
Abstract
Abstract
Alarcón-Yaquetto, Dulce E., Lidia Caballero, and Gustavo F. Gonzales. Association between plasma N-acylethanolamides and high hemoglobin concentration in Southern Peruvian highlanders. High Alt Med Biol 18:322–329, 2017.—High-altitude (HA) hypoxia is a stressful condition endured by organisms through different mechanisms. Failing to adapt to chronic HA exposure leads to a disease called chronic mountain sickness (CMS) characterized by excessive erythrocytosis (hemoglobin [Hb] ≥19 g/dL for women and ≥21 g/dL for men). Genes encoding for peroxisome proliferator-activated receptor (PPAR) subunits α and γ have been proposed as candidate genes for HA adaptation. N-acylethanolamides (NAEs) are endogenous fatty acid substances that bind to PPAR-α and -γ. NAEs are also able to modulate the endocannabinoid system, a signaling pathway activated in physiological stressful conditions. In the frame of a metabolomic study, we measured plasma levels of four NAEs: palmitoylethanolamide (PEA), oleoylethanolamide (OEA), stearoyl ethanolamide (SEA), and linoleoyl ethanolamide (LEA) in natives from Puno (3830 m), a city located in the Peruvian Southern Andes, and Lima (150 m). All NAEs were significantly higher in the HA population (p < 0.001, q < 0.001). Subjects with higher NAE values were those with higher Hb concentration and lower pulse oxygen saturation. However, there was no association between NAEs and CMS score. Our results suggest that PEA and OEA could be involved in physiological regulation following long-term HA exposure.
Introduction
H
This disease is strongly associated with inflammation and oxidative stress (Jefferson et al., 2004; Bailey et al., 2013; Julian et al., 2013). It is suggested that chronic diseases such as CMS develop after a sequence of inflammatory signals starting with an alteration in the oxidation/antioxidation balance and ending with the development of the disease.
EE has been described as a preclinical form of CMS and is observed before the appearance of CMS symptoms (Vargas and Spielvogel, 2006; Julian et al., 2013). Therefore, subjects with EE may have higher expression of inflammatory markers than those living at the same altitude but without EE.
Peroxisome proliferator-activated receptors (PPARs) are a family of receptors comprised by three subtypes (α, β/δ, and γ), which altogether control metabolic homeostasis and inflammatory processes (Tyagi et al., 2011).
The PPAR-α gene is inhibited by hypoxia inducible factor (HIF)-1 in mice subject to hypoxia (Narravula and Colgan, 2001) and a putatively advantageous haplotype of this gene is negatively correlated with Hb concentration in the Tibetan population (Simonson et al., 2010).
Palmitoylethanolamide (PEA) and oleoylethanolamide (OEA) are bioactive lipids that bind to PPAR-α (Fu et al., 2003; Lo Verme et al., 2005), PEA might as well work through isoforms β/δ and γ of this receptor (Paterniti et al., 2013). PEA and OEA comprise a family of endogenous substances named the N-acylethanolamides (NAEs).
The Pro12Ala polymorphism that moderately reduces the transcriptional activity of PPAR-γ was more frequent in HA Bolivians (Karasaki and Kashiwazaki, 2005) and in an adapted HA population (Tajik) (Liu et al., 2010) than in their lowland and nonadapted counterparts, respectively. Furthermore, maternal exposure to hypoxia represses the expression of PPAR-γ at HA (Julian et al., 2014) and its altered expression is associated with perinatal complications such as intrauterine growth restriction and preeclampsia (McCarthy et al., 2013), which women from HA are in greater risk to have (Keyes et al., 2003; Levine et al., 2015).
NAEs also influence a novel signaling pathway known as the endocannabinoid system (ECS) comprising cannabinoid receptors 1 and 2 (CB1 and CB2), endogenous ligands (mainly N-arachidonoyl ethanolamide, anandamide), and enzymatic machinery (O'Sullivan 2007; Ahn et al., 2008). Even though NAEs do not bind directly to cannabinoid receptors (Schmid and Berdyshev, 2002), they act on this system through an entourage effect (Lámbert and Di Marzo, 1999), meaning they enhance endocannabinoid signaling and share enzymatic pathways with anandamide (Di Marzo et al., 2005).
There is no extensive literature on the role of the NAEs nor endocannabinoids in conditions of HA hypoxia, especially in HA natives. An activation of the ECS has been reported in athletes suddenly exposed to HA (Feuerecker et al., 2012). OEA plays a specific role in sleep apnea, not only is it higher in patients suffering the disease but OEA levels also correlate with respiratory distress index (Jumpertz et al., 2010), which is a key component in high-altitude (HA) pulmonary edema. Sleep disorders are more severe in people suffering from CMS (Julian et al., 2013; Rexhaj et al., 2016), in fact, sleep disturbances are used as a clinical sign to diagnose CMS (León-Velarde et al., 2005).
Since recent evidence suggests that NAEs bind to PPAR-α and -γ subtypes, we assessed plasma levels of NAEs in natives of Puno (3830 MASL) in the Peruvian Southern Andes and compare them to those from Lima (150 MASL). In addition, we evaluated how NAE levels were associated with Hb, hematocrit (Htc), pulse oxygen saturation (SpO2), and CMS, assessed through the Qinghai score. Thus, we provide novel and important data on the functioning of endogenous bioactive lipids in HA.
Materials and Methods
Settings and design
The study was designed to study metabolomic differences between the HA and low-altitude (LA) population. The HA population studied is set in Puno, at the Southern Peruvian Andes at 3830 MASL. Puno is largely conformed by Aymaran and Quechua descendants. Aymaras are considered an adapted population due to the longer multigenerational time of exposure to HA settings, and therefore, we doubled the number of subjects in HA to increase the odds of studying adapted and nonadapted individuals. The LA population is from the Peruvian capital city Lima (150 MASL), where all ethnic groups are well represented.
Subjects
A total of 100 healthy subjects, men and women, aged 18–61 years were recruited. Eligibility criteria included permanent residence in the place of study for at least 10 years prior the beginning of the study; subjects must have not been taking medication for at least 3 months prior the sample extraction; and have no history of metabolic diseases such as diabetes, systemic arterial hypertension, dyslipidemia, nor metabolic syndrome. Exclusion criteria included pregnancy, and amenorrhea not related to pregnancy or menopause.
Ethics statement
All subjects were informed of the purpose and risks of the study and signed an informed consent form. All procedures were approved by the Institutional Review Board of Universidad Peruana Cayetano Heredia (Project identification code: SIDISI 61697).
Clinical variables and sample extraction
All subjects were weighed and sized to calculate body mass index (BMI). A venous blood sample was extracted in all studied subjects after overnight fasting. Venous blood samples were placed in two tubes containing EDTA to obtain plasma. Trained technicians measured systolic blood pressure (SBP) and diastolic blood pressure (DBP) in sitting position with a sphygmomanometer.
SpO2 was measured with a pulse oximeter (Nellcor N-20, Pleasanton, CA).
Hb concentration was measured with the HemoCue System (Angelholm, Sweden) and Htc was obtained through the microhematocrit procedure.
Assessment of CMS and optimal Hb value
The Qinghai score was used to assess CMS. This score was established by the consensus statement of HA diseases as an adequate method to diagnose CMS (León-Velarde et al., 2005). The test involves the evaluation of the following clinical signs and symptoms: (1) breathlessness, (2) sleep disturbance, (3) cyanosis, (4) vein dilatation, (5) paresthesia, (6) headaches, and (7) tinnitus. The presence and severity of each sign or symptom are scored from 0 to 3, 0 being an indicator of the absence of the sign/symptom. The scores are added and the CMS clinical score is obtained.
EE defined as Hb values equal or over 19 g/dL for women and equal or over 21 g/dL for men added 3 additional points to the score. Finally, the CMS clinical score plus the score obtained by Hb value (0 or 3) make the Qinghai score. CMS is diagnosed with a Qinghai score ≥6.
Metabolite analyses
After the blood samples were extracted and placed in tubes with EDTA, they were centrifuged and the plasma was stored at −80°C before being transported to Metabolon, Inc. (Durham, NC), where a metabolomic profile was conducted. The samples were prepared according to the Metabolon protocol for protein removal prior the insertion of each sample into the liquid chromatography and gas chromatography platforms (Lawton et al., 2008). Compounds were compared to a library of commercially available purified standards. This library currently consists of approximately 4500 named molecules from a wide variety of biochemical classes. Data extraction, metabolite identification, and metabolite quantification were undertaken using Metabolon's proprietary platform.
Data for each compound were normalized by calculating median values; missing values were assumed to be below the limit of detection and imputed with the observed minimum. The concentrations obtained are semiquantitative and expressed in arbitrary units. For this study, we worked with four metabolites related to the ECS pathway: PEA, OEA, stearoyl ethanolamide (SEA), and linoleoyl ethanolamide (LEA).
Statistical analysis
Data were analyzed with Stata version 12. Data are presented as mean ± standard error of the mean. A preliminary Shapiro–Wilk test was used to evaluate normality distribution of the data. If the normality assumption was met, a Student's t-test was used to evaluate differences between populations; otherwise, the Kruskal–Wallis rank sum test was used.
To test if NAE concentrations differed among populations, a two-tailed t-test of the normalized values was used. The ratio of the normalized concentrations of the metabolites within HA natives compared to LA ones was also assessed.
Associations of NAEs and clinical variables, including CMS score, were evaluated through the Pearson correlation test.
A multivariate regression analysis was performed to evaluate the risk of increased Hb value after controlling for age, gender, altitude, BMI, SpO2, and NAEs.
A p < 0.05 and a q < 0.1 were considered statistically significant. The q value describes the false discovery rates in multiple tests. A q value of <0.1 represents high fidelity of the results (Steffens et al., 2010).
Results
Characteristics of population studied
In Lima (LA), 10 women and 20 men were recruited, while 40 women and 30 men were recruited in Puno (HA). Clinical characteristics of subjects according to altitude are shown in Table 1. HA dwellers had significantly higher levels of Hb, Htc, BMI, SBP, and DBP, while pulse oxygen saturation was significantly lower compared to lowlanders.
Values are mean ± standard error of the mean.
Student's t-test.
Kruskal–Wallis test.
BMI, body mass index; DBP, diastolic blood pressure; Hb, hemoglobin; Htc, hematocrit; SBP, systolic blood pressure; SpO2, pulse oxygen saturation.
There were no gender-based differences in BMI, SpO2, and DBP in LA nor in HA (p > 0.05, data not shown), but Hb values were higher in males in both settings. In LA, Hb levels were 12.09 ± 0.09 g/dL for women and 13.50 ± 0.15 g/dL for men (p < 0.0001), while in HA, Hb values were 15.93 ± 0.21 g/dL for women and 17.98 ± 0.27 g/dL for men (p < 0.0001). In addition, only in HA, SBP was significantly higher in males (113.93 ± 1.63 mmHg vs. 107.075 ± 1.41, p = 0.0023).
CMS as defined by the Qinghai score had a prevalence of 12.85% (95% CI 5%–20.6%), but only two subjects (2.85%) had EE.
NAE concentration and relationship with clinical variables
NAE concentrations differed significantly among populations at different altitudes with the higher values found in HA dwellers. A boxplot of normalized NAE values according to altitude is shown in Figure 1 and the ratio of all analyzed metabolites is shown in Table 2.
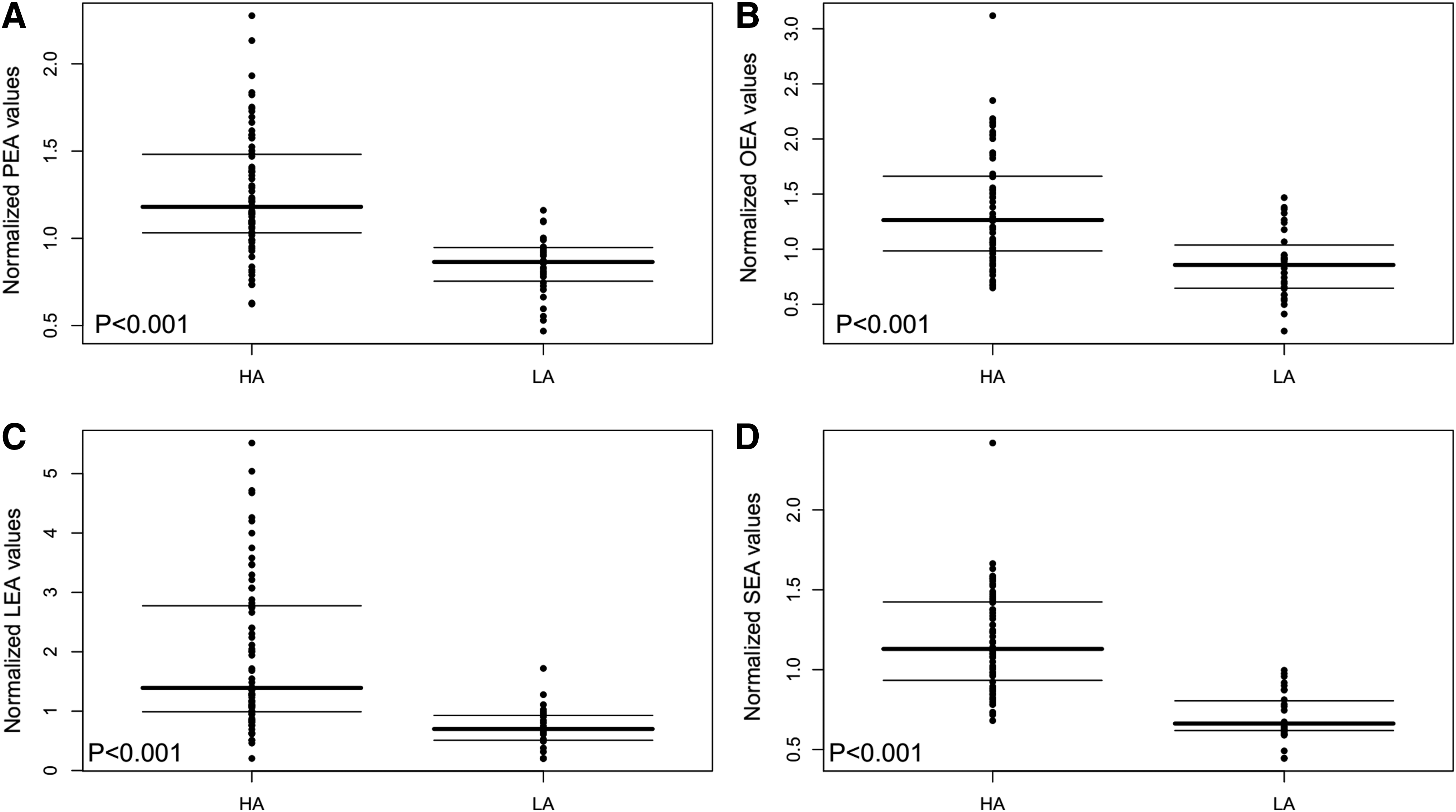
Normalized N-acylethanolamide values in different populations.
Ratio of normalized NAE values in HA subjects compared to LA.
HA, high altitude; LA, low altitude; LEA, linoleoyl ethanolamide; NAEs, N-acylethanolamides; OEA, oleoylethanolamide; PEA, palmitoylethanolamide; SEA, stearoyl ethanolamide.
The analyses of the relationship between NAEs and clinical variables in the whole population (Puno and Lima) show an association between NAEs with age, BMI, Htc, Hb, and SBP in a direct manner, while the relationship with SpO2 is inversely proportional (Table 3).
Pearson correlation coefficient is shown.
Whole: Lima and Puno, n = 100; HA: Puno, n = 70; LA: Lima, n = 30.
p < 0.0001, **p < 0.01, †p < 0.05.
In particular, at HA but not at LA, PEA and OEA correlate with Hb concentration; PEA, OEA, LEA, and SEA correlate with either SBP or BMI. Finally, PEA, LEA, and SEA correlate with age.
There were also gender-based differences in NAE levels but only in HA. All NAEs were significantly elevated in males (PEA p < 0.0001, OEA p = 0.0115, SEA p = 0.0003, LEA p = 0.0007).
Subjects in Puno with low Hb values and high SpO2 were those with NAE concentrations similar to those observed in LA (Fig. 2). We further analyzed the two populations independently, the positive association of all NAEs with Hb, Htc, and SBP remains significant only in the HA population. In fact, no clinical variable analyzed correlates with NAEs in Lima (Table 3).
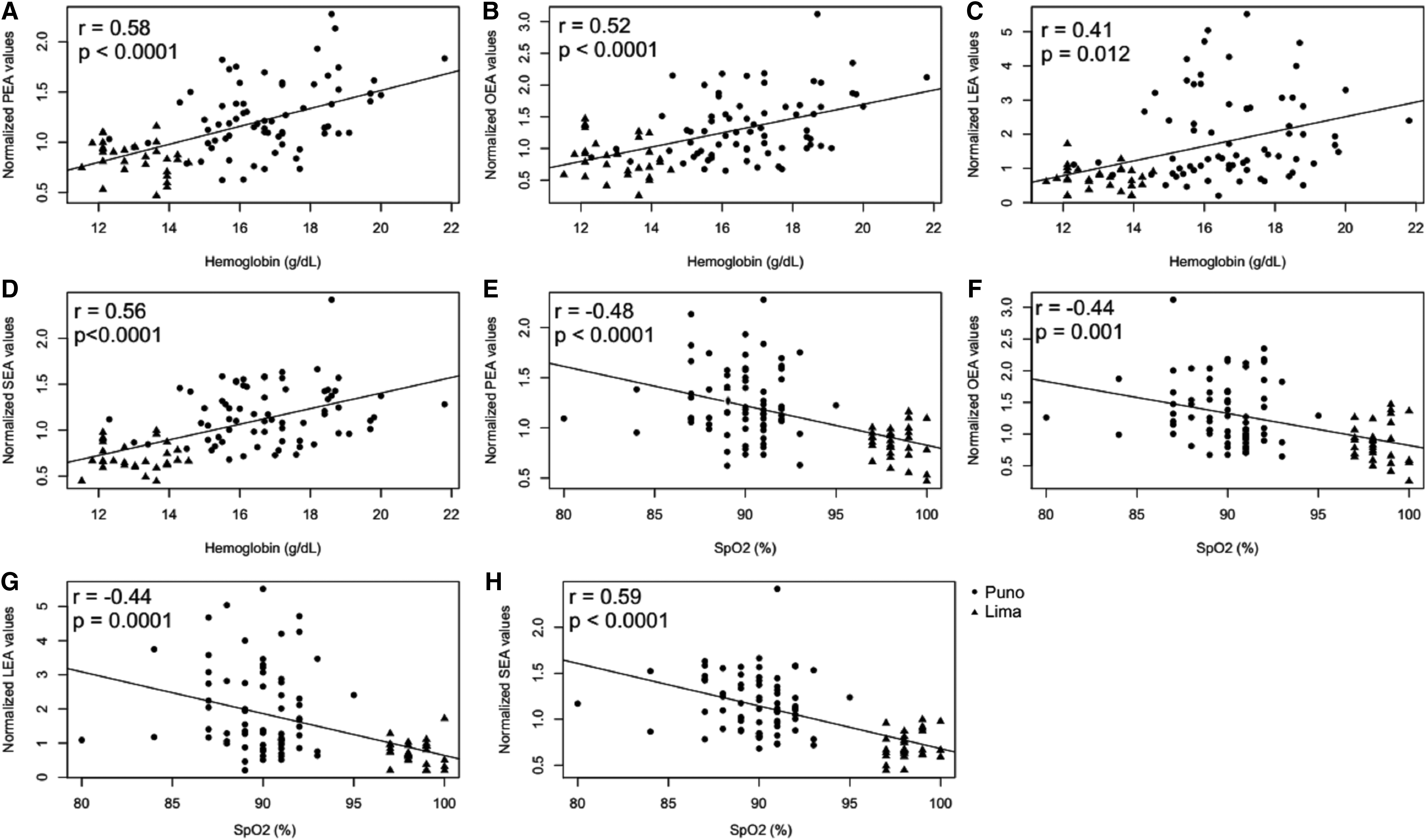
Correlation of hemoglobin with PEA
However, there was no association among PEA, OEA, and LEA with Qinghai score or any of the signs and symptoms evaluated. In fact, Hb and SpO2 did not correlate with any of the items evaluated by the Qinghai score either (Table 4).
Pearson coefficient is shown. No variable was associated with any sign or symptom evaluated in the Qinghai score p > 0.05.
Since these results establish a relationship between Hb and NAEs, we used multiple regression analyses to evaluate the effect of each NAE on changes of Hb concentration (Table 5). PEA and OEA are variables that significantly affect Hb concentration in models corrected by age, gender, BMI, and altitude.
Significant values are shown in bold.
aR2, adjusted R2; β, standard regression coefficient.
Discussion
The present study aimed to evaluate concentration of NAEs in HA natives and compare them to those from lowlanders. The main outcome of our study is the significantly higher concentration of plasma PEA, OEA, LEA, and SEA levels observed in HA dwellers and its relationship with the unique physiological parameters present in these settings.
The relationship between NAEs and several clinical variables is remarkable since it is only observed at HA but not at LA.
Our results demonstrate that at HA, only subjects with high Hb have high NAE values. Samples in both, Lima and Puno, are normally distributed and even using nonparametric statistics, the same pattern was observed. If we observe data from subjects at 3800 m (Puno), only those with increased Hb showed an increase in NAE values. Subjects with low Hb have NAE values as at sea level. Since this study comprised many more subjects from HA than LA, it could be argued that the difference in NAE values is given by the difference in sample size, however, a power analysis between populations showed that size effect does not explain differences in NAE values among groups at low and HA.
The Hb and Htc association remained significant for PEA and OEA when the HA population was studied solely. Age was also significantly correlated to NAEs only in the HA population and this is of significance since older individuals are at greater risk to develop CMS in HA (León-Velarde et al., 1994).
However, after controlling for age in the analyses, the relationship between Hb and PEA or OEA remained. This suggests that hypoxemia is a factor related with increased NAEs particularly PEA and OEA.
The positive association of endocannabinoids and related NAEs with BMI has been previously reported (Engeli et al., 2005; Martins et al., 2015) and is consistent with our findings, but only in the HA population. Obesity was established as a risk factor in the development of CMS (León-Velarde et al., 1994) further enhancing the hypothesis of the role these bioactive lipids play in the pathology of the disease. However, multiple regression analysis was unable to demonstrate associations of BMI with Hb values after several variables were controlled.
Despite plasma NAE levels not being significantly different in people with CMS as defined by the Qinghai score, almost no clinical variable is associated with it, especially EE, and this is in line with previous findings reporting that EE, the hallmark of CMS, is independent of the Qinghai score (Gonzales et al., 2013). This might also explain the inexistent association of NAEs in subjects with CMS diagnosis as defined by this score. It is important to note that some signs and symptoms used in the Qinghai score are not specific to HA chronic exposure and might be displayed in LAs such as tinnitus, headaches, and sleep disturbances. Since the Qinghai score is widely accepted as the best diagnose procedure for CMS, this inexistent relationship should be studied further.
Gender is also an important factor in EE, young males tend to be more prone to suffer EE than females of the same age (Villafuerte and Corante, 2016) and only at HA, males have increased values of all four NAEs studied.
The multiple regression analyses show that PEA and OEA are the two main metabolites that explain the increase in Hb concentration best. Both models presented in Table 5 are controlled by gender.
Our findings provide evidence that NAEs could play a role in the physiological response following HA chronic exposure.
NAEs as well as endogenous cannabinoids are synthesized on demand, but different to classical endocannabinoids, NAEs may show steady-state values (Ottria et al., 2016). There is not much extensive literature on half-life values of NAEs on circulation. Administration of 300 mg of ultramicronized PEA to healthy volunteers doubled plasma basal concentrations after 2 hours, returning to basal levels after 4 hours (Petrosino et al., 2016). Similarly, Gaetani et al. (2003) describe that 60 minutes after the injection of OEA, levels return to baseline.
Their concentration is regulated by synthesizing and degradation enzymes (Whitten et al., 2012). A tonic activation of their receptor regulates biosynthesis (Di Marzo et al., 2000), and therefore, with the polymorphism that reduces the transcriptional activity of PPAR–γ, which is found in HA-adapted population (Karasaki and Kashiwazaki, 2005), there might be lower biosynthesis of NAEs, which is consistent with our findings.
The physiological reasons of the involvement of PEA and OEA in the production of erythrocytes need to be studied further but seem to involve the families of receptors they act upon: subtypes α and γ of PPARs, which are repressed by HIF-1α following acute hypoxic exposure (Narravula and Colgan, 2001) and central and peripheral cannabinoid receptors, which are expressed in hematopoietic cell lines and might be behind hematopoietic differentiation (Jiang et al., 2007).
To the best of our knowledge, this work is the first to assess plasma NAE levels in HA population and to establish a link between the levels on plasma and physiological variables altered in hypoxic conditions. The significance of these findings grows since these endogenous lipids are in charge of homeostatic and metabolic control. Our findings suggest that NAEs, mainly PEA and OEA, could be involved in physiological responses that differentiate healthy highlanders from those who develop CMS, however, further studies should evaluate NAE levels in acutely exposed subjects and in populations with lower multigenerational time exposed to HA.
Conclusion
The concentration of plasma levels of NAEs is considerably higher in individuals chronically exposed to HA compared to lowland counterparts. Increase in Hb in HA dwellers is associated with PEA and OEA levels. Nevertheless, there was no association between NAEs and CMS as defined by the Qinghai score. Our results suggest that high Hb values are independent of this score. In addition, PEA is significantly higher in individuals with nonoptimal Hb concentration and poor pulse oxygen saturation.
Footnotes
Acknowledgments
This work is supported by the Peruvian CONCYTEC/CIENCIACTIVA through the Research Circle of Plants with Effect on Health, grant number 010-2014. CONCYTEC/CIENCIACTIVA had no role in study design, data collection, analyses, and interpretation or in the decision to submit this article for publication. The authors thank all personnel involved in sample and data collection both at Lima (Universidad Peruana Cayetano Heredia) and Puno (Universidad Nacional del Altiplano).
Authors' Contributions
D.E.A.Y. and G.F.G. conceived the study and analyzed the data. G.F.G. supervised fieldwork in Lima, L.C. supervised fieldwork in Puno and participated in fieldwork in Lima, D.E.A.Y. wrote the first draft of the manuscript, and G.F.G. edited the manuscript. All authors revised the final version of the manuscript and agreed on its publication.
Author Disclosure Statement
No competing financial interests exist.