
Abstract
Abstract
Irarrázaval, Sebastián, Claudio Allard, Juan Campodónico, Druso Pérez, Pablo Strobel, Luis Vásquez, Inés Urquiaga, Guadalupe Echeverría, and Federico Leighton. Oxidative stress in acute hypobaric hypoxia. High Alt Med Biol. 18:128–134, 2017.—The effects of acute hypobaric hypoxia endured by mountaineers were studied, specifically as evidenced by acute mountain sickness (AMS) and oxidative stress damage. Ten male volunteers were exposed to acute hypobaric hypoxia, and AMS was evaluated through arterial oxygen saturation (SaO2), cardiac rate, and the Lake Louise Score (LLS). Oxidative stress was determined through blood profile tests performed 24 hours before and after high-altitude exposure, assessing the oxidative damage and antioxidant profiles. Dietary habits were assessed using the Chilean Mediterranean Diet Index. During ascent (i.e., first 8 hours), all volunteers presented AMS (LLS ≥3 points), as manifested by a median LLS increment of four points, a 15 bpm cardiac rate, and 17% decrease in SaO2. Additionally, plasma lipid oxidative damage increased after the expedition, as evaluated through malondialdehyde, which was directly correlated with the LLS (R2 = 0.720, p = 0.003) and inversely correlated with SaO2 (R2 = 0.436; p = 0.035) at a high altitude. Preascent carbonyl levels were inversely correlated to SaO2 (R2 = 0.490; p = 0.008) and directly correlated to cardiac rate (R2 = 0.225, p = 0.016) at a high altitude. Moreover, dietary habits were inversely correlated with increased carbonyls during the expedition (R2 = 0.436; p = 0.047). In conclusion, acute hypobaric hypoxia induced AMS and an increment in oxidative stress markers 24 hours after altitude exposure in the volunteers. Furthermore, oxidative stress damage was related to AMS severity. Finally, volunteers with closer adherence to a Mediterranean diet presented a lower increase in oxidative damage during ascent, reflecting the potential preventive role of diet against AMS.
Introduction
T
Hypoxia can induce an imbalance between free radical generation and antioxidant protection, resulting in oxidative damage to biomolecules (Askew, 2002). Different clinical studies in humans have identified a series of oxidative stress markers produced following exposure to both hyperbaric and normobaric hypoxia, with or without exercise (Joanny et al., 2001; Bailey et al., 2001a; Wing et al., 2003; Magalhães et al., 2004). The primary underlying mechanism of secondary free radical generation is linked to reduced mitochondrial redox potential and/or increased catecholamine production (Mazzeo et al., 1998). Redox potential decreases due to the accumulation of reduced equivalents that cannot be transferred to oxygen by cytochrome oxidase, a phenomenon termed reductive stress (Kanter, 1998).
It is well known that the frequency of acute hypobaric hypoxia has increased due to a greater interest in certain sporting activities, such as mountain climbing and high-altitude training, as well as to an increase of high-altitude work (Levine and Stray-Gundersen, 1997; Stray-Gundersen et al., 2001; Basnyat and Murdoch, 2003; Gonggalanzi et al., 2016). In this context, antioxidant/prooxidant equilibrium is particularly important since free radical formation could also participate in the complex physiopathology of high-altitude sicknesses (Purkayastha et al., 1999; Bailey and Davies, 2001).
Traditionally, it was believed that oxidative stress originating from vascular muscle and brain damage would explain the endothelial dysfunctions observed in acute mountain sickness (AMS) (Bailey et al., 2001b). Nevertheless, recent studies have found that the accumulation of free radicals could have a physiopathological impact in the brain that is independent of blood–brain barrier disruption and impaired global cerebral oxidative metabolism (Bailey et al., 2009a, 2009b). The objective of this study was to evaluate acute hypobaric hypoxia at high altitudes in the contexts of AMS and oxidative stress. For this, AMS was measured by the Lake Louise Score (LLS), whereas oxidative stress was established by oxidative and antioxidant markers in the blood. Furthermore, the consumption of a Mediterranean diet (MD) was assessed as an influencing factor of AMS.
Methods
Participants
Male volunteers (n = 10) were recruited from the Mountaineering Club of the Pontificia Universidad Católica de Chile to participate in this study (Table 1). The median age of volunteers was 30.1 years of age, with a range between 24.9 and 32.7 years of age. The volunteers presented a median body mass index of 23.8 kg/m2 (ranging from 19.6 to 27.2 kg/m2); 40% were overweight, and 30% had participated in at least one climb within the 3 months before the study. The remaining participants (70%) had not been exposed to high altitudes or participated in any training program in the 3 months before the study. Over a 36-hour period, all volunteers were exposed to acute hypobaric hypoxia, reaching a maximum altitude of 4220 m. This study was approved by the Ethics Committee at the Faculty of Medicine, Pontificia Universidad Católica de Chile.
Study design
High-altitude exposure occurred over the course of 36 hours, with maximum altitude at the summit of Pintor Hill (4220 m), located in the Andes Mountain Range near Santiago, Chile. The ascent began by vehicle in Santiago (655 m) until reaching the La Parva Ski Center (3570 m). The same day, ascent continued on foot until reaching the base of Pintor Hill (4120 m), where participants slept for ∼8 hours. The next day, participants continued ascending on foot until reaching the summit of Pintor Hill (4220 m). Descent was completed on the same day, and participants returned to Santiago. The ascent and descent profiles, in hours, are presented in Figure 1.
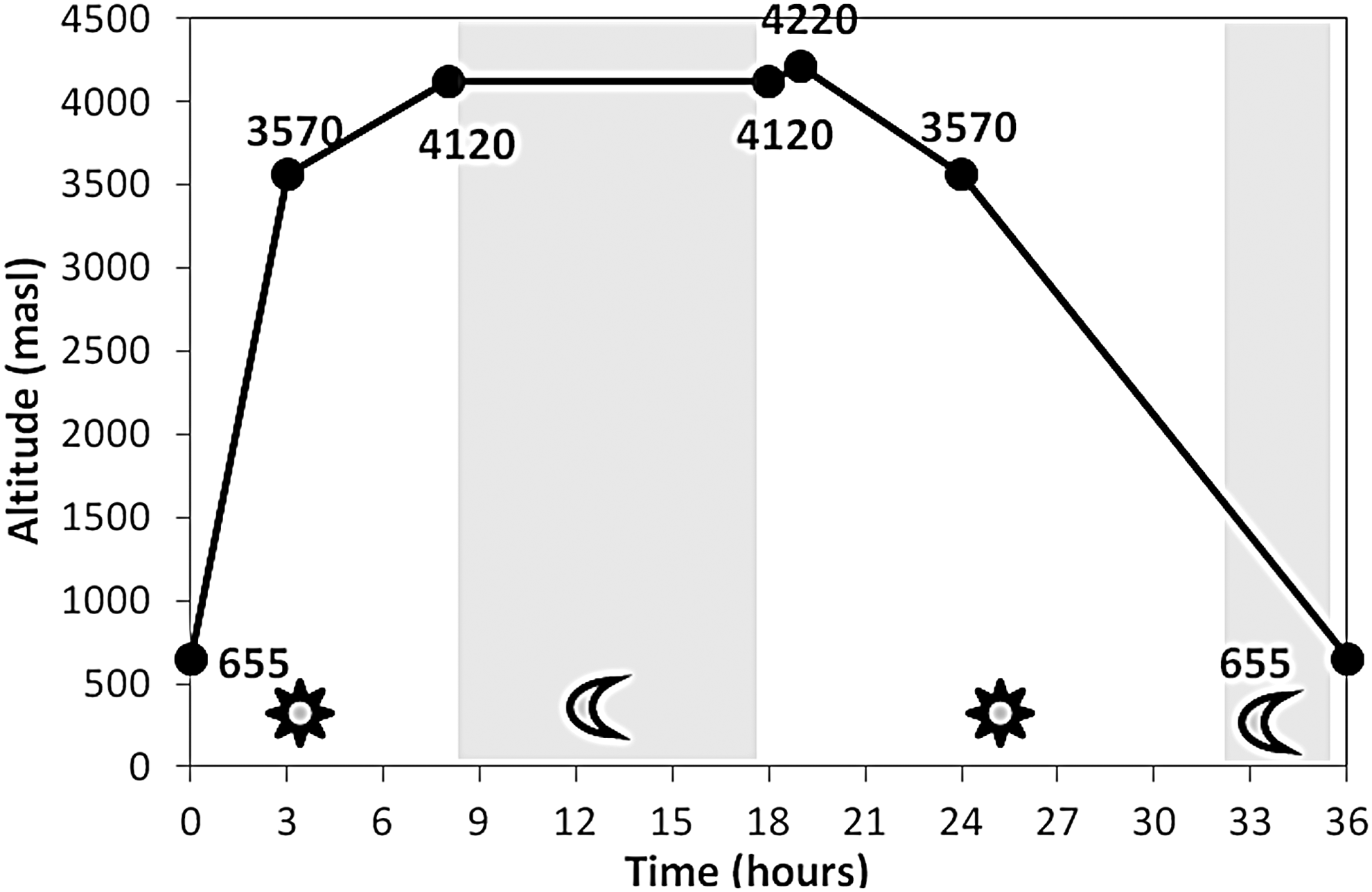
Altitude as a function of time, with exposure to acute hypobaric hypoxia over a 36 time-frame, reaching a maximum of 4220 m. High-altitude exposure occurred over the course of 36 hours, with maximum altitude at the summit of Pintor Hill (4440 m), located in the Andes Mountain Range near Santiago, Chile. The ascent began by vehicle in Santiago (655 m) until reaching the La Parva Ski Center (3570 m). The same day, ascent continued on foot until reaching the base of Pintor Hill (4120 m), where participants slept for ∼8 hours. The next day, participants continued ascending on foot until reaching the summit of Pintor Hill (4220 m). Descent was completed on the same day, and participants returned to Santiago.
The incidence of AMS in participants was periodically evaluated using the LLS for diagnosing high-altitude sicknesses (Sutton et al., 1993), which has grading between 0 and 24. AMS was diagnosed at a score ≥3, with a headache being a cardinal symptom. High-altitude cerebral edema was diagnosed when AMS was associated with compromised consciousness and/or ataxia. Measurements were taken during ascent at 0 hour (655 m), 3 hours (3570 m), 8 hours (4120 m), 18 hours (4120 m), 19 hours (4220 m), 24 hours (3570 m), and 36 hours (655 m).
In addition to LLS, arterial oxygen saturation (SaO2) and heart rate were determined using a pulse oximeter (Onyx Vantage Model 9590; Nonin Medical, Inc.), whereas blood pressure was taken using an automatic digital blood pressure monitor (Model 6073; Braun). Measurements were taken at the same altitudes and at the same intervals as LLS.
Oxidative stress
Antioxidant status and oxidative damage were assessed through blood tests 24 hours before the beginning of the expedition and 24 hours after high-altitude exposure (i.e., 4220 m). Determinations were made according to the Oxidative Damage and Antioxidant Profile (PADO, Spanish acronym) developed by the Center for Molecular Nutrition and Chronic Diseases at the Pontificia Universidad Católica de Chile (Urquiaga et al., 2010). This profile included fasting blood measurements for vitamin C and vitamin E, lycopene, beta-carotene, total antioxidant reactivity, and total reactive antioxidant potential, as plasma antioxidant markers; protein carbonyls, methionine sulfoxide (MetSO), advanced oxidation protein products, and malondialdehyde (MDA), as oxidative stress plasma markers; and GPx, SOD, and catalase as antioxidant enzymes, measured in red blood cells.
Each PADO measurement was expressed in comparison to reference values, which were obtained from the median of each determination from a group of 513 apparently healthy male adults with an average age of 38.3 years. The PADO results were represented as a spider diagram, with each radial axis representing a different antioxidant (vitamin E, lycopene, b-carotene, vitamin C, total antioxidant reactivity, and total reactive antioxidant potential), oxidative damage marker (MetSO, carbonyls, advanced oxidation protein products, and MDA), and antioxidant enzyme (GPx, catalase, and SOD). These results were normalized to reference values.
Mediterranean diet
A questionnaire was given to all volunteers before ascent to evaluate adherence to a MD in the 3 months before the study. This was assessed through the Chilean MD Index, a brief, 14-item index comprised of 22 multiple choice questions. The index was developed and validated for use in Chile by the Center for Molecular Nutrition and Chronic Diseases at the Pontificia Universidad Católica de Chile (Leighton et al., 2009). Chilean MD Index scores range from 0 (minimum adherence) to 14 (maximum adherence).
Statistical analysis
Since data were non-normally distributed (Shapiro–Wilk test), results for continuous variables were presented as median and range, whereas ordinal variables were presented as percentages. A Spearman correlation was used to analyze associations between markers of oxidative stress and antioxidants. A Wilcoxon Signed Rank Test was performed to compare pre and postascent changes in oxidative stress and antioxidant markers. Differences were considered statistically significant at a p < 0.05. Data processing and statistical analyses were performed using the SPSS v15 software.
Results
Symptoms of AMS
During ascent, a progressive increase in the signs and symptoms of AMS was observed, with average scores >3 from hour 8 of the expedition (4120 m; Fig. 2). All volunteers presented with AMS during the study (i.e., ≥3 points on LLS), but none presented with high-altitude cerebral edema.
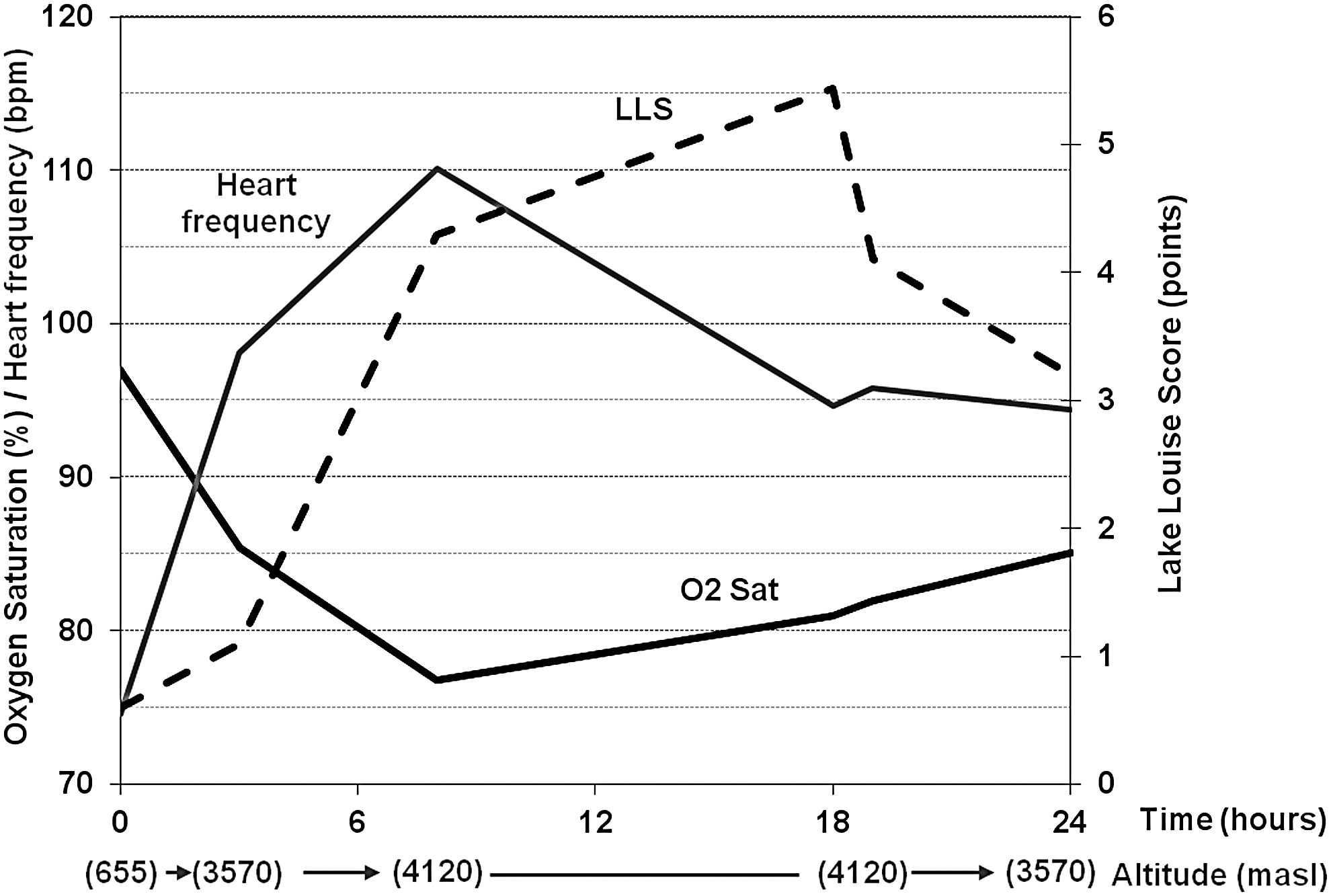
Changes in arterial oxygen saturation (O2 Sat), cardiac rate (Heart Freq), and LLS in relation to altitude. Evaluations were taken during ascent at 0 hour (655 m), 3 hours (3570 m), 8 hours (4120 m), 18 hours (4120 m), 19 hours (4220 m), 24 hours (3570 m), and 36 hours (655 m). LLS, Lake Louise Score.
Vital signs
As the ascent continued, there was an observed progressive decrease in SaO2, the lowest recorded values of which were obtained at hour 8 of the ascent (4120 m), just before participants went to sleep (76% average). From hour 18, at the same altitude, there was a steady increase in SaO2 levels, even at the summit (19 hours, 4220 m; Fig. 2).
Participant heart rates showed a similar, although inverse, behavior as SaO2. At rest, heart rate measurements progressively increased during ascent (100 bpm maximum average), but after hour 8 of the ascent (4120 m), the recorded resting heart rates began to decrease (Fig. 2).
Oxidative stress
Regarding antioxidant status and oxidative damage, when comparing profile results 24 hours before ascent with results 24 hours after ascent, significant differences were obtained for MDA and GPx values. Specifically, MDA increased postexpedition (p = 0.009), and GPx decreased postexpedition (p = 0.028, Fig. 3). No differences were found in antioxidants (vitamin C, vitamin E, b-carotene, and lycopene), in total antioxidant capacity (total antioxidant reactivity and total reactive antioxidant potential), in oxidative damage markers (advanced oxidation protein products and MetSO), or in antioxidant enzymes (catalase and SOD).
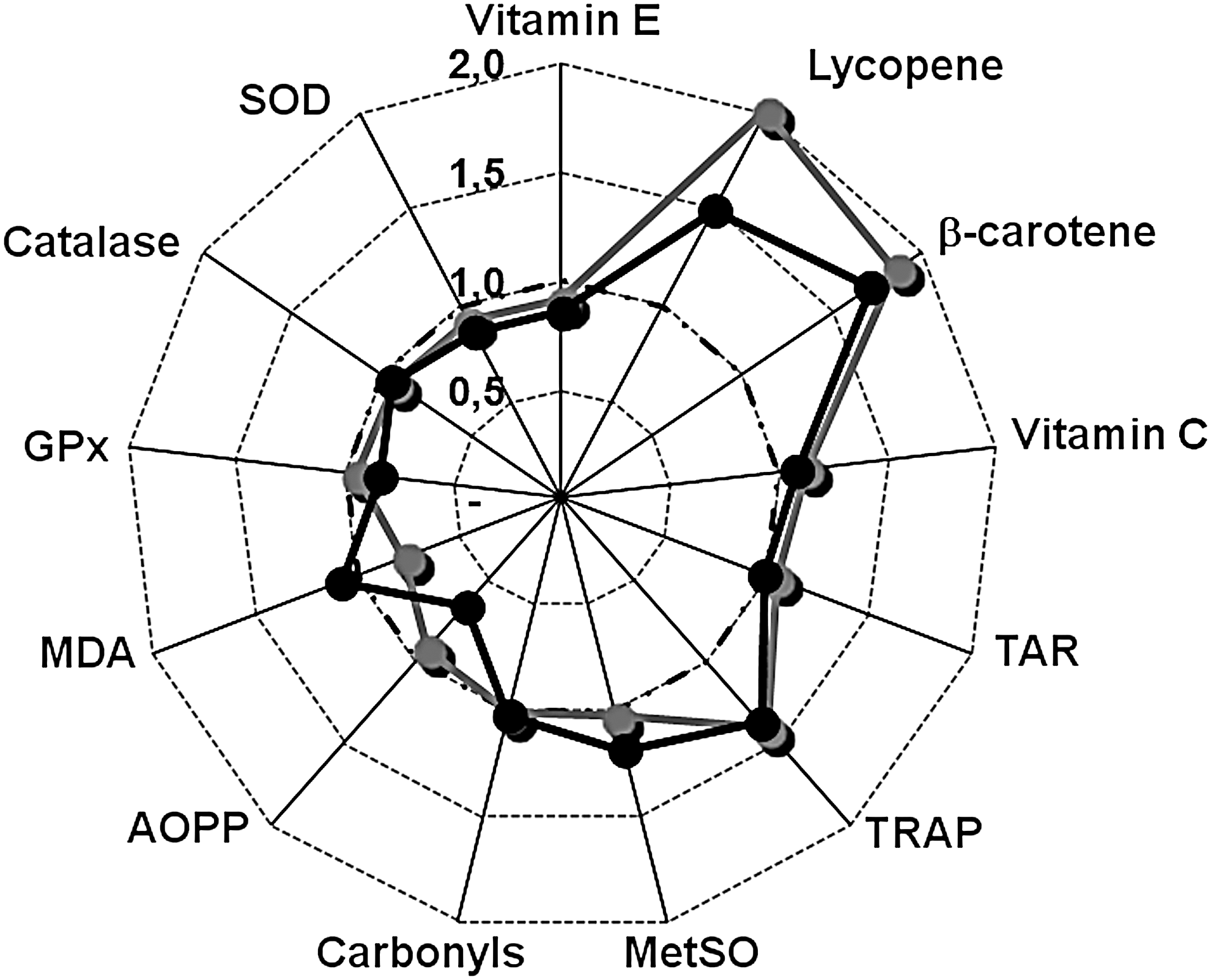
Oxidative stress and antioxidant profile. The PADO is shown as a spider diagram, where each radial axis represents a different antioxidant (vitamin E, lycopene, b-carotene, vitamin C, TAR, TRAP), oxidative damage marker (MetSO, carbonyls, AOPP, MDA), and antioxidant enzyme (GPx, catalase, SOD) determination, normalized to reference values. Reference values were obtained from the median of each determination from a group of 513 apparently healthy male adults with an average age of 38.3 years. Significant differences were recorded with regard to MDA (p = 0.009), which increased postexpedition, and to GPx, which decreased postexpedition (p = 0.028). AOPP, advanced oxidation protein products; GPx, glutathione peroxidase; MDA, malondialdehyde; MetSO, methionine sulfoxide; SOD, superoxide dismutase; TAR, total antioxidant reactivity; TRAP, total reactive antioxidant potential.
On the other hand, preascent plasma vitamin C concentrations correlated significantly with pre and postascent plasma protein carbonyl values (p = 0.012 and p = 0.001, respectively). When comparing markers of oxidative stress with clinical AMS symptoms, an inverse relationship was found between ΔMDA (post- and pre-expedition) and SaO2 at 4120 m. In turn, a direct relationship was observed between ΔMDA and LLS at 4120 m (Fig. 4). Additionally, when comparing preascent oxidative damage markers with changes to clinical AMS symptoms, only preascent carbonyl levels significantly correlated to SaO2 and heart rate. A decrease in SaO2 was directly correlated to preascent carbonyl levels (p = 0.008), whereas an increase in heart rate was directly correlated to preascent carbonyl levels (p = 0.016; Fig. 5). Finally, when comparing postascent oxidative damage markers with changes to clinical AMS symptoms, only protein carbonyl values and advanced oxidation protein product values were significantly correlated with heart rate changes during ascent (p = 0.012 and p = 0.041, respectively).
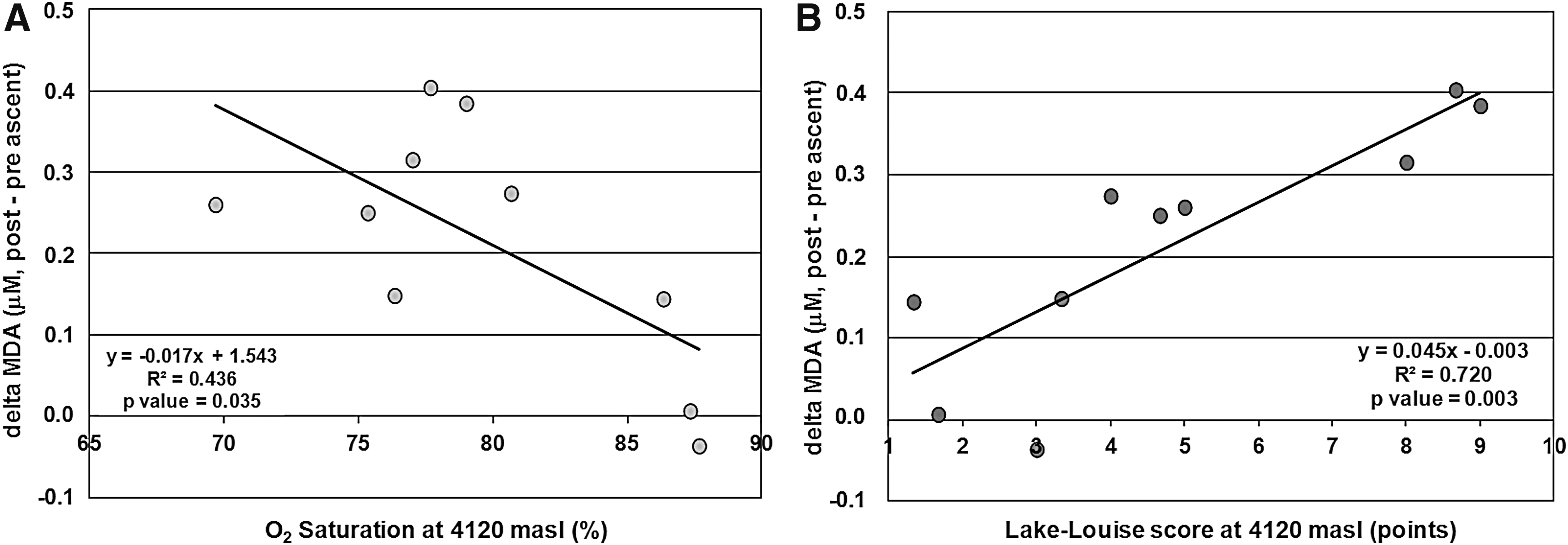
Correlation between

Relationship between changes in oxygen saturation
Mediterranean diet
The median Chilean MD Index score was 4.5 points (range 3.0–6.5 points), where 60% of volunteers had low adherence and 40% had moderate adherence to the MD (Table 1). Adherence to the MD was inversely correlated to oxidative damage in plasma proteins. Volunteers with a higher adherence to a MD presented a lower increase in plasma protein carbonyls during the expedition (R = 0.66, p = 0.047) (Fig. 6).
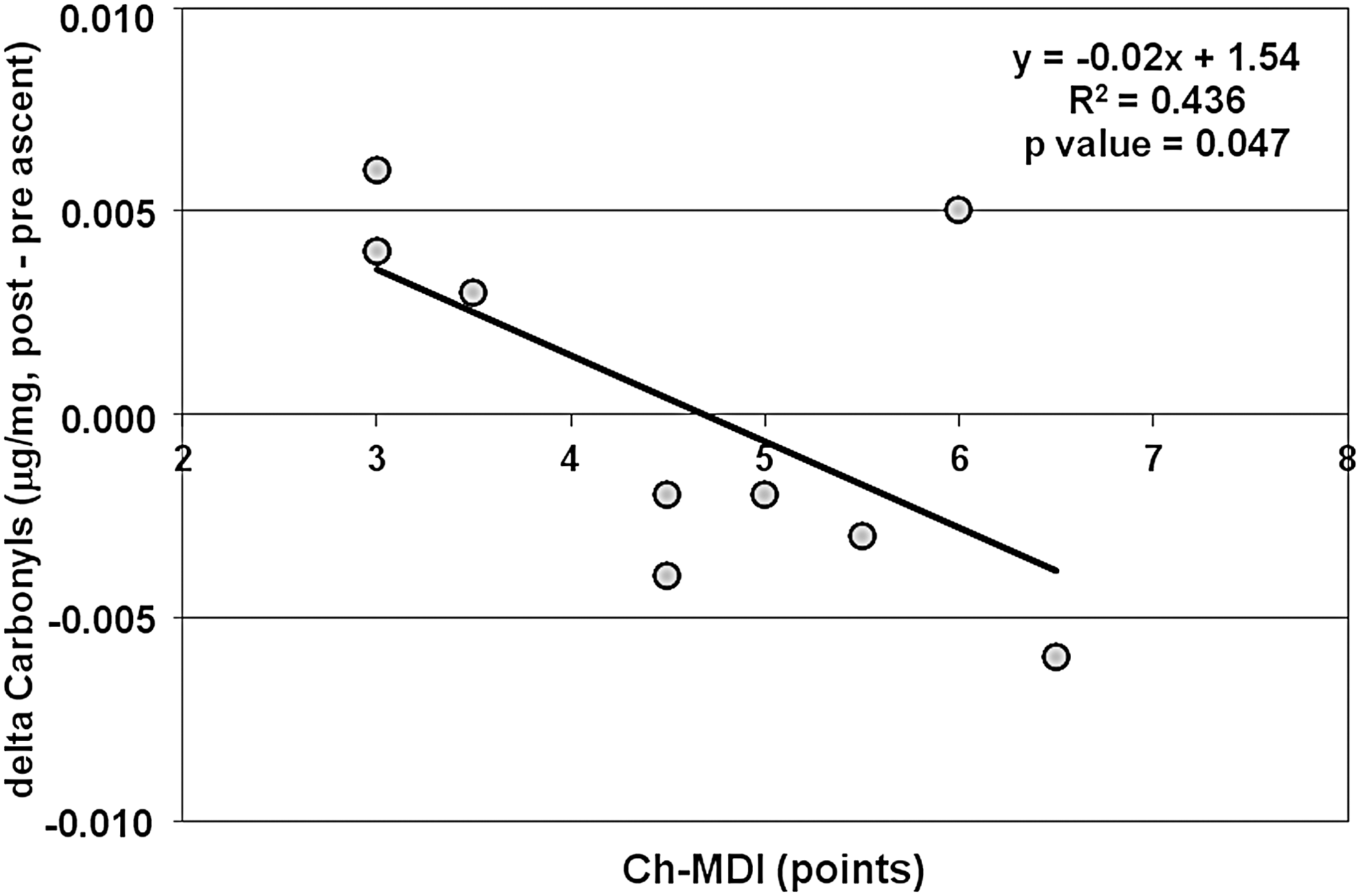
Correlation between diet quality and changes in carbonyls after exposure to acute hypobaric hypoxia. Diet quality was assessed by the Chilean Mediterranean Diet Index (Ch-MDI). Delta Carbonyl concentration in plasma protein was determined as the difference between post and pre-expedition measurements.
Discussion
The results of this study support that acute hypobaric hypoxia induces AMS, as objectively determined through the clinical LLS. The main etiological factor in the physiopathology of this disease was hypoxemia, which occurred secondary to the lower inspired partial pressure of high altitude oxygen. This was observed as a decrease of SaO2 in all subjects. Although AMS is, by definition, self-limited and nonlethal, in physiopathological terms, sustained high-altitude cerebral edema is a condition that, if left untreated, can progress within 24 hours to coma and posterior death from cerebral herniation (Hackett et al., 1998; Bärtsch and Swenson, 2013).
Acclimatization to hypobaric hypoxia through compensation mechanisms, such as hyperventilation, decreases hypoxemia. Subsequently, SaO2 increases and AMS scores decrease. This was observed in group participants 18 hours after high-altitude exposure (i.e., at 4120 m). Considering that the ventilatory response mechanisms to hypoxia are progressive and more effective during periods of rest at the same altitude, this change in participants was expected.
Regarding pro-oxidant/antioxidant equilibrium, an imbalance was found in study participants 24 hours after exposure to hypobaric hypoxia. Sampled blood markers of oxidative stress and of the antioxidant profile after hypoxia exposure revealed a decrease in antioxidants and an increase in damage markers. In particular, there was a significant increase in MDA and MetSO levels.
Two primary mechanisms underlie oxidative damage during hypobaric hypoxia. The first mechanism is the result of reduced mitochondrial redox potential and/or increased catecholamine production (Mazzeo et al., 1998). Specifically, redox potential decreases due to the accumulation of reduced equivalents that cannot be transferred to oxygen by cytochrome oxidase, a phenomenon termed reductive stress (Kanter, 1998). Furthermore, free radical levels can increase under hypoxic conditions following activation of the enzymes xanthine oxidase (Sohn et al., 2003), NADPH oxidase (Jones et al., 2000), phospholipase A2 (Neidlinger et al., 2005), and nitric oxide synthase (Jung et al., 2000).
The second mechanism for free radical generation during hypobaric hypoxia is related to the xanthine dehydrogenase/oxidase system (Radák et al., 1994). In this case, when the available oxygen is low, as occurs under circumstances of ischemia or exposure to altitudes over 6000 m, cells tend to generate ATP. This reaction occurs through the interaction of two ADPs and is catalyzed through the enzyme adenylate kinase. Additionally, this process generates AMP, which cannot be recycled and is subsequently catabolized to form hypoxanthine. In the presence of proteases related to calcium, xanthine dehydrogenase can convert into xanthine oxidase, which is then used instead of NAD+ as an electron receptor. Consequent xanthine production is accompanied by the production of superoxide anions or H2O2. The xanthine dehydrogenase/oxidase system is a potent generator of ROS under conditions of hypoxia/reperfusion. Worth highlighting, intermittent exposure to high altitudes is characteristically similar to conditions of ischemia/reperfusion.
It is worth noting that this study found correlations between different markers of oxidative stress. Important among these, when comparing the pre-exposure antioxidant status with pre- and postexposure oxidative damages, an inverse relationship was found between vitamin C and carbonyls. Similarly, comparing pre- and postexposure changes (delta, Δ) revealed that an inverse relationship was found between ΔGPx and ΔMetSO. Finally, between the pre- and postexposure markers of oxidative stress, a direct correlation was found between pre-exposure MetSO and postexposure MDA.
In turn, when oxidative stress markers were compared against clinical symptoms, ΔMDA was found inversely related to SaO2 and directly related to clinical symptoms of AMS, as objectively measured through LLS. Therefore, less oxidative damage, as evidenced by more SaO2 and a lower LLS, was found through ΔMDA. Considering this, we suggest that the greater oxidative damage indicated by ΔMDA would be related to greater hypoxemia. This was evaluated through SaO2 and the relationship of this with greater AMS, as determined through the LLS.
Oxidative status before high-altitude exposure could also play an important role. Indeed, low basal levels of oxidative damage markers, such as carbonyls, were correlated with a lesser decrease in oxygen saturation during ascent.
Finally, specific comparisons between MD score and oxidative damage revealed Δcarbonyls to be inversely related to the obtained diet score. The MD is characterized by a relatively large consumption of olive oil, poultry, fish, fruits, vegetables, and cereals, a moderate intake of red wine, and a low consumption of red meats. There is evidence that populations that consume diets rich in these foods have, on average, higher plasma concentrations of vitamin C and E, carotenoids, and antioxidants polyphenols, in addition to showing lower amounts of oxidative damage (Urquiaga et al., 2010). Through multiple synergistic mechanisms derived from the presence of these components, MD generates several physiological and metabolic changes (e.g., improvement in antioxidant profile, lipid profile, blood pressure, inflammation, and coagulation, as well as modulating gene expression). Consequently, people who consume a MD should be better prepared to confront hypoxia due to having a more favorable antioxidant and oxidative damage profile.
Therefore, stricter adherence to a MD could act as a protective factor to the oxidative stress induced by hypobaric hypoxia.
Conclusion
In conclusion, the results of this study suggest that acute hypobaric hypoxia induces AMS and increases oxidative stress. Related to this, a superior adaptation to high altitudes, as indicated by better oxygen saturation and fewer symptoms of AMS, could translate into less oxidative damage, as primarily represented by changes in MDA. Finally, lower postascent oxidative damage was observed in volunteers with low preascent oxidative damage and with higher adherence to a MD, thus reflecting the importance of oxidative status and the potential role of diet as a prevention factor against AMS.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest or financial ties to report.