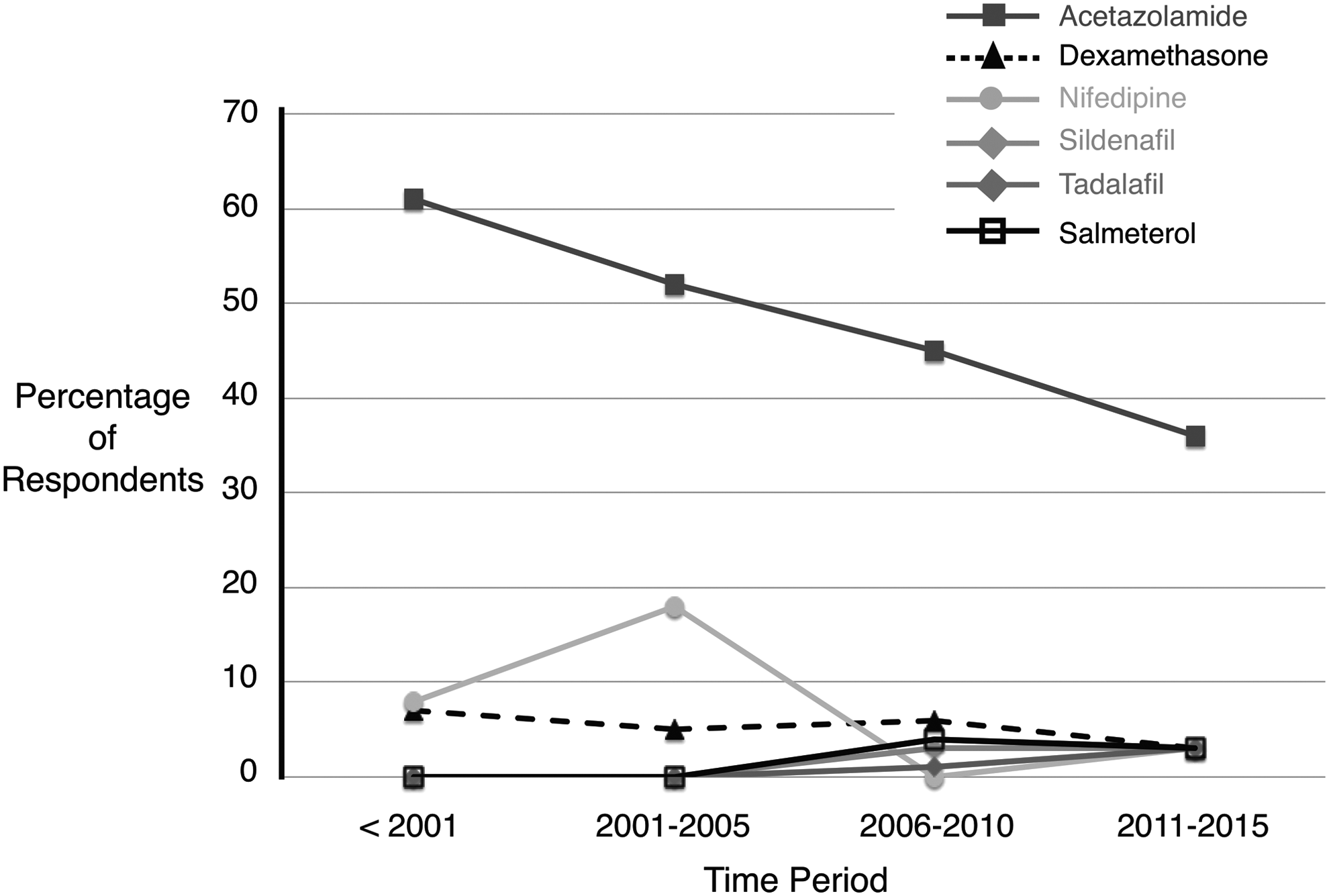
Reported use of altitude illness medications based on the time period in which the climbers attempted to summit Mt. Everest.
Percentages are based on the number of people who responded to the question.
Table 4 displays the reported reasons for taking each medication. Table 5 describes how climbers obtained the medications. Among climbers who provided a response, the most common source was the climber's primary care provider.
Respondents could report more than one reason or using a medication. Percentages are calculated based on the number of respondents who used the medication.
Respondents could report using more than one source of medications.
Table 6 displays information on attempts to climb other 8000 m peaks and whether the respondents used medications to prevent altitude illness or improve exercise capacity and chances of summit success. Cho Oyu was the most commonly attempted mountain among these peaks. Acetazolamide was the most commonly used medication on these expeditions. Use of the other medications was highly uncommon.
Figure 3 display responses to Likert-scale questions regarding attitudes about use of medications. The majority of respondents (64%) agreed that it is okay for climbers to use medications for preventing altitude illness, whereas a larger majority (92%) supported use for treatment. Although the majority felt that the use of medications while climbing Mt. Everest should be a personal decision, opinion was mixed as to whether climbers should be free to use whatever medications they feel are necessary to reach the summit and just more than one-half of respondents felt that medication use constituted an unfair advantage.

Participant's level of agreement with statements regarding medication use while climbing Mt. Everest. For each statement displayed on the left, participants were asked to state whether they strongly agreed, agreed, had no opinion, disagreed, or strongly disagreed.
Figure 4 displays responses to Likert-scale questions regarding attitudes about use of supplemental oxygen. A large majority of respondents felt it is okay for climbers to use supplemental oxygen on Mt. Everest and that this should be a personal decision. The majority of respondents also indicated that summiting with the use of supplemental oxygen did not carry the same value in their mind as summiting without oxygen and that use of supplemental oxygen constituted an unfair advantage.

Participant's level of agreement with statements regarding supplemental oxygen use while climbing Mt. Everest. For each statement displayed on the left, participants were asked to state whether they strongly agreed, agreed, had no opinion, disagreed, or strongly disagreed.
Discussion
This is the first study to investigate the frequency of altitude illness medication use among climbers who attempt to summit Mt. Everest. The results show that the majority of climbers do not use medications for altitude illness prevention or treatment while climbing the mountain. Among the minority of climbers who reported using medications, acetazolamide was the most commonly used drug. Dexamethasone, nifedipine, tadalafil, and sildenafil were infrequently used, as were combinations of altitude illness medications. Climbers generally feel it is appropriate to use medications for the purpose of preventing or treating altitude illness, as well as to use supplemental oxygen when climbing at an extreme elevation.
Our findings are similar to those demonstrated in the only other study assessing the frequency of medication use among climbers. In a study on Mont Blanc, Robach et al. (2016) used a novel approach to collect urine blindly and anonymously from male climbers at two mountain huts on a common route to the summit and to screen the samples for a wide range of drugs, including diuretics, glucocorticoids, stimulants, hypnotics, and phosphodiesterase inhibitors. Of the 430 samples analyzed from the two huts, 35.8% contained at least one medication. As was the case in our study, acetazolamide was the most commonly used medication, with 20.6% of samples testing positive across the two huts, whereas glucocorticoids were detected in only a small percentage of samples; phosphodiesterase inhibitors were not detected in any samples. As was also the case in our survey, concurrent use of multiple medications was uncommon, as only 33 samples (7.7%) tested positive for more than one substance. Due to some logistical issues in the study, such as the fact that samples were not collected from women and the study technique did not account for collection of multiple samples from the same individual, the reported percentages in this study may not accurately reflect the true percentage of climbers using medications, but the general pattern of results is valid and in agreement with what we observed in terms of the frequency and pattern of medication use. Use of supplemental oxygen is not routine on mountains under 8000 m, so this practice was not investigated in their study.
It should be noted that there are several reasons why our data may not reflect the true incidence of medication use among climbers. First, we had a relatively high percentage of climbers who did not report answers when asked about medication use during their expedition (Table 3), particularly for medications other than acetazolamide. To the extent answers were not provided because survey respondents were not willing to admit to use of these medications, this would lead to underestimation of medication use. We feel this problem was likely minimized, however, by the fact that the survey was conducted anonymously and respondents were not asked to provide any identifying information. The anonymous nature of the survey was made apparent to participants in survey announcements as well as at the start of the survey.
A second reason why we may underestimate the incidence of medication use is that unlike in the study by Robach et al., we did not inquire about the use of sedative-hypnotic agents by survey respondents. These medications were not included, because, in contrast to the medications in our survey, sedative-hypnotics are not generally viewed as options for prophylaxis or treatment of acute altitude illness (Luks et al., 2014). By improving sleep, however, these agents might indirectly increase the odds of a climber reaching the summit. Because they were omitted from our study, our data may not accurately reflect the overall incidence of medication use among climbers for the purpose of improving the chances of summit success.
Another difference between our study and that of Robach et al. is that our study design permitted us to inquire about the reasons for medication use among the climbers. The majority of people who used acetazolamide (69%, Table 4) indicated that they used it for prevention of acute altitude illness, and more than 60% of survey respondents supported using medications for this purpose (Fig. 3). Interestingly, even though prevention of altitude illness should ostensibly increase the odds of summiting a mountain, the respondents in our survey appear to draw a distinction between these purposes, as only 17% indicated that they used acetazolamide to increase the odds of reaching the summit and more than 60% either disagreed with or had no opinion regarding the use of medications to increase the chances of reaching the summit (Fig. 3). Because our data are insufficient to understand the complex reasons for these discrepancies, further investigations into climbers' motivations for using medications are warranted. In such studies, it would be useful to inquire how many climbers used acetazolamide to improve sleep, a question we did not ask in our study, because, as noted earlier, better sleep may be construed by some as increasing the chance of summiting the mountain.
The findings from our study and that of Robach et al. (2016) are useful for several reasons. First, they are an initial step toward informing discussions around the ethics of medication use while climbing at high altitude. To date, claims about the extent and purposes of medication use have been based largely on anecdotal reports rather than on systematically collected data. These two studies attempt to address that issue and suggest that rather than substantial numbers of climbers, only a minority may be using medications during expeditions on two major climbing objectives—Mont Blanc and Mt. Everest.
Second, the data from our study highlight opportunities to provide adequate counseling to climbers about the utility of these medications at high altitude and their safety and potential side effects, particularly when used in unstudied combinations. Although data demonstrate that the medications included in our survey are useful for preventing and treating altitude illness (Luks et al., 2014), only a few of the medications, including sildenafil (Ghofrani et al., 2006) and dexamethasone (Siebenmann et al., 2011), have been shown to increase exercise capacity in hypoxia and, therefore, might affect climbing performance. Acetazolamide, on the other hand, has been shown to have either no effect (Hackett et al., 1985; Faoro et al., 2007) or an adverse effect on exercise performance in healthy individuals at 3450–6900 m (Gonzales and Scheuermann, 2013; Bradwell et al., 2014). Our data indicate that opportunities for such counseling exist. Sixty-eight percent of those who provided information on this question indicated that they obtained their medications from sources who, with effective education, could provide adequate counseling, including primary care providers, travel medicine clinics, expedition physicians, or the Himalayan Rescue Association (Table 5). It should be noted, however, that 41% of survey respondents did not provide information on where they obtained their medications. To the extent this reflects individuals who self-prescribed medications, there may still be a substantial number of individuals who would not be accessible for such counseling.
Although our data provide a useful starting point for further research into these questions, caution is necessary in drawing firm conclusions from our results. Due to limitations in our study design, the data may not reflect the practices of the full spectrum of current Mt. Everest climbers. Because our study was published in English only, the majority of respondents (∼75%) were from English-speaking countries, with the largest percentage of respondents (49.5%) coming from the United States. These values are higher than the percentage of climbers from English-speaking countries (32.8%) or the United States (16.8%) who have gone above Everest Base Camp while attempting to summit Mt. Everest between 2000 and 2015 (Himalayan Database, 2004). Importantly, we did not capture climbers from China, which represents 6.6% of summit attempts between 2000 and 2015 (Himalayan Database, 2004), and other areas of Asia and the India subcontinent. As a result, our results may not reflect the practices or attitudes of climbers from the large number of countries that attempt to climb the mountain each year.
Another issue is that although we had a large number of respondents to our survey, these responses reflected climbs conducted over a nearly 30-year period. For any given year, we have responses for only a minority of the now hundreds of climbers who attempt to summit the mountain each year. Finally, due to the avalanche disaster in the Khumbu icefall in the spring of 2014 and the Nepal earthquake in the spring of 2015, only a handful of climbers attempted to summit Everest in those years and only a limited number of individuals reported data for climbs during those years (13 for attempts in 2014 and 1 for 2015). As a result, our results may not fully reflect the most current medication practices of the majority of Everest climbers. To address this concern, we examined reported medication use according to the time period in which survey respondents attempted to climb the mountain. The trends in usage for each medication are displayed in Figure 2. In examining these data, it should be noted that no climbers reported using salmeterol, sildenafil, or tadalafil before 2006, which is not surprising given that the study showing the effects of long-acting beta agonists in individuals susceptible to high altitude pulmonary edema was only published in 2002 (Sartori et al., 2002), whereas evidence regarding the effects of phosphodiesterase inhibitors on maximum exercise capacity was published in 2006 (Ghofrani et al., 2006). This is in contrast to the situation with acetazolamide, dexamethasone, and nifedipine, as data regarding their utility were available in the literature much earlier.
In addition to issues regarding generalizability of the results, another limitation of our study is the potential for both self-reporting and recall biases, particularly for subjects reporting information about climbs that took place many years ago. The effect of recall bias will likely vary based on the particular question being considered. For issues with discrete answers such as the route climbed or whether or not a medication was used, we would anticipate less effect from this form of bias; whereas for questions involving the reasons for a decision or the timing or purpose of medication use, the effect may be greater.
Despite these limitations, our study represents the first attempt to answer questions about the extent to which Mt. Everest climbers are using medications during their attempts to summit the mountain and suggests that the problem may not be as widespread as thought based on the prior anecdotal reports. Further research is warranted to clarify the frequency of medication use among Everest climbers. Because study techniques such as those used by Robach et al. (2016) on Mont Blanc would be difficult to implement in the field in Nepal or Tibet, further efforts could focus initially on conducting more surveys in multiple languages at base camp on the south and north side of the mountain during the climbing season over a several-year period, which would allow access to a larger number of climbers from a broader number of countries than we achieved in our study. The information gleaned from further studies will help inform ongoing discussions about the ethics of medication use while climbing the mountain and also provide information that can be used when counseling climbers about the efficacy and safety of such practices.
Footnotes
Acknowledgments
The authors would like to thank Richard Salisbury for providing information from the Himalayan Database.
Author Disclosure Statement
No competing financial interests exist.