
Abstract
Abstract
Riley, Callum James, and Matthew Gavin. Physiological changes to the cardiovascular system at high altitude and its effects on cardiovascular disease. High Alt Med Biol. 18:102–113, 2017.—The physiological changes to the cardiovascular system in response to the high altitude environment are well understood. More recently, we have begun to understand how these changes may affect and cause detriment to cardiovascular disease. In addition to this, the increasing availability of altitude simulation has dramatically improved our understanding of the physiology of high altitude. This has allowed further study on the effect of altitude in those with cardiovascular disease in a safe and controlled environment as well as in healthy individuals. Using a thorough PubMed search, this review aims to integrate recent advances in cardiovascular physiology at altitude with previous understanding, as well as its potential implications on cardiovascular disease. Altogether, it was found that the changes at altitude to cardiovascular physiology are profound enough to have a noteworthy effect on many forms of cardiovascular disease. While often asymptomatic, there is some risk in high altitude exposure for individuals with certain cardiovascular diseases. Although controlled research in patients with cardiovascular disease was largely lacking, meaning firm conclusions cannot be drawn, these risks should be a consideration to both the individual and their physician.
Introduction
E
Considering the increasing prevalence of CVD as well as the large number of individuals constantly exposed to high altitude for work or leisure, understanding the possible links between high altitude and CVD is of obvious clinical importance. Recent investigations using altitude simulation as well as a few real-life studies have shone new light on these links.
This review integrates more recent findings of how altitude affects the CVS both acutely and chronically with those already laid out by previous reviews. This was done using a PubMed search for relevant keywords, namely the title of each subdivided section coupled to “high altitude,” “hypoxia,” “hypobaric,” and “altitude simulation.” Only articles published after and including the year 2000 were initially considered. In several searches, multiple results for studies in patients with chronic obstructive pulmonary disease (COPD) and other pulmonary diseases were found. In these incidences, “pulmonary disease,” “sleep apnea,” and “COPD” were excluded from our searches. One hundred twenty-five articles were selected for initial review, and from these, 82 were selected for inclusion into this review based on each article's own merits, avoiding articles using animal models on topics not discussing biochemistry and giving large weight to sample size due to the generally small samples used in studies on this topic. Within these articles, references thought to be particularly relevant to a topic in question were also included. Generally, these are seminal articles published before 2000 within this review.
Second, it aims to collate the current evidence from both laboratory-based and real-world studies on how these changes to the CVS brought about by altitude may affect individuals with CVD.
The effects of subacute, acute, and chronic altitude exposure on the cardiovascular system are summarized in Figure 1.
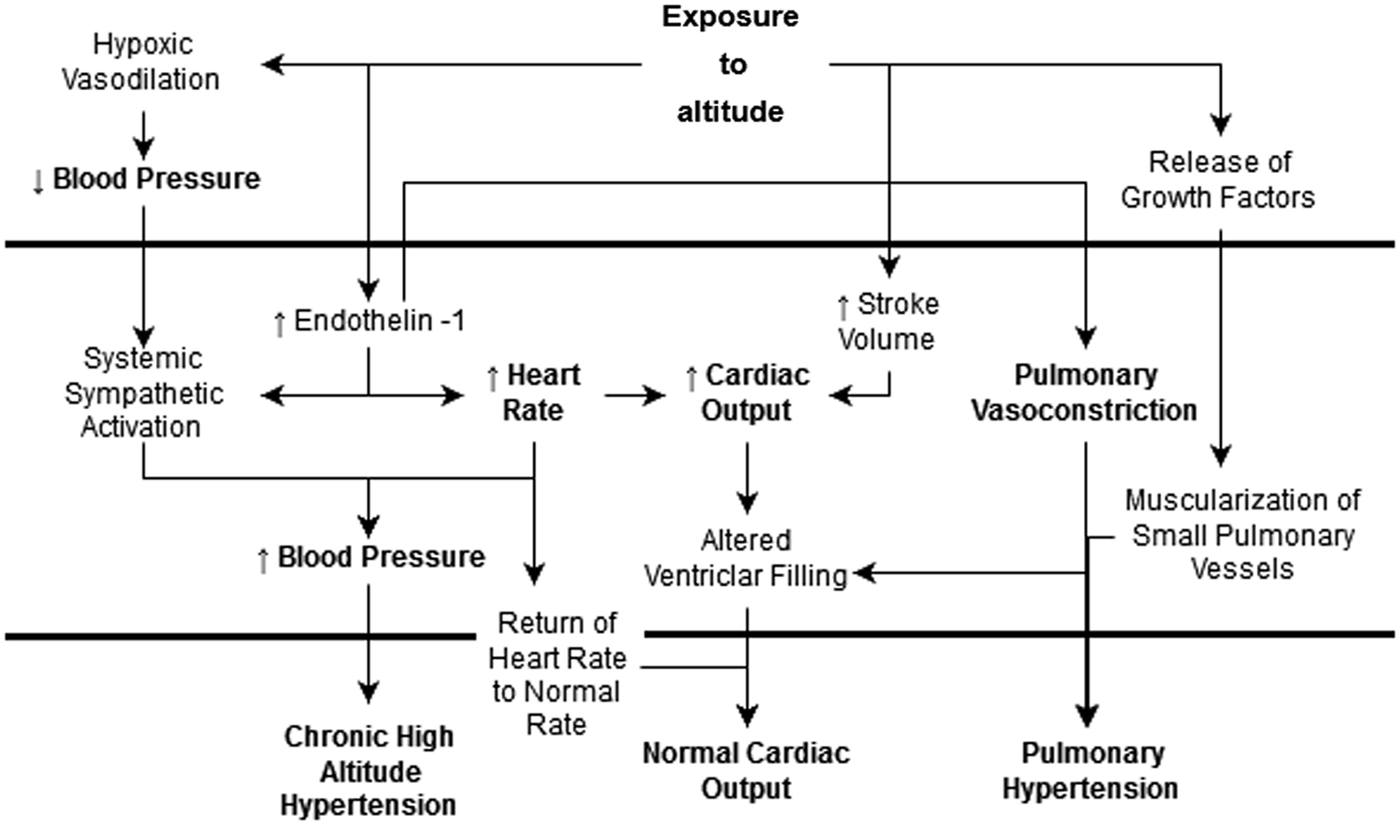
Flowchart summarizing the important physiological changes in cardiovascular physiology with both acute and chronic altitude exposure. The diagram is divided into three by two horizontal lines; at the top, are those changes that occur subacutely; in the middle, acutely; and at the bottom, chronically. This flowchart highlights the importance of endothelin-1 as a key regulator of heart rate, blood pressure, and pulmonary vasoconstriction.
The Effects of Altitude on CVS Physiology
Heart rate
An increase in heart rate (HR) is one of the earliest responses to high altitude. In a recent study of 139 healthy men, HR increased by 20.44 beats min-1 at an altitude of 3700 m compared with 500 m (Rao et al., 2015). However, the mechanism behind this increase, particularly during exercise, is only partially understood. Undoubtedly, increased sympathetic activity and circulating catecholamines play an important role in increasing HR at rest, and while some studies report that preliminary administration of beta blockers can overcome this increase (Mirrakhimov and Winslow, 2011), others have shown that at rest, only a blockade of both sympathetic and vagal activities simultaneously can completely overcome the rise in HR induced by hypoxia (Siebenmann et al., 2015). It is therefore likely that both vagal withdrawal and an increase in sympathetic activity are responsible for the rise in resting HR with altitude.
With chronic altitude exposure, there is enhanced parasympathetic activity, causing a decrease in maximum HR. The change in HR during exercise is also decreased from sea-level values (Boushel et al., 2001). At rest, however, data are conflicting on whether HR is normalized or maintains slightly elevated with acclimatization (Siebenmann and Lundby, 2015).
While important at rest, vagal withdrawal appears to play a more central role during exercise-induced tachycardia in hypoxia. Siebenmann et al. (2015) showed that propranolol had no effect on exercise-induced tachycardia at altitude. Similarly, with a combination of beta-adrenergic and muscarinic blockade (a combination that reversed hypoxic tachycardia at rest), there was only partial reversal of HR increase. This suggests there are other factors at play. The same study suggests that cardiac alpha adrenoceptors may respond to increased levels of circulating catecholamines to regulate HR at altitude. Historic animal studies have also elicited that pulmonary stretch receptors may play a role in regulating HR in this environment, although the mechanisms of this are poorly understood and may simply be through an increase in sympathetic activity (Mirrakhimov and Winslow, 2011). Both these possibilities, particularly the role cardiac alpha receptors play in regulation of HR in hypoxia, need further study.
It is also possible that endothelin-1 (ET-1) plays a role in regulation of HR at altitude. It is known that receptors for ET-1—a potent vasoconstrictor peptide—are expressed in cardiomyocytes (Ito et al., 1993). As discussed in the Pulmonary circulation section, ascent to high altitude is associated with higher plasma ET-1 (Goerre et al., 1995). Activation of the ET-1 b-type receptors in cardiomyocytes stimulates a leak of calcium ions from the sarcoplasmic reticulum, delivering positive inotropic and chronotropic effects (Kohan et al., 2011; Karppinen et al., 2014).
With chronic altitude exposure, there is enhanced parasympathetic activity, causing a decrease in maximum HR. The change in HR during exercise is also decreased from sea-level values (Boushel et al., 2001). At rest, however, data are conflicting on whether HR is normalized or maintains slightly elevated with acclimatization (Siebenmann and Lundby, 2015).
Very recently, heart rate variability (HRV) has been an area of interest for some studies. A decrease in HRV is a common finding at altitude due to increased sympathetic activity (Karinen et al., 2012). Karinen et al. (2012) suggested that HRV parameters could be used as a predictor of acute mountain sickness (AMS) and found this in their study. Their small sample size, however, meant this finding needed further investigation. Later, a similar study found that HRV indices were not associated with the prediction of AMS (Mairer et al., 2013).
Sex has no effect on the HR response to altitude (Boos et al., 2016a). Older subjects showed less adaptation and a reduced cardiovascular response to altitude, suggesting that age may blunt the increase in HR (Richalet and Lhuissier, 2013). This seems to be compensated for by the respiratory system.
Altitude simulation has recently allowed researchers to look at how different environmental components of altitude, such as hypoxia and hypobaria, affect HR. One such study found that postexercise resting HR was 50% higher in hypobaric hypoxia compared with normobaric hypoxia (DiPasquale et al., 2015). This example shows that both the hypobaric and hypoxic components of the high altitude environment are responsible for our physiological response and not hypoxia alone, raising important questions about the validity of previous experiments that simulated altitude artificially using only hypoxia.
Blood pressure
The changes to blood pressure (BP) during both acute and chronic altitude exposure are well established: first, there is a decrease in systolic BP due to hypoxic vasodilation, which is quickly (within a few hours) counteracted by an increase in sympathetic vasoconstriction, which raises systolic blood pressure (SBP) above sea-level values.
With chronic altitude exposure, systemic hypertension is well documented—even in natives (Mirrakhimov and Windslow, 2011). A recent study showed that diastolic BP did not change between sea level and altitude in mildly hypertensive patients (Lang et al., 2016). Chronic intermittent exposure to altitude has no long-term effect on BP (Vinnikov et al., 2016). The rise in SBP is evident even after only moderate altitude exposure. A trial of 46 healthy people found a rise in 24-hour ambulatory BP was evident even after an exposure to just 2035 m (Torlasco et al., 2015). This level of altitude is easily reachable by those with CVD and so may have important clinical applications (see the Coronary artery disease section). Hypertensives also show an enhanced BP response to exercise at altitude (Lang et al., 2016).
This systemic vasoconstriction is vital to maintain arterial O2 concentrations (Bender et al., 1988), and although the rise in SBP is linear with plasma noradrenaline concentration (Mirrakhimov and Windslow, 2011) showing the importance of sympathetic activity in this response, similar to HR, simultaneous alpha and beta blockade fails to entirely reverse it, meaning other mechanisms must be at least partially responsible (Bärtsch and Gibb, 2007). Possibilities include compensatory polycythemia, which increases blood volume, and the role of the renin-angiotensin system.
Despite the fact important changes have been observed, the effects of altitude on the renin-angiotensin aldosterone system (RAAS) and the resulting influence on BP are broadly ignored by other studies and reviews. Historic studies on RAAS at altitude have shown an acute decrease in plasma levels of renin, aldosterone, and angiotensin II, but rise to normal levels with acclimatization (Maher et al., 1975; Keynes et al., 1982). The activity of renin and aldosterone also decreases (Keynes et al., 1982). The mechanism for the decrease in these components of RAAS is uncertain since the increase in sympathetic activity seen at altitude coupled with renal artery vasoconstriction would be expected to increase plasma renin levels. Bouissou et al. (1989) showed that beta adrenergic mechanisms were not responsible for this decrease. There are also peculiarities in the levels of angiotensin-converting enzyme (ACE) in this environment; one study showed that peripheral ACE is raised with acute altitude (Kamikomaki and Nishioka, 2004). This is despite multiple historical reports pointing out that transpulmonary ACE activity decreases (Li et al., 2016). The real role of RAAS in BP regulation at altitude is yet to be fully revealed by further study; however, it is known that RAAS inhibition is a practical way to control the rise in BP at altitude, although it may not be as effective as it is at sea level (Parati et al., 2014; Lang et al., 2016). Sympathetic control may be more effective (Bilo et al., 2011).
While some studies attribute changes in RAAS to AMS, little is in fact known about the relationship between AMS and plasma renin activity (Sun et al., 2013). Despite some authors attributing the depression in RAAS to AMS (Bouissou et al., 1989; Li et al., 2016), Sun et al. (2013) found that ACE and renin activities are higher in those with AMS of increasing severity, in a study of 230 participants. Genomic studies have revealed that polymorphisms in components of RAAS are linked to susceptibility to AMS and high altitude pulmonary edema (Stobdan et al., 2011; Srivastava et al., 2012; Sun et al., 2013), offering more evidence for the role that RAAS may play in altitude maladaptation. Srivastava et al. (2012) also point out that their data also suggest ethnic variation in these polymorphisms—particularly between highlanders and lowlanders.
Cardiac output
Cardiac output (CO) is known to increase with acute exposure to altitude to preserve O2 delivery to tissues. Tachycardia is the key reason for this increase in CO (see the Heart rate section), but the role of stroke volume (SV) remains controversial. Although this section aims to review recent available data, for a more thorough review on the subject, the reader is directed to Siebenmann and Lundby (2015).
The part played by SV in CO increase with altitude is debatable, and while Siebenmann and Lundby (2015) state that SV remains unchanged in acute hypoxia, the results from studies on the subject are varied—ranging from a decrease (Sime et al., 1974) to increase in SV (Rao et al., 2015). A limitation shared by many of these studies is small sample size, particularly in studies that failed to show any significant change in SV (Kjaergaard et al., 2006). Very recently, Rao et al. (2015) showed a significant increase in SV with acute exposure to genuine altitude from 64.65 mL at 500 m to 68.09 mL at 3700 m (Fig. 2). This was a study on 139 healthy male volunteers, distinctly the largest sample size of any study to date. They hypothesize that the reason for this increase in SV is likely due to increased venous return due to the enhanced sympathetic activity on vasculature.
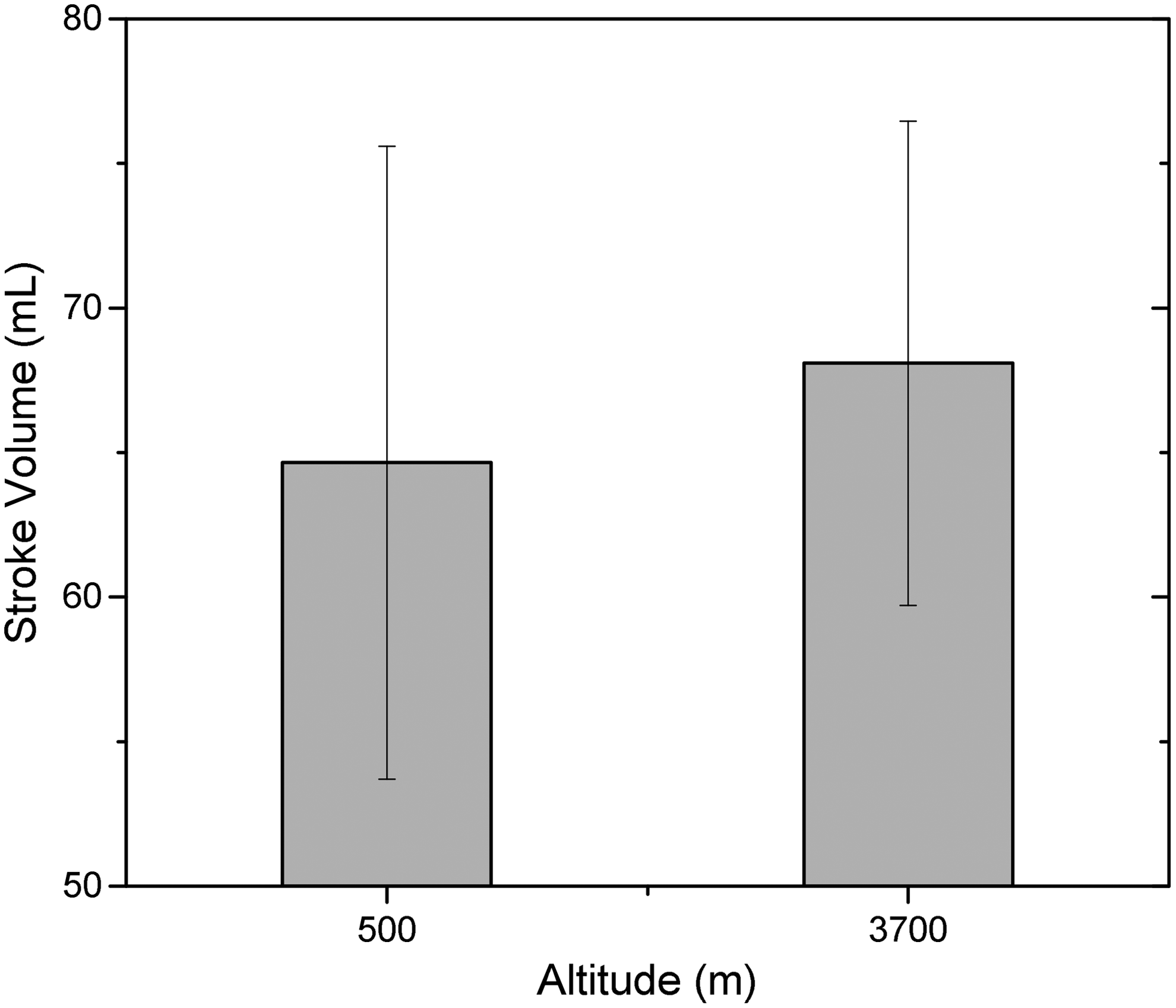
Graph showing the change in SV between 500 and 3700 m in Rao et al. (2015) (n = 139). The error bars indicate 95% ranges in the data. Although many smaller laboratory-based studies and reviews have commented that SV remains largely unchanged (or even decreases) during acute altitude exposure, these data on a large cohort at genuine altitude suggest SV may actually increase. SV, stroke volume.
Following this acute increase in SV, there is a good evidence base for chronic reduction in SV following acclimatization, returning CO to normal physiological levels. While ejection fraction is preserved or increased after time, ruling it out as the cause of SV reduction during acclimatization (Siebenmann and Lundby, 2015), it has been shown that altered filling of the ventricles may be responsible (Stembridge et al., 2016). The reason for this is most likely due to reduced preload, which is due to pulmonary vasoconstriction (Siebenmann and Lundby, 2015). Although there is an increase in blood volume with acclimatization due to polycythemia, which would alter venous return and thus CO, this is counteracted by vascularization of tissues returning venous return to normal levels (Mirrakhimov and Windslow, 2011).
Maximum achievable CO decreases with chronic altitude exposure (Wagner, 2000; Calbet, 2003). The leading theory for this is that muscle function is decreased at altitude, limiting its need for increased blood flow. Another is reduced myocardial function due to hypoxemia. Although this theory has support of in vitro experiments, in vivo experiments have shown that myocardial function is maintained up to 5000 m (Stembridge et al., 2016).
Changes in CO simulated using normobaric hypoxia and hypobaric hypoxia may not be representative of changes in genuine high altitude. Boos et al. (2016b) found that although there is no significant change between these environments and genuine altitude at rest, the differences begin to show following exercise. A previous and similar study found no difference between them even at exercise (Miyagawa et al., 2011). However, Boos et al. (2016b) point out methodological flaws, which call the reliability of their finding into question. This finding by Boos et al. (2016b) offers further support to experiments carried out in genuine altitude, as opposed to in a simulated environment, such as Rao et al. (2015).
Pulmonary circulation
A rise in pulmonary vascular pressure attributed to vasoconstriction is a significant consequence of hypoxia at high altitude. Pulmonary arterial pressure (PAP) increases in a parabolic manner from altitudes of 3000 m, increasing from a mean 15 mmHg at 2000 m to 28 ± 11 mmHg at 4540 m (Penaloza and Arias-Stella, 2007). The increase is subject to a great deal of variability between individuals and shows some genetic influence; studies on the population of Lhasa, Tibet (3658 m), showed a mean PAP of 15 ± 1 mmHg (Groves et al., 1993), close to sea-level values. Penaloza and Arias-Stella (2007) note the population of Lhasa have the oldest altitude ancestry, comparing them with the relatively recent population of Leadville, Colorado (3100 m), which showed abnormally high PAP.
Infants are particularly sensitive to the effects of high altitude, and hyperreaction results in heart failure (HF). This condition, described as subacute mountain sickness, brings about hypertrophy of pulmonary arteries and the right ventricle (Sui et al., 1988).
Typically, pulmonary vasoconstriction causes redistribution of blood to areas of the lung that are better ventilated, improving oxygen saturation. Although this is a useful compensatory mechanism when only a small region of lung is affected, when there is widespread hypoxia throughout the lung, as with altitude, vasoconstriction causes pulmonary hypertension (Swenson, 2013; Sommer et al., 2016). Acute hypoxia closes oxygen-sensitive potassium ion channels in vascular smooth muscle, with subsequent depolarization causing calcium influx and contraction of smooth muscle. Readers are directed to Swenson (2013) for further discussion of the mechanism and ion channel cascades.
Chronic hypoxia brings about remodeling of pulmonary vessels as summarized by Wilkins et al. (2015): enlargement of muscle in distal vessels and the extension of this muscle into normally unmuscularized arterioles. This muscularization of typically amuscular vessels is perhaps one of the most characteristic adaptations to chronic altitude; animal models have shown that this muscularization of alveolar wall vessels may be one of the first remodeling events to occur in chronic hypoxia (Stenmark et al., 2006). Hypoxia compromises the integrity of the endothelial cell membrane, triggering influx of growth factors, which bring about proliferation of smooth muscle cells and thickening of pulmonary arteries (Wang et al., 2014). Additionally, hypoxia also brings about an increase in aldosterone synthesis within pulmonary artery endothelial cells, which may promote vascular remodeling (Maron et al., 2014).
The role of an inflammatory response is also evident in hypoxic pulmonary vasoconstriction (HPV) and is becoming increasingly appreciated. Recent studies have provided evidence for hypoxia and macrophages locking fibroblasts into an activated state through epigenetic mechanisms, which then lead to the release of factors that cause proliferation and growth (Li et al., 2011). Stenmark et al. (2006) outline the evidence for recruitment of leukocytes in acute hypoxia and increase in circulation of monocytes and macrophages. They also note the importance of accumulating fibrocytes, which contribute to the vascular remodeling process through stimulation of angiogenesis and production of collagen promoting fibrosis. A recent review hypothesizes that infiltration of macrophages brings about changes that lead to chronic and unresolving inflammation, which promotes continuous vascular remodeling (Pugliese et al., 2015).
The molecular mechanisms underpinning pulmonary hypertension and remodeling have been the focus of recent studies (Firth et al., 2013; Lai et al., 2015). The signaling complex whereby chronic hypoxia brings about calcium influx was recently investigated, finding that hypoxia increases ET-1-induced responses (Gonzalez Bosc et al., 2016). Hypoxia increases the generation of ROS in the mitochondria of pulmonary vascular smooth muscles, which act as a mediator of intracellular calcium release (Wang and Zheng, 2013). Sommer et al. (2016) summarize that the increase in ROS leads to an increase in resting intracellular calcium; either directly or through interaction with kinases, phospholipase, and calcium and potassium channels. Identification of such factors relevant to pulmonary hypertension would open new avenues for therapeutic targets, although this is disputed by other authors who note that the complexity of the pathways implicated makes targeting single mechanisms for therapeutic intervention difficult (Firth et al., 2013).
Hypoxia stimulates the synthesis of ET-1 in the vascular endothelium, and exposure to high altitudes is associated with greater plasma concentrations of ET-1 (Goerre et al., 1995). ET-1 acts as a potent vasoconstrictor, and excessive release is associated with pulmonary hypertension and pulmonary edema (Sartori et al., 1999). Angiotensin II (see the Blood pressure section) stimulates ET-1 release (Emori et al., 1991) and has also been found to upregulate the ET-1-type A receptor in vascular smooth muscle (Lin et al., 2014), enhancing the vasoconstrictor effect.
Through its interactions with the ETB receptor, ET-1 causes transient vasodilation and hypotension through the release of nitric oxide and prostanoids (Yanagisawa et al., 1988; Kohan et al., 2011), which may be the mechanism behind the fleeting hypoxic hypotension seen on acute exposure to altitude (see the Blood pressure section).
Antagonism of ET-1 receptors may be beneficial in treating HPV (Lüscher and Barton, 2000), stressing the important role of the protein in PAP regulation. Modesti et al. (2006) found that ET-1 antagonists such as bosetan reduced resting PAP after rapid ascent to altitude, supported by findings by Pham et al. (2010) and by Kojonazarov et al. (2012) in highlanders suffering from HPV. Neither Pham et al. (2010) nor Seheult et al. (2009) found a significant reduction in exercising PAP.
The recent review article by Kylhammar and Rådegran (2016) provides an excellent summary on the various pathways surrounding HPV and remodeling, including contemporary research on potential therapeutic targets such as the ET-1 antagonists, stimulators of the nitric oxide pathway, and phosphodiesterase inhibitors.
Native cardiovascular adaptations to altitude
Many native highland populations are exposed to constant hypoxia. With increasing availability of genomic techniques, these populations have been of particular interest to those studying how genetics may affect adaptation to altitude. Several patterns of chronic human adaptation to hypoxia are observed. This section will aim to give a brief outline of them, although more thorough reviews of the subject are available, highlighted throughout.
Populations living at altitude in the Andes display erythrocytosis in addition to high hemoglobin concentrations and oxygen saturation (Beall, 2006). Tibetan populations also show increase in hemoglobin starting at higher altitudes than that of the Andean pattern, although their hemoglobin concentration levels are generally lower. Adaptations of Tibetan natives are instead primarily respiratory rather than hematological, including lower ventilation at rest and more rapid breathing (Beall, 2006), greater HPV responses (see the Pulmonary circulation section), and increased nitric oxide synthesis, with the resulting vasodilation improving oxygen delivery (Beall et al., 2012). Gilbert-Kawai et al. (2014) summarize the adaptation in Himalayan Sherpas and Tibetans in a recent review and should be consulted for further detail to the extent of these changes. Ethiopian highlanders may display a third pattern of adaptation not observed in other populations. Despite exposure to altitudes above 3000 m, hemoglobin concentrations and oxygen saturations do not deviate greatly from healthy populations at sea level (Beall et al., 2002). Further studies have found that Ethiopian populations show little cerebrovascular sensitivity to hypoxia (Claydon et al., 2008).
Genome scans in Andean and Tibetan populations show evidence of selection for genes regulating hypoxia inducible factor (HIF) pathways governing erythrogenesis and angiogenesis to improve oxygen delivery under hypoxia (Ke and Costa, 2006; Bigham et al., 2010). Mutations identified in Tibetans protect them from the polycythemia stopping HIF-mediated erythropoiesis (Lorenzo et al., 2014), while several potential hypoxia tolerance genes have been identified in Ethiopians (Udpa et al., 2014). Polymorphisms in RAAS components have also been shown to have variable consequences for altitude adaptation. The polymorphisms that are protective against maladaptation may possibly be positively selected in highland populations (see the Blood pressure section).
Animal studies have also shown the importance of specific genes in our adaptation to altitude. Knowing the importance that ET-1 plays in altitude adaptation and maladaptation, Stobdan et al. (2015) produced knockout mice lacking the ET-1 receptor type B (ETRB). They found that in these mice, hypoxia is better tolerated: CO is better maintained and contractility and ejection fraction improved. Even oxygen delivery to other vital organs was found to be higher than wild-type mice (Stobdan et al., 2015). Reduced ETRB may therefore have a role in hypoxia tolerance and adaptation. However, these findings require further work to elucidate the function of the receptor in human subjects as well as testing at real rather than simulated altitudes.
CVD and Associated Risks at High Altitude
Hypoxia and other environmental conditions may exacerbate symptoms of CVD or unmask unknown disease. Adverse events occurring far from medical help at altitude may be catastrophic. The following section of this review will highlight the risks associated with altitude for many CVDs.
Coronary artery disease
Few studies on the risks for patients with coronary artery disease (CAD) traveling to high altitude exist. Of those few that have been conducted, even less compare their findings with healthy controls or have an ample sample size. As such, only guidance for patients based on this small amount of data is available, with no concrete recommendations.
Hypoxemia is a major risk to people with CAD traveling to altitude. This, coupled with increased myocardial oxygen demand due to the increase in HR seen with acute altitude exposure (see the Heart rate section), creates a situation whereby myocardial oxygen demand may not be met. This runs the risk of exacerbating symptoms of previously stable CAD or unearthing unknown CAD, as well as the possibility for adverse events, including secondary myocardial infarction. Despite this, many studies have shown that patients with stable CAD have no major increase in risk up to 3500 m (Dehnert and Bärtsch, 2010). However, those patients with stable angina may experience symptoms at lower thresholds at altitude than they usually would at sea level (Dehnert and Bartsch, 2010). One study showed that there is no risk to patients traveling to moderate altitude (3453 m) 6 months postrevascularization for CAD (n = 22) (Schmid et al., 2006). The importance of this particular study is that it potentially demonstrates the safety of altitude in patients following revascularization procedures, including coronary bypass operations. On the other hand, all patients had a normal exercise stress test at sea level before the experiment in this study. This is an important consideration and proviso for anyone with suspected CAD traveling to altitude since it is during exercise when the mismatch between myocardial demand and supply is at its greatest. To overcome this, Dehnert and Bärtsch (2010) recommend that exercise training is started before exposure to altitude for patients with stable angina who are not well accustomed to exercise.
The key difference between those patients with stable angina compared with those with unstable angina at altitude is the risk of adverse events. In particular, adverse events (including unstable angina) do not increase in prevalence at altitude compared with sea level (Dehnert and Bärtsch, 2010), although it is again important to reiterate the data are limited. Compare this with unstable disease, which has not been studied at altitude due to its inherent risk of adverse events even at sea level. The physiology of HR, coronary vasoconstriction, and hypoxemia soundly suggests that it is unsafe for those with unstable angina to travel to altitude, along with those having had a recent myocardial infarction or ventricular fibrillation. Dehnert and Bärtsch (2010) recommend that patients with unstable angina must not travel to altitude.
Exercise capacity is reduced by 1% for every 100 m ascended after 1500 m (Fulco et al., 1998). Healthy individuals have enough functional reserve to overcome this, although this functional reserve is reduced with age (Levine, 2015). This, coupled with the recent finding that diseased coronary arteries paradoxically constrict during exercise and stress (Arbab-Zadeh et al., 2009) due to coronary spasm and respiratory alkalosis (Rimoldi et al., 2010), raises important concerns for (particularly elderly) patients with CAD who may be somewhat exerting themselves at altitude. Again, despite this, studies have shown little difference in reduction in exercise capacity between patients with CAD and healthy controls, and adverse events are rarely reported. A study of eight patients with previous history of myocardial infarction found no significant difference between loss of exercise capacity with altitude (4200 m) compared with seven healthy controls (de Vries et al., 2010). Roach et al. (1995) did find ischemia-like ECG changes in 40% of its sample of elderly people exerted at 2500 m, although there were no adverse events reported.
Historically, it has been known that ischemia-like changes on ECG have occurred at altitude for some time since the work of Levy et al. (1939), who found these ECG changes in patients symptomatic for CAD when breathing an FIO2 of 10%—equivalent to around 5000 m altitude (Levine, 2015)—for just 5 minutes. Thankfully, the use of this uncomfortable test in these patients is unnecessary nowadays with availability of stress testing and improved imaging; however, Levy's findings do demonstrate the possibility of ischemia in this cohort in a low-oxygen environment.
De Vries et al. (2010) also highlight the importance of acclimatization in this cohort of patients. All their patients were acclimatized well to their environment for 10 days. Acclimatization is an important step in minimizing risk in this cohort. Although risk of adverse events is minimal, a retrospective cohort study found that one night of acclimatization at an altitude of 1300 m may reduce adverse events by a factor of 5.7 (95% confidence interval 2.8–11.6) (Lo et al., 2013; Levine, 2015).
All these available data suggest that ascents to 3500 m or less pose no significant risk to fit patients with stable well-controlled CAD. Higher altitudes, however, contribute significant risk even to seemingly healthy patients who may be at risk of CAD. Vizzardi et al. (2015) discussed the case of a seemingly fit 60-year-old professional climber who became dyspneic at 5500 m, later revealing a stenosed coronary artery. Following revascularization, the patient was asymptomatic and showed no ECG changes up to 2800 m, adding support to Schmid et al. (2006).
There is not enough evidence for definitive recommendations to be made for patients with CAD wanting to travel to high altitude. Some authors have, however, made suggestions: generally for patients with stable disease, on optimal medication, and who have a good exercise tolerance, travel to altitudes of <3500 m is thought to have no significant risk from the data available (Dehnert and Bärtsch, 2010). It is, however, impossible to define a safe altitude under which it is entirely safe for this group (Bonadei et al., 2016). It may be recommended that elderly patients with CAD or a past history of an adverse event should undergo exercise stress testing at sea level (Levine, 2015). Acclimatization is highly recommended before any physical exertion to reduce risk of adverse events (Lo et al., 2013; Levine, 2015). Travel to higher altitudes should be avoided (Dehnert and Bärtsch, 2010), but for those who choose to, Vizzardi et al. (2015) recommend examination at a specialist center, including nonstandard tests such as a hypoxic exercise stress testing.
Heart failure
The safety of traveling to altitude with HF is largely undefined. Very few studies on the effects of altitude on HF have been conducted, and even fewer have taken part in genuine altitude. It is not only the disease itself that is a cause for concern when patients are exposed to altitude but also the comorbidities many patients with HF may suffer from. Agostoni (2013) highlights that the common comorbidities of COPD, anemia, and pulmonary hypertension (see the Pulmonary circulation section); all have safety concerns at altitude.
Nevertheless, Agostoni (2013) concludes that spending time at altitudes of <3500 m is safe for patients with stable HF. This is a conclusion corroborated by the few other studies found on the subject. One recent study of 29 stable HF patients found that an altitude of 3454 m was tolerated well, even during exercise (Schmid et al., 2015). However, some patients did become susceptible to tachyarrhythmias during this experiment, prompting additional research into the field. It is worth noting that patients with COPD were also excluded from this study.
For patients with symptomatic HF, Mieske et al. (2010) comment that exposure to high altitude is contradicted. This is because they often decompensate due to fluid retention relating to AMS.
HF patients can, however, expect a substantial decrease in their exercise capacity at altitude, more so than healthy subjects. This reduction is worst in people with the most severe HF (Agostoni et al., 2000). In their controlled experiment (14 healthy controls, 38 HF patients, all without primary lung disease), Agostoni et al. (2000) found that exercise capacity decreased 3% ± 4% per 1000 m in their control groups, but by 5% ± 3% (p < 0.01) in patients with HF with normal workload. This decrease was even more dramatic in HF patients with markedly reduced workload who suffered a decrease of 11% ± 5%. This study, however, only used hypoxia to simulate altitude. As discussed in the Cardiac output section, this is not representative of genuine high altitude. In fact, in a comment on this article, Kraus (2000) points out many shortcomings of this experiment, suggesting that many typical changes at genuine altitude, especially increase in circulating catecholamines (see Heart rate section), may have detrimental effects on HF. Since this study did not use genuine altitude, it may not have reliable data.
Interestingly, there has been some evidence to suggest that intermittent simulated altitude may improve HF patients' exercise capacity, skeletal muscle strength, and quality of life (Saeed et al., 2012). In their study involving 12 HF patients, Saeed et al. (2012) showed a significant increase in all these parameters after 10 sessions of simulated altitude up to 2700 m over 22 days.
Not enough data exist to make firm recommendations about patients with HF traveling to high altitude, especially those with comorbidities such as COPD, since these patients are excluded from all studies. Agostoni (2013) suggests it is safe for those with stable disease and without comorbidities to travel to altitudes of <3500 m, but highlights how optimal medical therapy at sea level is likely different to that at altitude, particularly with regard to beta blockers, where elective drugs may be preferred. For more information on medical management, the reader is redirected to Agostoni (2013).
Arrhythmias and sudden cardiac death
Despite their symptoms being reported by visitors to high altitude for many years, it is only recently with the perfection of ambulatory monitoring that arrhythmias at high altitude have been properly studied. Although studies have shown that acute exposure to altitude is arrhythmogenic, these arrhythmias are largely benign in the healthy populations studied. Nevertheless, sudden cardiac death (SCD) remains a leading cause of death at altitude; responsible for 30% of deaths in hikers and 52% in downhill skiers (Windsor et al., 2009). Components of the high altitude environment may predispose to arrhythmias, many discussed in the earlier section of this review. In particular, hypoxia, respiratory alkalosis, and electrolyte imbalances are some of these.
Historic studies in healthy people frequently showed an increase in HR (see the Heart rate section), right-axis deviation, and accentuated sinus arrhythmia with acute altitude exposure (Woods et al., 2011). More recent studies using ambulatory monitoring have shown similar results, particularly during exercise. One study using subcutaneous loop monitors showed increased incidence of ventricular ectopics and one incidence of asymptomatic atrial flutter during exercise at 4500 m (Woods et al., 2008). Although this was a study in only nine healthy male volunteers, it was very revealing—showing that the cardiac workload brought on by altitude is arrhythmogenic. The benign nature of the arrhythmias recorded by Woods et al. (2008) supports other similar conclusions. Particularly, it supports that of Operation Everest II, which concluded that extreme altitude (8848 m) is not associated with significant arrhythmia or ischemia (Malconian et al., 1990). Operation Everest II did, however, use simulated altitude, which as explained in other parts of this review has shortcomings. A more recent study using genuine high altitude in the Andes has shown that in a population (n = 33) of varying age, high altitude favors arrhythmogenesis (Behn et al., 2014). Although this was the case in all age groups, it was most pronounced in the younger age group. Arrhythmias were most common upon rapid descents in altitude, which may partially explain the high number of deaths caused by SCD in downhill skiing.
Although available studies have shown that altitude is unlikely to cause a malignant arrhythmia, all these have been on a healthy test population. It does, however, remain a fact that SCD, usually predisposed by a malignant ventricular arrhythmia, is an important cause of death in those traveling to altitude, particularly the elderly. Even moderate altitude between 1100 and 2100 m is thought to be a risk factor for SCD (Burtscher et al., 1993), with mountain hiking increasing the risk of SCD by 4.3 in men over 34 years of age (Windsor et al., 2009). Although it is impossible to carry out large studies on the effects of altitude on SCD in those most at risk, recommendations can be made based on prior knowledge. Windsor et al. (2011) discussed how conditions of the high altitude environment such as hypoxia, hypothermia, and electrolyte imbalances may coincide with an increase in QT interval. These along with the associated weight loss and infection risk of high altitude activities may be an underlying cause of fatal arrhythmia and SCD at altitude. Although unlikely to be a risk to the healthy individual, these factors may unmask unknown long QT syndrome (LQTS), a condition known to increase episodes of ventricular arrhythmia and SCD.
Although no studies into the cause of SCD at altitude have been conducted, retrospective studies have highlighted important risk factors, namely previous MI, CAD, diabetes, hypercholesterolemia, and hypertension. Additionally, those who do not regularly undertake activities at high altitude are also at greater risk (Burtscher, 2007; Burtscher et al., 2007).
While it is impossible to make recommendations to those with acquired LQTS due to the sparsity of evidence and variable presentation of the disease, the authors of Windsor et al. (2011) recommend that those with known congenital LQTS must not travel to altitudes exceeding 2500 m. They also note that the unspecific symptoms of syncope, dizziness, and palpitations in patients wishing to travel to high altitude should not be ignored since to prevent episodes of SCD, it is first vital to identify those with LQTS. For more information on the management of LQTS and those at risk of SCD at altitude, including medical therapy, the reader is redirected to Windsor et al. (2011).
Hypertension
The increase in BP associated with ascent to altitude (see the Blood pressure section) may be of concern to patients suffering from hypertension. As with healthy individuals, it has been demonstrated that hypertensive patients suffer a moderate increase in BP with exposure to altitude (Luks, 2009). In one study, systemic BP in mild hypertensives (n = 42) rose from 154 ± 18 to 168 ± 17 mmHG, a slightly higher increase than normotensives in the same study (Wu et al., 2007). Hypertensives also show an accentuated increase in BP during exercise at altitude compared with their healthy counterparts (Lang et al., 2016). There is, however, great variability in BP response to altitude within individuals.
Although it is known that there is an increase in BP with altitude and that hypertension is a risk factor for many adverse cardiovascular events at altitude, including SCD (Burtscher, 2007), there is little evidence to suggest that exposure to altitude causes any increase in the risk to patients with hypertension (Luks, 2009; Mieske et al., 2010). Indeed, very few studies show any increase in adverse events in patients with hypertension, compared with controls at altitude (Wu et al., 2007; Luks, 2009). As such, moderate hypertension is not believed to be a contraindication to high altitude travel.
Despite this reassuring evidence, there has been no study at altitude in patients with severe hypertension. Wu et al. (2007) excluded workers with severe hypertension from their study, and therefore it is impossible to make recommendations on patients with severe disease. Similarly, since variation in BP response to altitude is great, even moderate hypertensives are recommended to monitor their own BP during stays at altitude (Luks, 2009). A lot more needs to be done to comfortably address the individual variability in BP response.
Along with monitoring their own BP at altitude, Luks (2009) states that it is not necessary for patients with stable disease to change their medication while at altitude, although change, starting with an increase in existing medications, may be useful for individuals who experience a particularly large increase in BP at altitude. Luks (2009) also states that should additional medications be required, alpha-blockers and calcium channel blockers have sound physiological backing. Recently, experimental evidence has backed up this claim, showing the efficacy of nifedipine (an alpha blocker) coupled with telmisartan at reducing BP in hypertensives at altitudes of 3300 m (Bilo et al., 2015).
Despite these satisfying conclusions, further study is needed to uncover populations at risk of hypertension and particularly its complications at altitude.
Approaching patients with CVD
Considering the very limited guidance on managing CVDs at altitude, it is hard to draw firm management plans for patients who wish to travel to altitude. Since the reason for travel is often due to work or leisure, it often contributes a major factor toward quality of life, meaning it is important to emphasize the importance of shared decision-making between patient and physician when advising patients on the subject. This is especially poignant in patients with well-established and controlled disease.
Although it is obviously wise to deter patients with unstable disease (including moderate–severe HF, unstable angina, and LQTS) from traveling to high altitudes, for patients with stable disease, it may be more appropriate to inform and advise them on the effects altitude may have on them and how they can alter their trip to minimize risks. Ways this can be done include prealtitude screening tests, self-monitoring while at altitude, allowing time for acclimatization, and possibly some modification in medical therapy. In particular, it is important to warn patients with HF that they will experience a decrease in functional capacity as they ascend.
As discussed earlier, there is much evidence for the effectiveness of using acclimatization for reduction of risk in this cohort of patients (DeVries et al., 2010; Lo et al., 2013). It should be advised to all patients with CVD wishing to travel to altitude to alter their ascent profile to allow for acclimatization or to include at least one night at a more intermediate altitude if they are traveling to altitude by transport. Just one night's acclimatization may reduce adverse events by a factor of 5.7 (Levine, 2015).
The use of prealtitude screening is also recommended by some authors (Vizzardi et al., 2015) as a way to uncover unknown disease in a controlled environment and to assess exercise tolerance. Evaluation is a good thing to consider if available, especially if there is any concern on behalf of patient or physician. However, altitude simulation is sparsely available, expensive, and somewhat unreliable; meaning that exercise tolerance measures could be used to offer an affordable approximation of how patients may cope with the increased physiological demand of altitude. In addition to this, self-monitoring of BP is vital for all those with CVD traveling to altitude. This should be more rigorous than usual, especially during the first few days of exposure, and a log should be kept. This is due to the variability of BP at altitude as well as the implications of an increasing BP in this cohort. Stark rises in BP may be an implication for increasing medical therapy in hypertensives (Luks, 2009).
To summarize, although the physician can warn of the risks to a patient at high altitude, a shared decision-making approach in which the patient is informed of relevant risks is wholly preferable. Simple management options such as encouraging self-monitoring of BP, spending time to acclimatize, and prior monitoring may not only decrease risk of adverse events in this cohort of patients but will also address any concerns the patients may have.
Going Forward
Although our understanding of how altitude affects human cardiovascular physiology is well rounded, further insight is needed into the precise biochemical mechanisms that govern these. Elucidating these mechanisms may uncover novel ways of avoiding consequences of these adaptations to those they may affect. In addition, with the recent realization that simulated altitude does not paint a full picture when studying physiology, more study is needed to confirm and build upon findings found using these techniques.
Given how little is known about clinical aspects of CVD at altitude, it is now time to start studying it in depth. Future studies should focus their efforts on how genuine high altitude is tolerated by patients with hypertension, stable angina, and mild–moderate HF. It should be emphasized here again that these future studies should use genuine altitude exposure in their investigations, with an emphasis also on large patient cohorts, as these are two areas of weakness in almost all studies in this area to date.
Work by Boos et al. (2016b) investigates the difference in response to different forms of hypoxia. Similar studies should be conducted in larger cohorts to draw robust conclusions to varying responses. From this, previous studies using simulated hypoxia may be reevaluated. With a richer understanding of its shortcomings, future simulated altitude studies on larger cohorts can be interpreted with informed caution.
Despite the shortcomings of simulation in respect to understanding physiology, it does have a strong place in this field. In particular, the findings of Saeed et al. (2012)—intermittent sessions of simulated altitude may have a positive impact on HF patients' quality of life—need further investigation. Its results have not yet been reproduced, and more robust studies containing control groups and larger cohorts are needed. If their findings are reinforced with further study, it could have profound effects on the treatment of HF. What is more is that optimizing medical therapy in patients with HF also requires investigation in genuine altitude. Agostoni (2013) lays out the physiological background and current evidence for using selective beta blockers over nonselective drugs at altitude, however, notes in this article that this has never been investigated in long stays at altitude. Evidence that these selective drugs are better tolerated is needed since as evidence stands, it may not be wholly justified to interrupt management of patients who are stable and tolerating their current treatment.
With more people choosing to travel to altitude, an emphasis should be placed on how common disease, such a CVDs, may be affected. There are large gaps in our knowledge on how the most at-risk groups are affected by altitude and, with them, large gaps in how to manage them. Although some firm recommendations can be drawn from what we already know, complete minimization of risk and fatality to those traveling to altitude with CVD will only come with further research.
Footnotes
Author Disclosure Statement
No competing financial interests exist.