
Abstract
Abstract
Willmann, Gabriel, Kai Schommer, Maximilian Schultheiss, M. Dominik Fischer, Karl-Ulrich Bartz-Schmidt, Florian Gekeler, and Andreas Schatz. Effect of high altitude exposure on intraocular pressure using Goldmann applanation tonometry. High Alt Med Biol. 18:114–120, 2017.
Aims:
The aim of the study was to quantify changes of intraocular pressure (IOP) during exposure to 4559 m using the state-of-the-art method of Goldmann applanation tonometry for IOP measurement and to detect correlations between IOP and acute mountain sickness (AMS) in a prospective manner.
Methods:
IOP was measured using a Goldmann applanation tonometer AT 900® (Haag-Streit, Switzerland) and central corneal thickness (CCT) with the anterior segment module of a Spectralis™ HRA+OCT® device (Heidelberg Engineering, Germany) at baseline and high altitude. Assessment of AMS was performed using the Lake Louise and AMS-C questionnaires, and Pearson's correlation coefficient was calculated for association between IOP and AMS.
Results:
Raw IOP values at high altitude were not significantly changed compared to baseline. IOP adjusted to the increase in CCT at high altitude, which is known to alter IOP levels, showed a significant reduction for corrected IOP values on day 3 of exposure (morning −2.1 ± 1.2 mmHg; evening −2.3 ± 1.1 mmHg; p < 0.05). No correlation of IOP with AMS or clinical parameters (heart rate and SpO2) at high altitude was noted.
Conclusions:
IOP showed a significant reduction of IOP levels when corrected for increased CCT values at high altitude. Furthermore, the prospective measurement of IOP is not useful in diagnosing AMS or for the prediction of more severe high altitude related illnesses as the decrease in IOP and symptoms of AMS do not correlate during altitude exposure.
Introduction
H
Intracranial and intraocular pressure (IOP) are positively correlated (Lashutka et al., 2004; Sajjadi et al., 2006; Morgan et al., 2016). Because the measurement of IOP is noninvasive and thus applicable even in remote areas, this method for the detection of subjects at risk for severe high altitude illnesses has become of particular interest (Bosch et al., 2010b; Cushing et al., 2013). However, the outcome of existing studies investigating IOP at high altitude remains controversial as some studies suggest an increase and others a decrease of IOP during high altitude exposure (Cymerman et al., 2000; Ersanli et al., 2006; Pavlidis et al., 2006; Somner et al., 2007; Bosch et al., 2010b; Karakucuk et al., 2012; Cushing et al., 2013). The divergent results may, in part, be explained by different approaches of IOP measurement procedures, different duration of high altitude exposure, or various degree of high altitude hypoxia at which IOP was studied. The aim of the present study was to quantify changes of IOP during a 4-day stay after acute exposure to an altitude of 4559 m. For the first time in high altitude research the gold standard method for IOP measurement, the Goldmann applanation tonometry, was used and IOP values were corrected for the amount of corneal edema formation before correlation between IOP and AMS was assessed.
Materials and Methods
Study design
Fourteen healthy subjects (mean age 36 ± 9 years; range 25–54 years) volunteered to participate in this prospective field study. All subjects were sea-level residents and had no altitude exposure above 2000 m within two weeks before high altitude exposure. All subjects were healthy and had no eye diseases. At 341 m above sea level (Tübingen, Germany), all baseline examinations were performed (BL1 and BL2). Subjects ascended on foot accompanied by a mountain guide within 24 hours from Gressoney (1635 m, Italy) to the Capanna Regina Margherita (CM; 4559 m, Italy), including passive transportation by cable car from Gressoney to Punta Indren (3260 m) and an overnight stay at the Capanna Gnifetti (3647 m, Fig. 1). Subjects spent three nights at the CM and descended on the fourth day in the morning (Fig. 1). Throughout the study period, subjects were not allowed to have intake of caffeine and alcohol. High altitude headache was treated with ibuprofen 600 mg and nausea with metoclopramide 10 mg orally on demand, but none of the subjects were treated with acetazolamide. Metoclopramide was only used in two subjects 1 × 10 mg in the morning after arrival, and a detailed overview on the intake of ibuprofen is shown in Table 1. Written consent was obtained from the subjects, and the study was performed in accordance with the tenets of the Declaration of Helsinki 1975 (1983 revision) and was approved by the local IRB (Ethik-Kommission der Medizinischen Fakultät und am Universitätsklinikum Tübingen, IEC project number: 258/010B01).
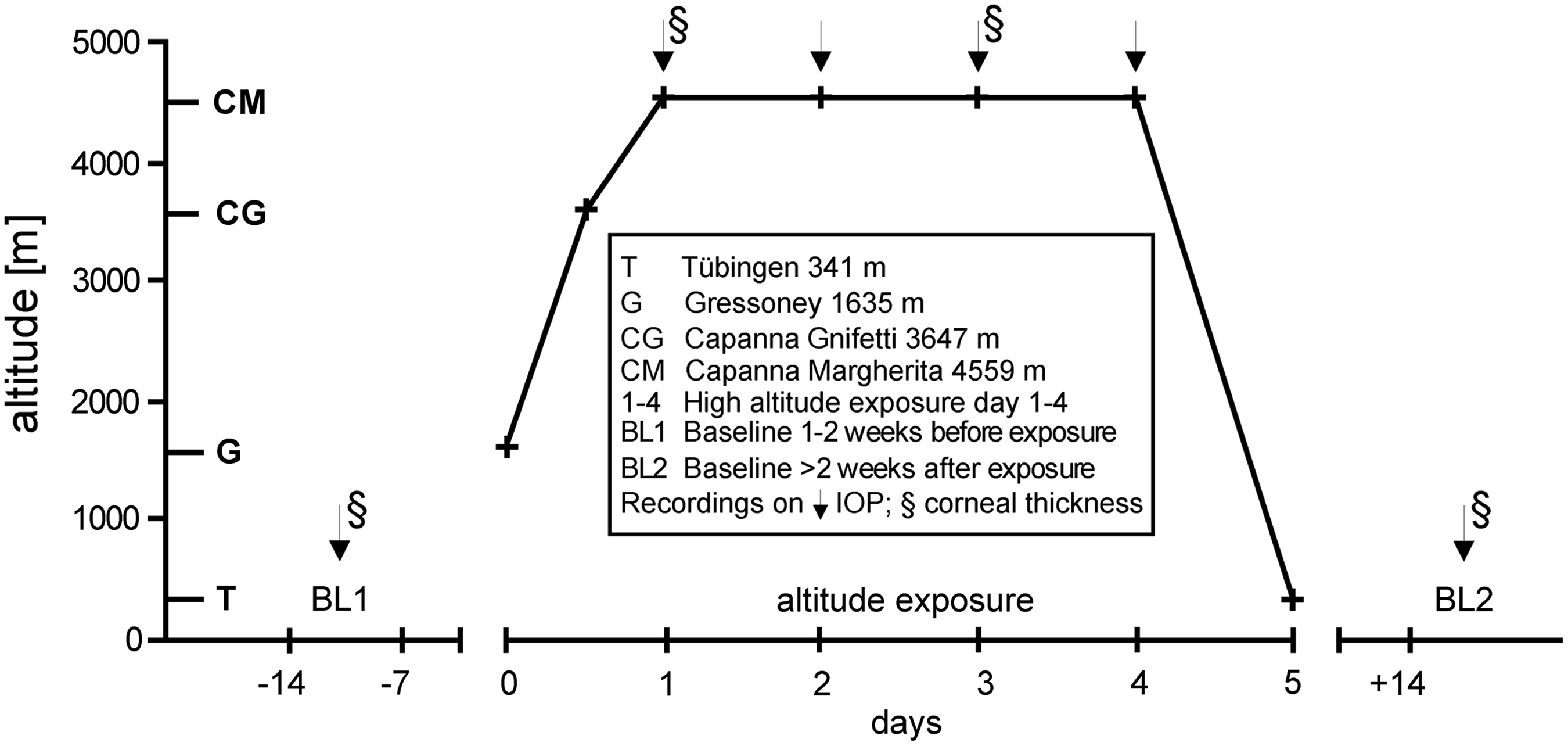
Ascent profile to the Capanna Margherita (4559 m). Baseline examinations were performed at Tübingen (341 m; Germany) 7–14 days before and at least 14 days after ascent to high altitude. At high altitude, examinations were performed for 4 days (1–4). All IOP measurements (arrow) and examinations of central corneal thickness (§) are marked. IOP, intraocular pressure.
Amount of ibuprofen intake for each subject at high altitude for all 4 days. While six subjects did not need any medication, one subject used up to 3000 mg of ibuprofen; −, healthy subjects; +, subjects suffering from AMS (acute mountain sickness).
Examinations
Baseline IOP measurements were performed within 2 weeks before and again at least 2 weeks after the field study in the morning (Fig. 1), and were repeated during the field study at the CM twice daily (morning and evening; day 1–4). Central corneal thickness (CCT) was measured at both baseline examinations (before and after exposure to high altitude) and on day 1 and 3 at the CM in the morning (Fig. 1) (Willmann et al., 2013). Due to logistical difficulties at the evening of day 1, IOP was observed in only 9 and CCT in only 8 of 14 volunteers. Clinical assessment of AMS and of vital parameters was performed twice daily (morning at 07:00am and evening at 08:00pm) after >5 minutes' rest during the stay at the CM.
Ophthalmological examinations
A Goldmann applanation tonometer installed on a slit lamp (Haag-Streit BP 900®, Haag-Streit, Köniz, Switzerland) was used for IOP measurements. The tonometer was calibrated once at baseline and high altitude using a standard calibration bar (Haag-Streit, Switzerland). Three IOP measurements were averaged for every subject and time point. Corneal anesthesia was achieved by applying one drop of Conjucain EDO® (Bausch & Lomb GmbH, Berlin, Germany) 2 minutes before the first IOP measurement. Immediately after corneal anesthesia a drop of Fluorescein SE Thilo® (Alcon Pharma, Freiburg, Germany) was applied for tear film staining. Observation of CCT was obtained using two identical Spectralis™ HRA+OCT® devices (Heidelberg Engineering, Heidelberg, Germany) and a prototype anterior segment lens provided by the manufacturer as previously described (Willmann et al., 2013). For evaluation of CCT 9 high-resolution line, scans of the central cornea were averaged for one recording.
Adjusting IOP for CCT at high altitude
It is well documented that values of IOP obtained with the Goldmann applanation tonometer are affected by CCT, corneal curvature, and axial length (Whitacre and Stein, 1993; Whitacre et al., 1993). Therefore IOP values measured were adjusted according to the “Dresdner correction table” with the use of the equation ΔIOP = (−0.0423 × CCT) +23.28 as described in detail by Kohlhaas et al. (2006). In addition, the Ehlers and Whitacre models were used to compare variability between CCT correction models (Ehlers et al., 1975; Whitacre et al., 1993).
Clinical assessment
Oxygen saturation (SpO2) and heart rate (HR) were measured by a finger pulse oximeter (oxy control 4c®, Geratherm Medical AG, Geschwenda, Germany). AMS was assessed by the Lake Louise (LL) and the AMS-C subscore of the Environmental Symptom Questionnaire (Sampson et al., 1983; Roach et al., 1993). The LL score consisted of the self-report questionnaire and a clinical examination. For the self-report questionnaire, each participant answered questions about the severity of headache, gastrointestinal symptoms, fatigue, light-headedness or dizziness, and insomnia. A score of 0–3 points (0 = no symptoms, 1 = mild symptoms, 2 = moderate symptoms, and 3 = severe symptoms) was assigned for each question. In the clinical examination, a score of 0 (normal) to 4 points was given for mental status (for which 4 points indicated coma) and ataxia (for which 4 points indicated inability to stand on the heel-to-toe walking test). The sum of all points yielded the LL score.
The AMS-C score of the Environmental Symptom Questionnaire consists of 11 items, which are graded from 0 (absent) to 5 (extremely severe). The factorial weight of each item is given in parentheses: light-headed (0.489), headache (0.465), dizziness (0.446), feeling faint (0.346), dim vision (0.501), off-coordination (0.519), feeling weak (0.387), sick to stomach (0.347), loss of appetite (0.413), feeling sick (0.692), and feeling hung-over (0.584). To obtain the AMS-C score, the sum of all item scores multiplied by the respective factorial weight was multiplied by 5 and divided by 25.95 (Sampson et al., 1983). Subjects were considered to have AMS, when the LL score was ≥5 in the presence of headache and the AMS-C score was ≥0.70. The clinical parameters (HR and SpO2) were measured immediately before assessing AMS scores (AMS-C and LL).
Statistics
All statistical analysis was performed using JMP® (Version 8.0.2, SAS Institute, Cary, Canada). Normal distribution was ensured using Shapiro–Wilk test (p = 0.05). Baseline examinations (BL1 and BL2) were compared using dependent t-test (p = 0.05). Both eyes were assessed for IOP, but no significant difference between both eyes was found (p > 0.05). Thus, results of right eyes were used for calculation of intraindividual differences between baseline (BL1) and follow-up examinations (follow-up–BL1). Data are shown as mean and 95% confidence interval for each time point. Intraindividual differences were compared by multivariate analysis of variance for repeated measures (MANOVA; p = 0.05). Pearson's correlation coefficient (significance level p < 0.05) was calculated to evaluate a possible correlation between IOP and clinical parameters (SpO2, HR) and LL, as well as AMS-C, on day 1 during high altitude exposure.
Results
Clinical assessment and AMS scores
Incidence of AMS (LL ≥5 and AMS-C ≥0.7) was 50% (n = 7/14) the morning after arrival at high altitude. Clinical parameters of peripheral oxygen saturation were significantly decreased and HR significantly increased on all days spent at high altitude compared to baseline recordings. An overview of all clinical data and AMS scores is summarized in Table 2.
Numbers displayed are mean ± SD. SPO2, oxygen saturation measured by pulsoximetry; HF/min, heart rate per minute; LL, Lake Louis; AMS-C, score for assessment of AMS. BL1 is the baseline examination before exposure to high altitude, 1–4 days at high altitude, and BL2 is the examination after high altitude exposure.
Raw IOP measurements
Assessment of IOP before and after ascent to high altitude was not significantly different with values at BL1 of 11.7 ± 1.1 mmHg (mean ±95% confidence interval) and BL2 of 11.3 ± 1.1 mmHg (p = 0.47). Longitudinal intraindividual differences of raw IOP to baseline (Fig. 2) showed a nonsignificant reduction of IOP at high altitude (day 1 morning 0.0 ± 1.1 mmHg; day 1 evening −0.4 ± 1.4 mmHg; day 2 morning −0.6 ± 1.1 mmHg; day 2 evening −0.9 ± 1.1 mmHg; day 3 morning −0.9 ± 1.1 mmHg; day 3 evening −1.1 ± 1.1 mmHg; day 4 morning −0.8 ± 1.1 mmHg; p > 0.05).
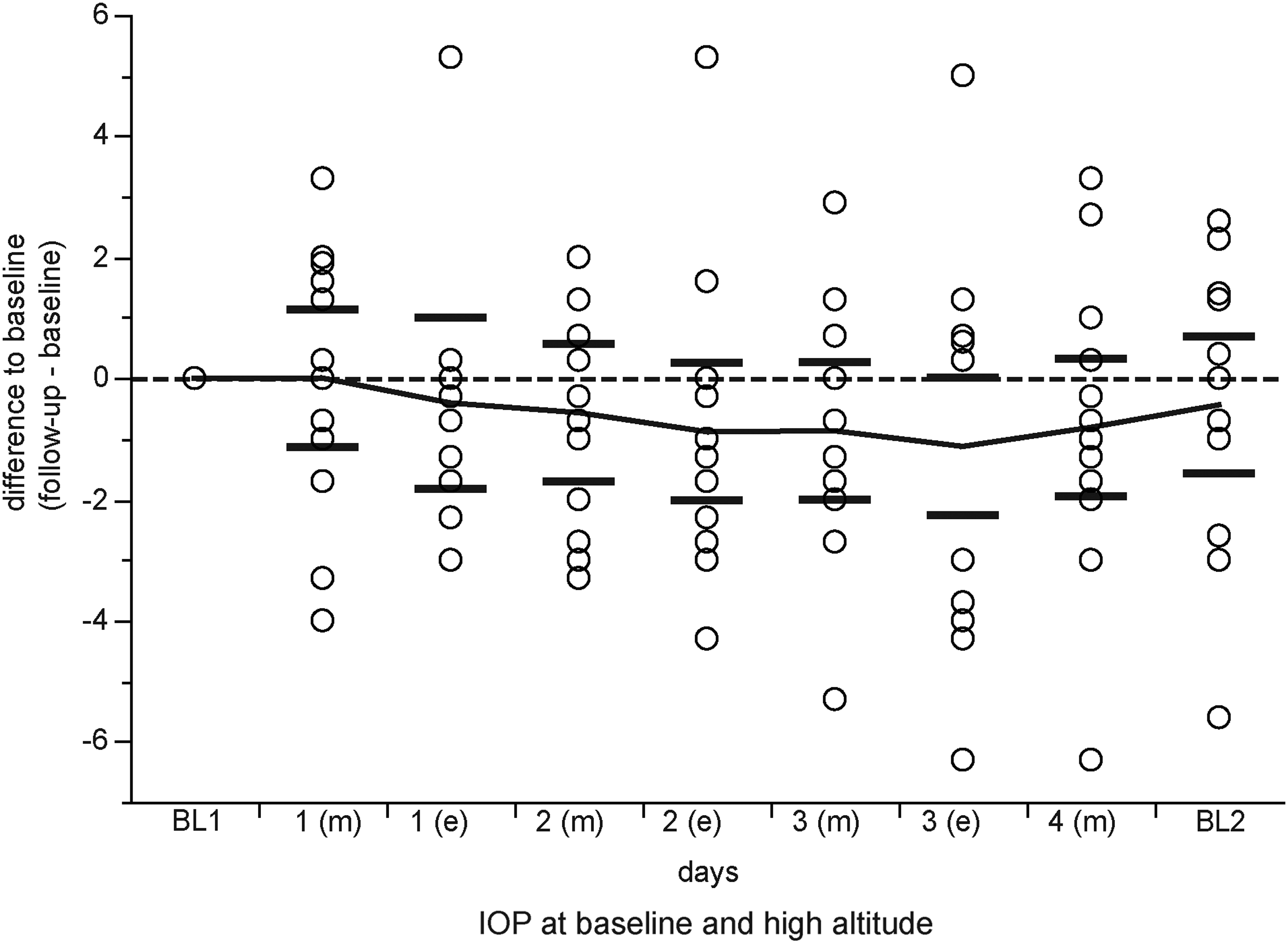
Results of raw IOP measurements at baseline (BL1), during high altitude exposure (day 1–4), and after high altitude exposure (BL2) with means (illustrated as connected line) and 95% confidence intervals (whiskers) for examinations at morning (m) and evening (e). No significant differences were observed during high altitude exposure.
CCT measurements
Both baseline examinations, before and after ascent to high altitude, revealed no statistically significant differences (BL1 515.4 ± 18.1 μm and BL2 515 ± 17.4 μm). Compared to baseline, a significant increase of CCT was found at high altitude on both days tested: day 1 (535.8 ± 17.5 μm; p < 0.05) and day 3 (524.9 ± 19 μm; p < 0.05).
IOP measurements adjusted to CCT
The comparison of IOP levels adjusted to CCT before and after ascent to high altitude revealed no significant differences (BL1 13.2 ± 1.2 mmHg; BL2 12.8 ± 0.9 mmHg; p = 0.45). At high altitude, the intraindividual differences to baseline (Fig. 3) showed a nonsignificant reduction on day 1 (morning −0.9 ± 1.1 mmHg; evening −1.4 ± 1.4 mmHg; p > 0.05). However, a significant reduction of IOP values adjusted to the increased CCT at high altitude (Fig. 3) was observed on day 3 (morning −2.1 ± 1.2 mmHg; evening −2.3 ± 1.1 mmHg; p < 0.05). When using other commonly used correction formulas of Ehlers (day 1 morning −1.5 ± 1.1 mmHg, evening −2.1 ± 1.4 mmHg, p < 0.05; day 3 morning −2.9 ± 1.9 mmHg, evening −3.1 ± 2.1 mmHg, p < 0.05) or Whitacre (day 1 morning −0.4 ± 1.8 mmHg, evening −0.9 ± 2.1 mmHg, p > 0.05; day 3 morning −1.5 ± 1.6 mmHg, evening −1.7 ± 1.5 mmHg, p < 0.05), similar results with a significant reduction of IOP after correction for CCT at high altitude were noted.
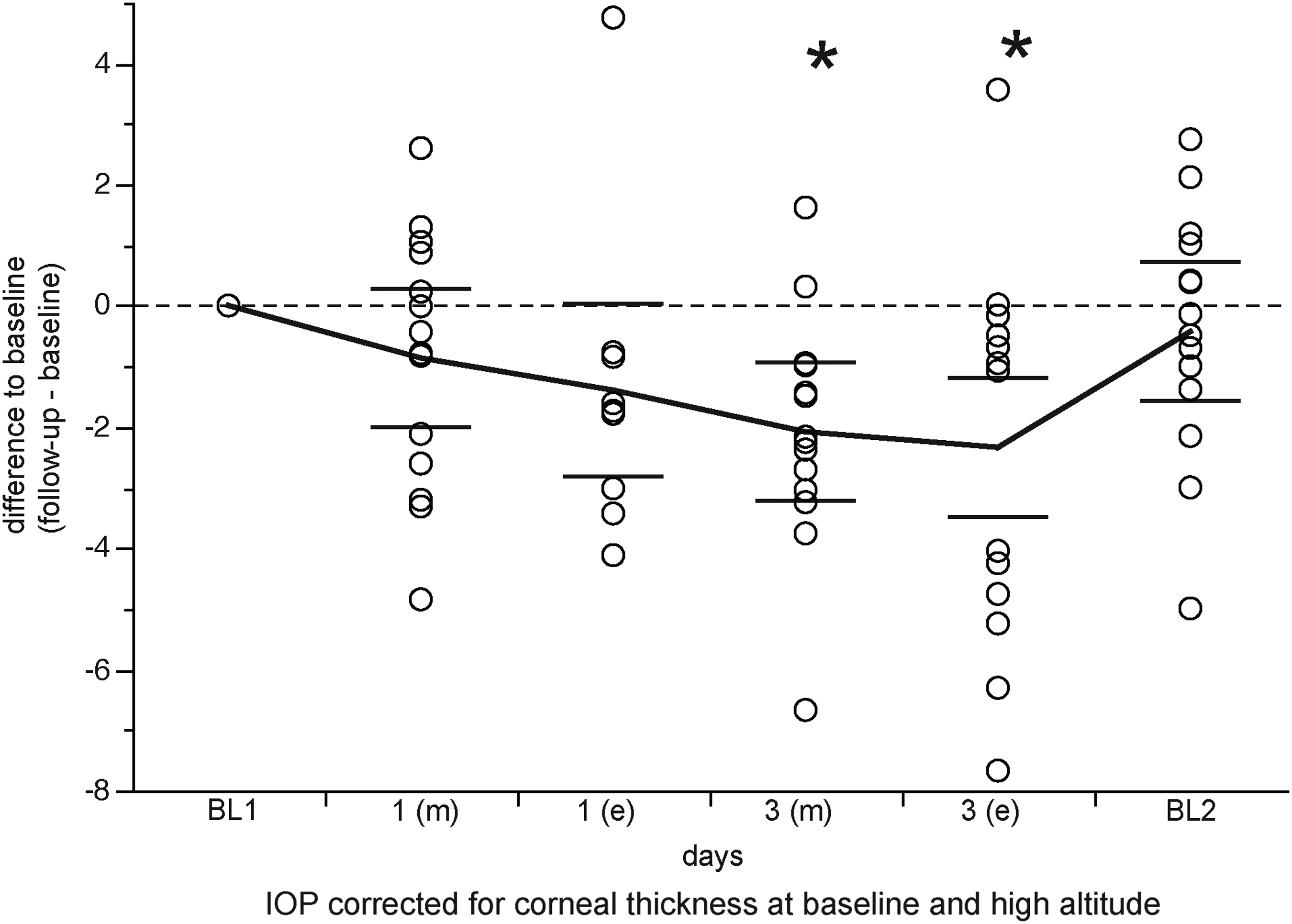
Illustration of IOP measurements adapted to central corneal thickness at baseline (BL1), during high altitude exposure (day 1–3), and after high altitude exposure (BL2) with means (illustrated as connected line) and 95% confidence intervals (whiskers) for examinations at morning (m) and evening (e). Significant differences are marked by stars (*p < 0.05).
Correlations of IOP with scores of AMS and clinical parameters
An association between raw IOP measurements and LL, AMS-C, or clinical parameters (HR and SpO2) was not observed. All calculations of correlation revealed no significant results (P 0.06–0.95; r − 0.52 to 0.36). After adjusting IOP levels to CCT values, the assessment of respective correlations with LL, AMS-C, and clinical parameters showed again no significant results (P 0.11–0.94; r − 0.02 to 0.32).
Discussion
In our study, we investigated possible changes of IOP during exposure to high altitude in a prospective manner using the gold standard ophthalmological technique for IOP measurement, Goldmann applanation tonometry. Respective raw IOP values were corrected for CCT at high altitude (Goldmann and Schmidt, 1957). IOP assessed by applanation tonometry and corrected for an increased CCT at high altitude was found to be significantly decreased. This finding is in accordance to previously published data using a handheld tonometer (Somner et al., 2007). Furthermore, both corrected and not corrected IOP values did not correlate with any scores of AMS or clinical parameters (HR and SpO2). Therefore, the measurement of IOP does not seem to be a useful tool for diagnosing AMS. In contrast, the role of IOP changes for the prediction of severe high altitude related illnesses involving increased ICP such as HACE still remains to be tested.
In contrast to our study, two previous studies showed a correlation between increasing AMS scores and the reduction in IOP (Cymerman et al., 2000; Pavlidis et al., 2006). Cymerman et al. (2000) examined 11 subjects during a 2-week stay at an altitude of 4300 m and found a decrease in IOP as measured by a noncontact tonometer after 2 days at altitude. In another experiment, IOP was examined in 12 subjects during a 50-hour chamber exposure to 446 mmHg using a contact tonometer, and a positive correlation between AMS and a decrease in IOP was found (Cymerman et al., 2000). The authors concluded that the IOP before and during high altitude exposure may provide a method to assess the individual's response to hypoxic stress. Pavlidis et al. showed a decrease in IOP during an active ascent from 2286 to 5050 m in eight subjects using a contact tonometer during the Greek Karakorum expedition. The decrease in IOP correlated with the assessed LL score (Pavlidis et al., 2006). We are in line with the finding that IOP decreases with gaining altitude, but could not detect any correlation with the assessment scores of AMS or clinical parameters (HR and SpO2). These contrary results may partially be explained by the divergent methods of examination of IOP and the different types of hypoxia exposure (rapid versus slow and gradual ascent). Nevertheless, the use of the state-of-the-art method for measuring IOP and the twice-daily assessment of LL and AMS-C scores in our study warrants validity of IOP assessment and respective correlation analysis to AMS. In addition, another recent study assessing IOP changes in a hypobaric chamber environment up to 18,000 feet using an I-Care tonometer found a significant decrease in IOP after exposure (Nebbioso et al., 2014). However, a number of studies even describe an increase in IOP with gaining altitude exposure up to 5533 m (Ersanli et al., 2006; Somner et al., 2007; Bosch et al., 2010b; Karakucuk et al., 2012). Interestingly, Bosch et al. (2010b) reported no correlation between AMS scores, but found an increase of IOP observed up to an altitude of 5533 m followed by a decrease with further ascent to 6265 m during an expedition to Muztagh Ata (7546 m). In a recent cross-sectional study by Cushing et al. (2013), a median IOP of 21 mmHg (IQR 18–24 mmHg) was measured in 161 volunteers at an elevation of 4392 m, which even presents a mean value above the normal physiological IOP value, but IOP was not correlated with the LL score or oxygen saturation.
In our prospective study, a significant reduction of IOP was only observed after IOP was corrected for the increased CCT at high altitude. Even though there is controversial evidence that correction for CCT in a clinical setting may or may not be useful for calculating actual IOP levels in disease states depending on the type of method used (applanation versus indentation), it certainly should be applied when measuring IOP in the presence of corneal edema such as during high altitude exposure (Herndon 2006; Kohlhaas et al., 2006).
Therefore, we suggest that all studies assessing IOP using an applanation method have to correct for increased CCT levels at high altitude as raw IOP measurements may result in falsely elevated IOP values especially due to the acute onset of corneal edema (Doughty and Zaman, 2000; Morris et al., 2007; Bosch et al., 2010a; Willmann et al., 2013). This may even explain why some of the existing studies found an increase in IOP at high altitude despite the use of applanation tonometry (Somner et al., 2007; Bosch et al., 2010b; Karakucuk et al., 2012). Indeed, Somner et al. using a handheld tonometer and an ultrasound pachymeter for CCT measurements at 3700 m and 5200 m in 76 subjects described elevated raw IOP measurements up to day 3 of exposure at 5200 m compared to baseline measurements at sea level, whereas the measurements of IOP corrected for an increased CCT revealed no significant increase up to day 3, respectively (Somner et al., 2007). Another difference to studies investigating CCT at high altitude using pachymetry was our approach to measure CCT with a Spectralis optical coherence tomography (OCT) device (Somner et al., 2007; Bosch et al., 2010a; Karakucuk et al., 2012). It has been shown that the use of OCT is widely accepted in clinical research for examination of corneal thickness and morphology of the cornea and the anterior chamber (Rio-Cristobal and Martin, 2014; Wu et al., 2014). Furthermore and in line with previous studies, we observed an increase of CCT with raising altitude (Morris et al., 2007; Bosch et al., 2010a; Karakucuk et al., 2012; Willmann et al., 2013). In contrast, the relatively small number of subjects assessed in our study may present a limitation of our study. Both level of exercise and environmental condition (cold temperature) have been shown to reduce IOP (Lempert et al., 1967; Orgul et al., 1995). However, these potentially confounding factors were excluded in our study as all measurements were performed under room air conditions and at rest. One limitation of our study may have been the use of ibuprofen as ocular side effects such as corneal deposits, refractive errors, macular edema, diplopia, or altered aqueous humor dynamics have been reported. However, no ocular side effects were noted during our study possibly due to the small dosage used in our study.
Our data show a small, but significant decrease of IOP corrected for altered CCT upon exposure to acute high altitude hypoxia without any association to AMS. This missing correlation is of particular interest since it is known that cerebrospinal fluid pressure interacts with IOP (Morgan et al., 2016). Hence, our findings indirectly suggest that the pathophysiological basis of AMS may not be caused by an increase in ICP since mean IOP levels even decreased at high altitude.
Overall, it is important to note that high altitude travel in regard to changes of IOP seems to be not harmful for the visual system as the changes found are within the normal range for IOP.
Footnotes
Acknowledgments
The authors thank all participants in the study and the Wilderness Medical Society (WMS) for their support.
Authors Contribution
All authors were involved in the conception, design, and interpretation of data. G.W., K.S., M.S., D.F., F.G., and A.S. were involved in data acquisition and analysis. G.W. and A.S. are responsible for intellectual content and the approval of the final version of the article. In addition, A.S. provided careful statistical advice.
Author Disclosure Statement
No competing financial interests exist.