
Abstract
Abstract
Reno, Elaine, Talia L. Brown, Marian E. Betz, Michael H. Allen, Lilian Hoffecker, Jeremy Reitinger, Robert Roach, and Benjamin Honigman. Suicide and high altitude: an integrative review. High Alt Med Biol 19:99–108, 2018.
Introduction:
Suicide rates are greater at high altitudes, and multiple mechanisms have been suggested for this relationship, including hypoxia, differences in population density, characteristics of suicide victims, and firearms ownership and access. To better understand these potential mechanisms, studies evaluating the associations between high altitude and suicide were examined.
Methods:
A literature review of published studies on high altitude and suicide was conducted in Medline, Embase, Web of Science, the Cochrane Database of Systematic Reviews, and the Cochrane CENTRAL database. We extracted and analyzed all studies that met the inclusion criteria, excluding foreign language studies and letters. Most of the measurements and results were synthesized using modified Letts' criteria.
Results:
Searches using an extensive list of keywords returned 470 articles, but only 6 met the inclusion criteria. The studies' samples ranged in size from 8871 to 596,704, while studies which did not document sample size reported suicide rates. In five of the studies selected, individuals living at high altitudes were at greater risk of suicide. Four studies used aggregated data at a county or state level to analyze variables, such as age, gender, race, socioeconomic factors, and firearms access. All the studies found that high altitude was independently associated with suicide. One study found that many individual characteristics of those who committed suicide were different at high altitudes than low altitude, including a lack of access or barriers to mental healthcare. Depression exacerbated by hypoxia was hypothesized as a possible biologic mechanism in three studies.
Conclusion:
These research studies published since 2009 support an association between high altitude and suicide rates at the state or county level, but do not provide sufficient data to estimate the effect of high altitude on an individuals' suicide risk. Although the impact of hypoxia on mood and depression has been hypothesized to be a contributing cause, many other individual factors likely play more important roles.
Introduction
S
Recently, high-altitude residence has been proposed as an additional potential explanation for these geographic differences (Cheng et al., 2005; Haws et al., 2009; Brenner et al., 2011). Some researchers have theorized that the link between high altitude and suicide risk is a direct result of high-altitude hypoxia in the brain (Kim et al., 2011; Young, 2013). Researchers suggested that, as ambient oxygen levels drop with increasing elevation, even individuals living at elevations of <3000 ft (900 m) might have enough hypoxic insult to be predisposed to a higher suicide risk (Haws et al., 2009; Brenner et al., 2011; Kim et al., 2014). However, many physiologic changes indicating hypoxic responsiveness, such as increased ventilation (Donoghue et al., 2005), raised hematocrits (Weil et al., 1968), and detectable erythropoietin release (Ge et al., 2002) occur only at much higher elevations (Swenson, 2011), casting doubt on this hypothesis.
Despite these doubts, some have suggested that hypoxia can result in negative moods that might persist for weeks after hypoxic exposure (Shukitt and Banderet, 1988; Bardwell et al., 2005). Many mechanisms have been proposed to account for this mood effect, including influences on brain neurotransmitters, drug pharmacokinetics, and cellular metabolism (Delmastro et al., 2011; Gamboa et al., 2011; Helbich et al., 2013; Asiri, 2014). Other factors that occur at high altitude, such as lower barometric pressure and changes in lithium metabolism, have also been shown to alter human behavior, mental health, and suicide (Jurgens et al., 2002; Arancibia et al., 2003; Schory et al., 2003; Maldonado et al., 2009). To better understand the relationship between suicide and high altitude, a comprehensive integrative review of the research literature was performed.
Methods
Literature search
A medical research librarian (L.H.) conducted the literature search and identified studies in the following databases: MEDLINE (Ovid, 1946 to present), Embase (Embase.com, 1980 to present), Web of Science (1974 to present), Cochrane Database of Systematic Reviews (Wiley), and Cochrane Central Register of Controlled Trials (Wiley). No language or year limits were applied initially, and the searches were complete through June 2016.
The search strategies centered on the terms altitude and suicide, using multiple subject headings and text-word terms to describe these concepts. The concept set for “high altitude” includes the terms, hypoxia, anoxia, altitude, altitude sickness, elevation, mountain, mountaineering, Himalaya, Tibet, Rocky Mountains, Rockies, Colorado, Peru, Andes, and Alps. The concept set for suicide included suicide, suicidality, suicidal ideation, suicide prevention, attempted suicide, and suicidal behavior. The search terms were truncated using wildcards to capture phrases and spelling variations. Phrases were searched using proximity syntax or quotation marks. Where appropriate, subject headings were expanded to include subcategories. Complete details of the search strategy for the MEDLINE database are presented in Appendix A1.
Inclusion and exclusion criteria
Eligible studies were controlled experimental or observational studies that (1) examined human subjects aged ≥10 years, were conducted in any country, were written in English, and provided data on both suicide rates and the altitude of victims' residences. Given the specific interest in suicide outcomes, only studies that had suicide as a primary outcome were included. The exclusion criteria included animal studies; studies evaluating mental disorders, such as bipolar disorder and depression, at high altitude; studies investigating these psychiatric disorders when suicide was a secondary outcome; elevation defined as a height from which an individual jumped or fell, leading to suicide determination not associated with the high altitude of the residence; foreign language studies; and nonresearch publications, such as news reports, commentaries, editorials, and letters that provided no methodology for how the results were obtained.
Review and data abstraction
From the initial search results, we removed any duplicates, identified nonrelevant citations (e.g., animal studies), and noted study design details in the remaining sample. Two reviewers (T.L.B. and B.H.) independently screened all the retrieved records. One reviewer (T.L.B.) was specifically chosen based on her background in epidemiologic studies and lack of affiliation with any publication on this subject to minimize bias in both article selection and analysis. Any differences in opinion would have been resolved by a third reviewer, but no differences in article selection occurred.
The six studies ultimately included in the review were studied and analyzed in depth. Modified Letts' critical-review criteria were used to determine the strengths and weaknesses of each study (Letts et al., 2007). The factors analyzed included study design, data collection process and procedures, data analysis, conclusions, implications, and methodologies for measuring suicide rates and determining high altitude. Considering all of these factors and based on the inclusion criteria, one study was determined to be methodologically sound (Betz et al., 2011), two methodologically weak (Brenner et al., 2011; Kim et al., 2011), and three methodologically poor (Haws et al., 2009; Selek, 2013; Kim et al., 2014). The strengths and limitations of the included studies are discussed more fully in the Results and Discussion sections.
Ad-hoc analysis using the Web-based Injury Statistics Query and Reporting System (WISQARS) Injury Mapping Module developed by the CDC was conducted to better understand the findings from the selected studies (CDC, 2016). This approach was chosen to analyze the counties with the highest suicide rates, which would more fully explore the relationship between suicide and altitude using a different methodology than described in the six selected studies.
Results
The original search methodology identified 470 articles. Figure 1 displays the elimination process used to select the final six articles, which were published from 2009 to 2014. Four studies were based in the United States, and one each in South Korea and Turkey. The populations studied were largely drawn from country-specific national statistical reporting data. Suicide rates were also determined using databases specific to each country: for the United States, the National Violent Death Reporting System, state suicide rates, and CDC mortality data; for South Korea, the national statistical office; and for Turkey, province' suicide rates. The outcomes evaluated were based on both adjusted and unadjusted suicide rates.
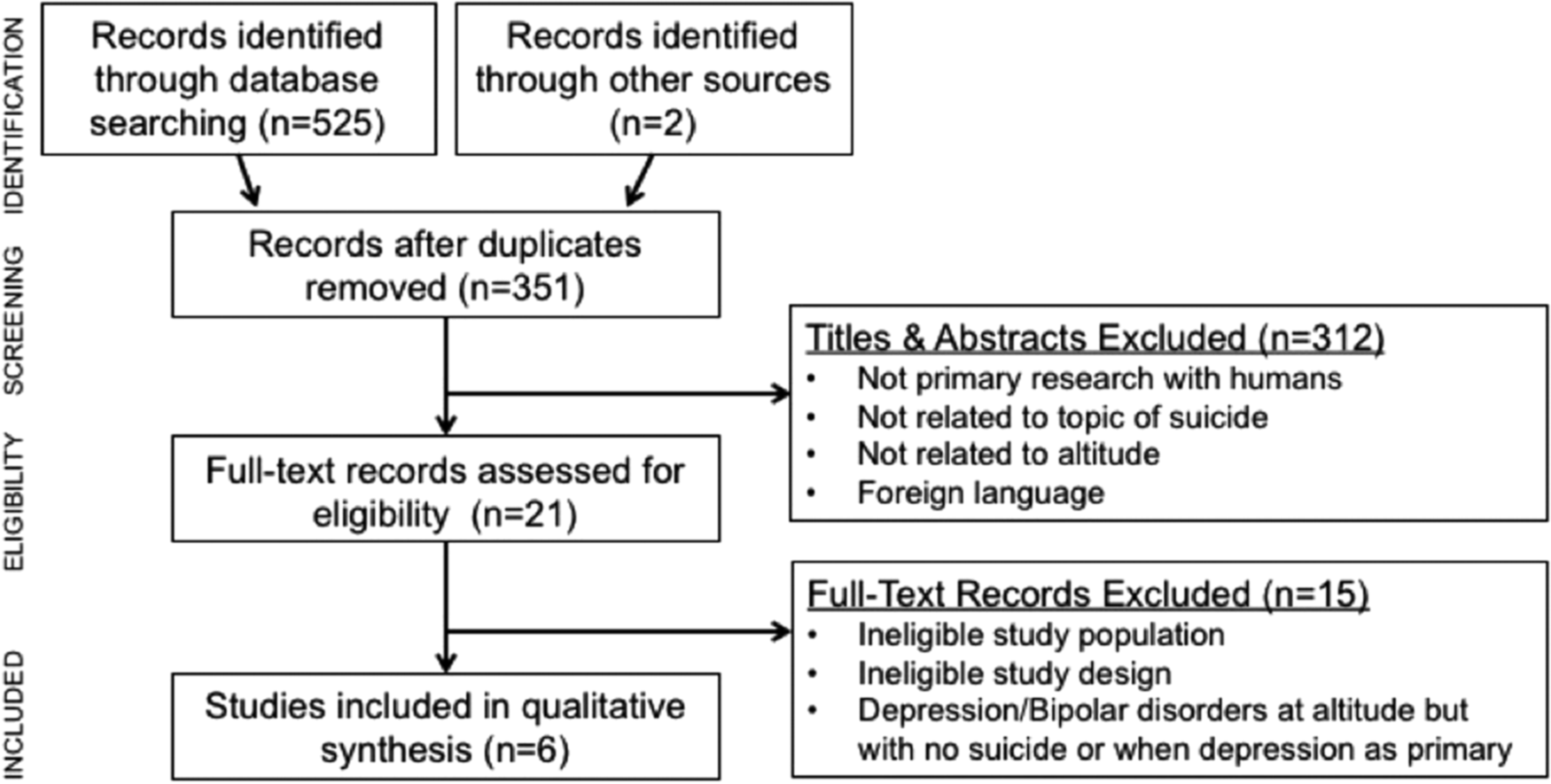
Flow diagram of identification, review, and final articles included in the systematic review. Adapted from Moher et al. (2009).
The sample size of the studies ranged from 8871 to 596,704 people. High altitude was measured in several ways. Five of the six studies calculated the average high altitude for states, counties, or administrative districts and produced results ranging from sea level to >10,000 ft (3030 m). One study divided high altitude into three categories—low (<3300 ft, 1000 m), middle (3300–6600 ft, 1000–2000 m), and high (>6600 ft, 2000 m)—and grouped the counties studied into these categories (Betz et al., 2011). Actual elevation measurements also varied among studies, with four utilizing nation-wide state or county elevation data and one Google Earth for GPS measurements. One study did not provide information about how the altitude of each county was determined. The key features of the selected studies are shown in Table 1.
The review made evident several methodologic problems in these studies. Measurements of altitude and populations in relationship to suicide varied across the six studies. Haws et al. (2009) measured altitude using the mean altitude of state capitals, while others (Betz et al., 2011; Brenner et al., 2011; Kim et al., 2011) used county-level data, which are more precise, but still cover a large geographic scope. The use of more granular data, such as zip codes and census tracts, could improve the association of suicide with more precise elevations. In addition, the suicide rates in three articles were calculated using the denominator census data on population from a 20-year period that did not precisely correspond to the years used for suicide cases in the numerators, raising the possibility of bias in these measurements (Haws et al., 2009; Brenner et al., 2011; Kim et al., 2011). Four studies were limited because they used aggregated, regional-level data without controlling for person-level factors in each suicide case (Haws et al., 2009; Brenner et al., 2011; Kim et al., 2011, 2014). One study assessed the individual characteristics of suicide victims, but only measured suicides in a 15-state region (Betz et al., 2011). This study found that suicide victims at high altitudes differed significantly from those at low altitudes in multiple demographic, mental health, and suicide-related characteristics, even after adjusting for rural residence (Betz et al., 2011). A detailed analysis of many covariates used in the articles and their relationships to suicide and high altitude is given in Table 2.
Suicide and high altitude
Five of the six studies reviewed demonstrated higher suicide rates at high altitudes (Haws et al., 2009; Betz et al., 2011; Brenner et al., 2011; Kim et al., 2011, 2014). This finding was consistent despite the use of different methods to measure high altitude and different databases to identify populations. Although all studies indicated difficulty determining actual suicide rates, one study reported an unadjusted suicide rate of 17.7 suicides per 100,000 people at high altitudes and 5.7 suicides per 100,000 at low/high altitudes (Betz et al., 2011). Another study showed that the threshold value for increased suicide rates occurred between 2000 and 2999 ft (606 and 909 m) (Brenner et al., 2011), an elevation that has not been clinically shown to have physiologic consequences. Curiously, despite an overall age-adjusted higher suicide rate at high altitude in the United States, there was not a statistically significant relationship in suicide rates and high altitude when isolating the 50 U.S. counties with the highest suicide rates (Kim et al., 2011).
Studies from outside the United States have reported mixed results. South Korean data demonstrated a positive correlation between age-adjusted suicide rates and mean high altitude, although the highest elevations reported were only 3300 ft (1000 m) (Kim et al., 2014), while data from Turkey showed no correlation between high altitude and suicide rates in 81 provinces (Selek, 2013).
In an ad-hoc analysis using the WISQARS database, we reviewed suicide by county in the United States, determined mean county elevations and suicide rates, and compared that rate to the national mean suicide rate (Fig. 2 and Appendix Table B1; CDC, 2016). Two observations stand out from Figure 2. First, more counties with higher suicide rates are at elevations of <2500 ft (758 m), and the relationship from 5000 to 10,000 ft (1524–3048 m) is relatively flat. The counties with the highest suicide rates are in South Dakota and Alaska, which are all below 3200 ft (970 m), and many other counties with high suicide rates are at or near sea level, which calls into question the strength of the association between high altitudes and suicide rates.
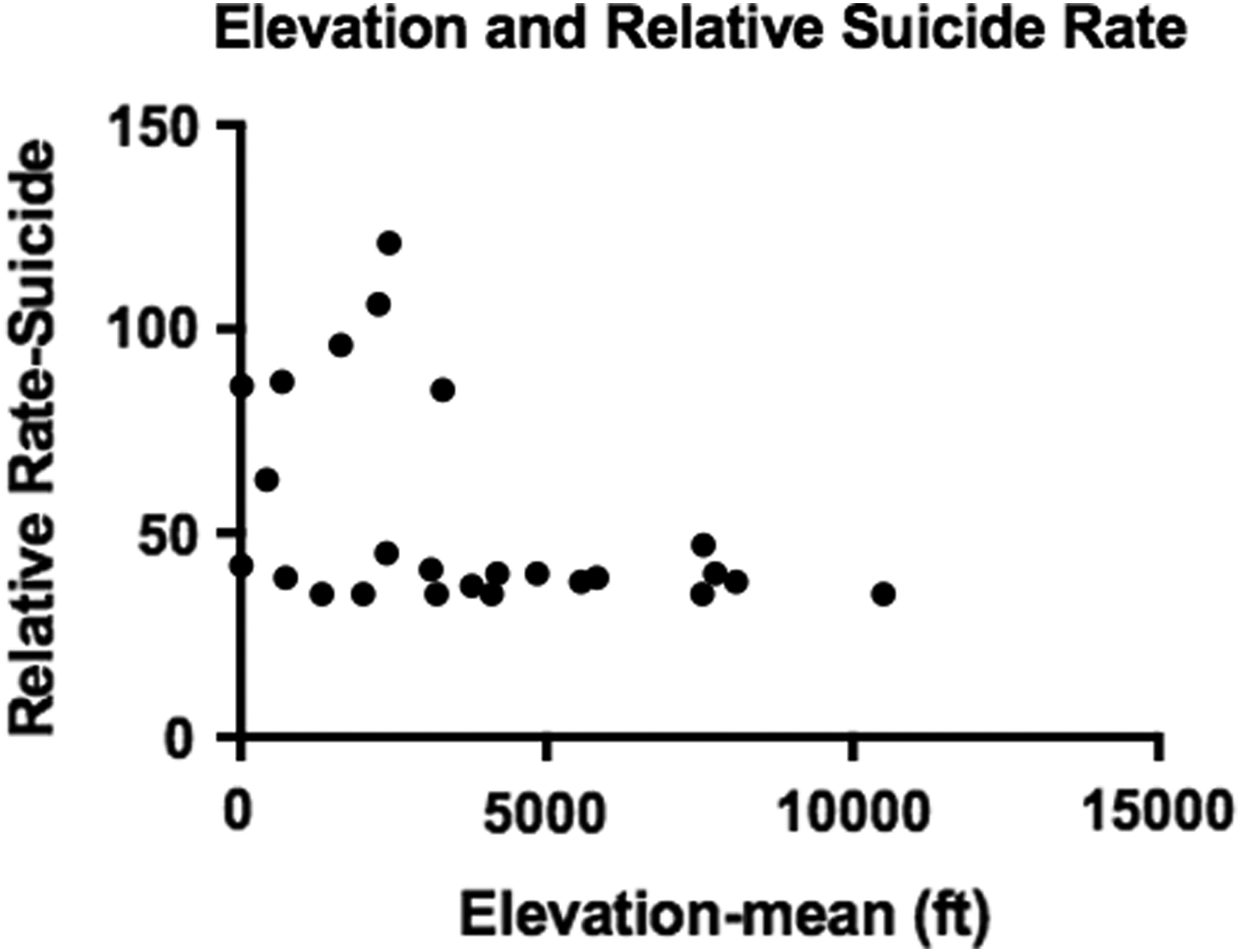
Depiction of the elevation of all U.S. counties with rate of suicide per 100,000 people >2.6 times the U.S. mean of 13.3.
Relationship of gender and suicide to high altitude
Several studies adjusted for gender in relationship to high altitude and suicide (Haws et al., 2009; Betz et al., 2011; Brenner et al., 2011; Kim et al., 2011). The majority (76%–79%) of suicide victims were male, which did not change between low, middle, and high altitude (Betz et al., 2011). Three studies adjusted for gender in their analyses, but did not treat gender as an independent factor (Haws et al., 2009; Brenner et al., 2011; Kim et al., 2011).
Relationship of age and suicide to high altitude
Four of the six studies evaluated age as a covariate (Haws et al., 2009; Brenner et al., 2011; Kim et al., 2011). Betz et al. (2011) reported that the median age of suicide victims was 45 years, with no significant difference based on high altitude. Others, however, did find a positive correlation between age-adjusted suicide rates and high altitude (Haws et al., 2009; Brenner et al., 2011; Kim et al., 2011).
Relationship of suicide and firearms to high altitude
Three of the six studies included firearms data in the evaluation of suicide and high altitude, and all found that firearms were more commonly involved in suicides at high altitudes (Betz et al., 2011; Brenner et al., 2011; Kim et al., 2011). Betz et al. (2011) showed that a higher proportion of suicides completed at high altitudes compared to low altitudes involved firearms (58.4% vs. 51.4%). Kim et al. (2011) showed that firearm suicide rates and nonfirearm suicide rates were both positively correlated with higher altitude and elevation had a stronger correlation with age-adjusted suicide rates than gun ownership. In a comparison of the counties with the highest firearm-suicide rates and the counties with the lowest firearm-suicide rates, the suicide rate between the counties with the highest elevation (4096 ft; 1234 m) and the lowest elevation (324 ft; 99 m) differed by 22.6-fold. When firearms were removed as a method of suicide, the difference in suicide rates decreased significantly to 12.5-fold (Brenner et al., 2011).
Relationship of race and suicide to high altitude
Four of the six studies considered race to be a factor in suicide and high altitude with differing data (Haws et al., 2009; Betz et al., 2011; Brenner et al., 2011; Kim et al., 2011). Most suicide victims were white (89.0%–93.9%) and non-Hispanic (86.5–96.9%) (Betz et al., 2011). African Americans accounted for a higher proportion of suicide victims at lower altitudes than higher altitudes (p < 0.001), while American Indians and Alaskan Natives accounted for a higher proportion at high altitudes (p < 0.001) (Betz et al., 2011). Kim et al. (2011) found no statistically significant correlation with race and suicide. Haws et al. (2009) adjusted for race as a variable, but did not correlate race with altitude or suicide rates.
Population density and suicide
Some studies showed that lower population density resulted in more suicides in all locations and suicide victims at high altitudes were more likely to live in rural areas with low population density (Betz et al., 2011; Kim et al., 2011). The findings from this analysis of the WISQARS database identified counties in South Dakota and Alaska as having the highest suicide rates in the country (CDC, 2016). These counties were rural and had low population density and low altitudes.
Other suicide predictors at high altitudes
Suicide victims living higher than 3300 ft (1000 m) were found to be more likely to suffer from depressed moods, although high- and low-altitude victims had equal rates of current psychiatric diagnoses and current or prior mental healthcare (Betz et al., 2011). Suicide cases at high altitudes (higher than 6600 ft or 2000 m) were more likely to involve suspected intoxication at the time of death and a crisis or contributing social problem in the weeks before death (Betz et al., 2011).
Discussion
In this integrative review, five of the six studies reported higher suicide rates at altitude (Haws et al., 2009; Betz et al., 2011; Brenner et al., 2011; Kim et al., 2011, 2014). However, four of these studies were limited because they used aggregated, regional-level data without controlling for person-level factors in each suicide case, which is called an ecologic fallacy (Haws et al., 2009; Brenner et al., 2011; Kim et al., 2011, 2014). Although epidemiologically interesting, these studies' findings do not permit stating definitively that high altitude per se is the cause. Rather than an aggregate measure based on where people live, an ideal study design would be to attach an accelerometer to individuals to measure their individual elevation exposure. People living in the mountains probably experience elevation changes throughout the day depending on where they work; so all the studies reviewed have poor measures of individual elevation exposure. Ecologic studies help identify correlations worthy of further investigation and can demonstrate population-level phenomenon, but cannot prove causal associations. Therefore, individual-level studies are needed to understand cause and effect.
Only one of the six studies reviewed investigated the associations of individual characteristics with suicide fatalities (Betz et al., 2011). The relative strength of the study by Betz et al. (2011) is that they could adjust for individual-level factors, whereas the ecological studies could not.
Betz et al. (2011) found that suicide victims at high and low altitudes differed significantly in multiple demographic, mental health, and suicide-related characteristics, including race, Hispanic ethnicity, intoxication, firearms use, report of depressed mood before suicide, and recent financial, job, legal, and interpersonal problems. Even after adjusting for rural residence, numerous differences in personal, mental health-related, and suicide characteristics among those living at higher and lower altitudes remained. These issues appear to be more important reasons for differences in suicide rates than physiologic causes, such as hypoxia.
Several factors warrant closer scrutiny to better explain the differences in rates and understand how the researchers drew conclusions in these six studies. These factors include, foremost, measurements and definitions of high altitude, as well as firearm access and ownership, population density, and ethnicity.
Measurement of altitude
How high altitude is measured and defined could have significant impacts on the findings. Three of the studies used a large geographic region, such as a state (Haws et al., 2009), county (Brenner et al., 2011), or administrative district (Selek, 2013; Kim et al., 2014), to determine elevation. Using such a large area is problematic because the significant variations in elevation across these regions made it impossible to determine precisely at which elevations suicide victims lived. In some Colorado counties, for example, the altitude ranges from 4000 to 8000 ft (1212–2400 m). In addition, two studies excluded from analysis 20 counties that had <20 suicides during the dates studied, and it is unclear whether these counties were at high or low altitudes, which could have affected the findings (Brenner et al., 2011; Kim et al., 2011). Despite these differences in measurements, it is important to note that, when a low-precision, highly variable outcome consistently has a statistically significant relationship to the area of interest, the underlying relationship might be very strong, which may explain why five of the six studies found an association between altitude and suicide.
Firearms ownership
Three of the articles investigated reported high rates of suicide by firearms, and firearms ownership rates have been shown to be higher in rural areas and Western states with higher elevations (Haws et al., 2009; Betz et al., 2011; Kim et al., 2011). In one study, county elevation was found to be a more important factor than firearm use (Kim et al., 2011). The data, however, suffered from methodologic problems because firearms ownership was based on a self-reported survey and reflected ownership at a state level rather than a county level (Kim et al., 2011). Due to this limitation, every county in a given state was assumed to have the same rate of firearms ownership, despite differences in county elevations and rural and urban settings (Kim et al., 2011). In addition, firearms ownership alone also does not consider storage patterns or efforts to restrict access in case of mental health crises.
Many other studies (although without consideration of altitude) have identified firearms ownership rates as likely determinants of geographic variation in suicide mortality in the United States, largely because firearms have the highest case-fatality rate of any suicide method (85%–90%) (Spicer and Miller, 2000; Miller et al., 2013). None of the studies reviewed considered nonfatal suicide attempts, but considered only completed attempts. The method of suicide attempts has been shown to play a role in the likelihood of death (Spicer and Miller, 2000); so the data could be skewed by an increased completion rate due to the method of attempt.
Population density and rural living
Population density and rural living have also been shown to be major factors in fatal suicides (Searles et al., 2014). The present evaluation of the CDC's WISQARS Fatal Injury Mapping database confirmed this finding (see Fig. 2 and Appendix Table B1) (CDC, 2016). The counties with the highest suicide rates were those in rural areas of South Dakota and Alaska, all at <3200 ft (970 m) and many at or near sea level. This finding accords with one article reviewed, which reported finding a very weak association of high altitude to suicide in the 50 U.S. counties with the highest suicide rates (Kim et al., 2011). In this review, the other important characteristics of these counties were their rural nature and large Native American and Alaskan Native populations. In nationwide all-cause mortality in the United States, suicide is the 10th leading cause of death (Kochanek et al., 2016), but among American Indians and Alaskan Natives, suicide is the second leading cause of death in adults 15–34 years old, and the suicide rate in this age group is 1.5 times higher than the national average (CDC, 2015). This suggests that demographic differences could explain the high suicide rates unrelated to elevation in counties at both low and high altitudes. Another possible explanation is that areas with low population density have barriers to accessing mental health resources in crisis situations or low availability of emergency services, including resuscitation. These findings call into question the leading explanation for higher suicide rates at high altitude offered by four articles reviewed (i.e., chronic hypoxia increases suicide risk) (Haws et al., 2009; Brenner et al., 2011; Kim et al., 2011, 2014).
Hypoxia as a mechanism for higher suicide rates at high altitude
Three of the six reviewed studies hypothesized that the association between altitude and increased suicide rates could be attributed to changes in brain chemistry related to environmental hypoxia (Haws et al., 2009; Brenner et al., 2011; Kim et al., 2014). Serotonin levels decrease, which can lead to depression, and dopamine levels increase, which can lead to impulsive, spontaneous behavior (Trouvin et al., 1986). These conditions can combine to increase suicide risk (Young, 2013). Three of the six studies, although, showed higher suicide risk even at elevations of <4921 ft (1491 m; 2297–4353 ft, 696–1319 m) (Haws et al., 2009; Brenner et al., 2011; Kim et al., 2011). The understanding of high-altitude hypoxia is based on decades-old principles of oxygen transport and the behavior of the oxygen dissociation curve. Oxygen saturation remains higher than 95% until an altitude of 8000 ft (2424 m), and even at this point, measureable decreases in human performance are rarely reported. Thus, it is generally well accepted that, at <4900 ft (1484 m), the physical altitude might change, but the very minor drop in oxygen partial pressure has no discernable effects on the human body (Hackett and Roach, 2012).
Some have suggested, however, that even modest decreases in ambient oxygen availability can change how the brain functions. Shi et al. (2014) demonstrated that brain intracellular pH is higher in healthy subjects at 4500 ft (1361 m) than those at sea level, while others reported finding lower inorganic phosphate and creatine levels in the brains of those living at high altitudes compared to subjects at sea level (Renshaw, 2012). However, to the authors' knowledge, no human studies have demonstrated that neurotransmitter changes or other physiologic changes in the brain at <10,000 ft (3030 m) lead to suicide. Moreover, recent evidence points to thousands of changes occurring at the level of gene transcription during acclimation to hypoxia in animals (Baze et al., 2010) and humans (Chen et al., 2012). Therefore, in addition to the well-known changes in brain physiology at high altitudes (Ainslie and Subudhi, 2014), it is likely that the overall systemic physiological response is extremely complicated. Consequently, changes in one biomarker in one study likely will not offer a significant explanation of what happens in long-term adaptation to high-altitude hypoxia. Clearly, more research is needed before these complex interactions can be linked to clinical outcomes.
Potential effects of high altitude on neurotransmitter release in animal studies
First, it is important to consider that most high-altitude residents in the United States live in the state of Colorado, and of these, 850,000 live at or higher than 7000 ft (2121 m) and only 3350 people live at or higher than 10,000 ft (3030 m) (Dorish, 2012). To the authors' knowledge, no animal studies have been conducted on neurotransmitter production at or <9000 ft (2727 m), where the clear majority of people live and 99% of all reported suicides in the United States have occurred (Betz et al., 2011). Most animal studies showing changes in neurotransmitters (decreasing serotonin levels and rising dopamine levels, along with their precursors and metabolites) have been conducted at elevations of 12,000–25,000 ft (3636–7575 m) (Poncet et al., 1997; Ray et al., 2011), which are much higher than the typical elevations where people live in the United States. Supporting this idea, Prioux-Guyonneau et al. (1982) showed that levels of five HT (a precursor to serotonin) in rats did not change at 5400 ft (1800 m), but did change at 17,160–23,100 ft (5200–7000 m). Therefore, it is unclear that rat studies using simulated altitudes higher than 22,000 ft (6666 m) for 7–14 days are comparable to the human experience of chronic hypoxia associated with living at high altitudes.
Some have suggested that behavioral changes in animals might be a proxy for depression, which can lead to suicide, but research on behavior changes at high altitudes with animal models have returned inconclusive results (Kanekar et al., 2015). Male rats exposed to simulated moderate and high altitude showed no behavior changes. In female rats, no statistically significant differences were seen in some behaviors at all elevations, but small changes did occur in forced swim tests and immobility (a proxy for depression) when comparing sea level to 4500 ft (1363 m), but rose more significantly when female rats were exposed to simulated high altitudes of 10,000 ft (3030 m) (Kanekar et al., 2015). Given these findings, it is difficult to propose that rat studies can serve as a proxy for depression leading to suicidal behavior in humans.
Indeed, some studies have demonstrated links between brief exposure to high altitude in a hypobaric chamber and cognitive changes, reduced vigor, and increased fatigue (Shukitt-Hale et al., 1998; Gerard et al., 2000; Nicolas et al., 2000). However, these studies used small samples of healthy volunteers who had brief exposure to high altitude, to measure the effects of acute hypoxia on outcomes such as cognitive performance (Shukitt-Hale et al., 1998; Nicolas et al., 2000). It is not clear that these earlier studies can be generalized to those living at high altitude, and none of these studies clinically demonstrated significant and ongoing mood changes or depression. In addition, there is a lack of knowledge about the time course of exposure to high altitude in individuals who commit suicide. Any effect of hypoxia likely would be most significant early in adaption to high altitude, but no study has captured data on this factor, which would also be entangled with other potential contributors.
Very little is also known about mood in native populations living at high altitudes, although Ishikawa et al. (2016) showed no increase in depression symptoms in an elderly population living at 12,500 ft (3788 m) in the Himalayas and Tibetan plateau. This is a fertile topic for future research. Unlike native populations, which have lived at high altitudes for generations, many studies have shown possible increases in depression and bipolar disease in a variety of populations living at moderate- to high-altitude settings in the United States and other countries (Gamboa et al., 2011; Asiri, 2014; Huber et al., 2014; Alameda-Palacios et al., 2015). In addition to hypoxia, the suggested causes of these findings include changes in hormone levels and decreased lithium levels in drinking water, as found in some higher elevations, which may lead to higher suicide rates (Helbich et al., 2013). Although not the focus of this article, a detailed review of these studies is warranted to analyze the methodologies used and the altitudes measured.
Some researchers have cited the relative hypoxia seen in smokers and patients with comorbid conditions, such as asthma and chronic obstructive pulmonary disease (COPD), as evidence that hypoxia is the cause of higher depression rates in these groups (Van Den Bemt et al., 2009; Kuo et al., 2010; Aubin et al., 2011; Goodwin et al., 2012a, 2012b; Luger et al., 2014; Zaeh et al., 2016). To the authors' knowledge, no studies have investigated whether comorbid conditions and depression lead to increased suicide rates at high altitude. Toward this question, it is worth noting that many COPD patients use supplemental oxygen and still have high rates of depression (Wilson, 2006; Stapleton and Curtis, 2007). Yu et al. (1999) showed that oxygen therapy was beneficial for pulmonary function in hypoxic patients with sleep apnea, but did little to improve mood. Individuals with asthma experience only intermittent hypoxic episodes, which brings into question whether a significant number of other variables might lead to depression in these conditions.
Conclusions
This integrative review of the current literature confirms that there are higher suicide rate at high altitudes, but the cause of this correlation remains incompletely explained. Suicide victims at high altitudes differ significantly from those at low altitudes in multiple demographic, mental health, and suicide-related characteristics. These other factors, rather than hypoxia, are more likely and more plausible explanations for high suicide rates at high altitudes. Regardless of the cause, clinical professionals at high altitudes should be especially vigilant concerning this public health issue.
Footnotes
Acknowledgment
The authors thank Amanda Bond for her help with constructing the tables and for her clerical support.
Author Disclosure Statement
No competing financial interests exist.
Search Strategy for Medline (Ovid 1946 to present)
| State | County | Elevation-mean (ft) | Elevation-mean (m) | Relative rate—suicide | X times U.S. mean |
|---|---|---|---|---|---|
| Alaska | North Slope | 10 | 3 | 42 | 3.2 |
| Northwest Arctic | 679 | 207 | 87 | 6.7 | |
| Nome | 20 | 6 | 86 | 6.6 | |
| Wade Hampton | 2428 | 740 | 121 | 9.3 | |
| Yukon | 427 | 130 | 63 | 4.8 | |
| Arizona | Fulton | 1100–6001 | 335–1829 | 35 | 2.7 |
| California | Trinity | 2390 | 728 | 45 | 3.5 |
| Colorado | Freemont | 7547 | 2300 | 35 | 2.7 |
| Clear Creek | 6500–9001 | 1981–2744 | 40 | 3.1 | |
| Huerfeno | 6126–9001 | 1867–2744 | 47 | 3.6 | |
| Moffat | 6198–10,001 | 1889–3048 | 38 | 2.9 | |
| Park | 10,500 | 3200 | 35 | 2.7 | |
| Montana | Custer | 3780 | 1152 | 37 | 2.8 |
| Deer Lodge | 4849 | 1478 | 40 | 3.1 | |
| Rosebud | 3115 | 949 | 41 | 3.1 | |
| Nevada | Nye | 5819 | 1774 | 39 | 3 |
| White Pine | 5561 | 1695 | 38 | 2.9 | |
| North Dakota | Sioux | 1634 | 498 | 96 | 7.4 |
| South Dakota | Corson | 2254 | 687 | 106 | 8.2 |
| Shanon | 3200 | 975 | 35 | 2.7 | |
| Todd | 3300 | 1006 | 85 | 6.5 | |
| Tennessee | Benton | 741 | 226 | 39 | 3 |
| De Kalb | 1330 | 405 | 35 | 2.7 | |
| Utah | Grand | 4200 | 1280 | 40 | 3.1 |
| Washington | Skamania | 2007 | 612 | 35 | 2.7 |
Source: CDC (2016).