
Abstract
Abstract
West, John B. Are permanent residents of high altitude fully adapted to their hypoxic environment? High Alt Med Biol. 18:135–139, 2017.—Millions of people live permanently at high altitude and many have been there for generations. It is sometimes claimed that these people have completely adapted to their environment, and certainly some remarkable genetic adaptations have recently been described. However there is now strong evidence that permanent residents are not completely adapted to the high altitude in the sense that they have fully compensated for the environmental hypoxia. By sea level standards, highlanders have severe chronic arterial hypoxemia. Furthermore, their maximum oxygen uptake increases if they descend, and recent measurements suggest that cognitive function is reduced in this population compared with a matched group at a lower altitude. Reproductive success is reduced at high altitude because neonatal mortality increases with altitude. The topic has recently gained importance because new technology enables the physiological altitude of permanent residents to be reduced by adding oxygen to the air of buildings on a large scale, a procedure known as oxygen conditioning. Its feasibility has been questioned, but in essence it is no different from air conditioning that is universally used to improve the well-being and productivity of millions of people in hot climates. Oxygen conditioning has the potential to do the same for permanent residents of high altitude.
Introduction
T
A remarkable series of adaptation processes have made it possible for people to live under these severely hypoxic conditions. There is a large literature devoted to these features of acclimatization that include an increase in ventilation and, in most cases, an increase in red cell concentration in the blood. Of particular interest are the remarkable genetic changes that have been described, chiefly in Tibetans, during the last 15 years. For a recent review see Simonson (2015). These changes have occurred relatively rapidly in the evolutionary time scale and indeed some people argue that these genetic changes are some of the fastest that have been seen in humans.
However, despite these remarkable adaptive processes, it is important to appreciate that permanent residents of high altitude continue to be exposed to severe chronic hypoxia. This is highlighted in Table 1 and Figure 1. For example, while the normal alveolar P
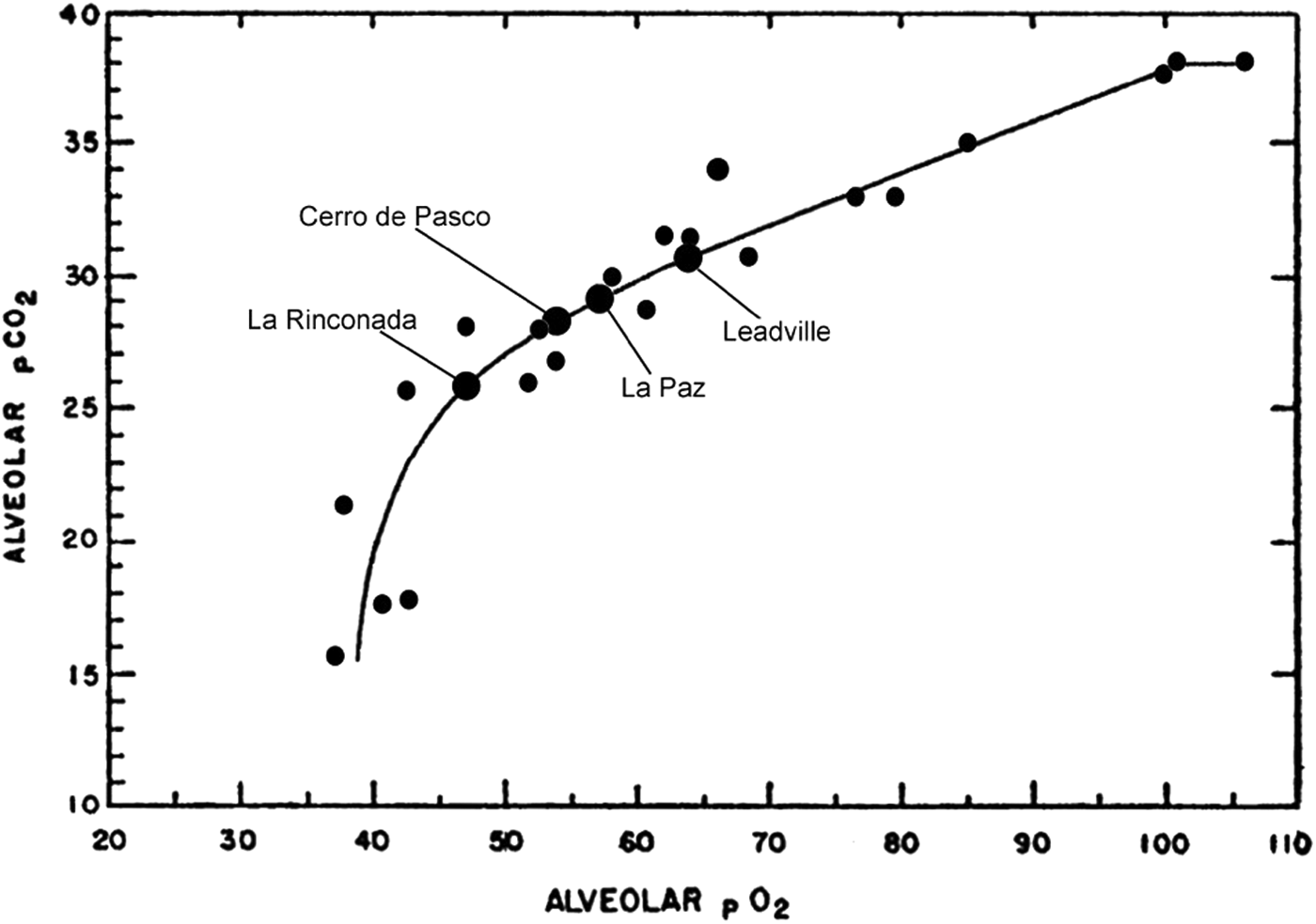
O2-CO2 diagram showing alveolar values for permanent residents of high altitude drawn by Rahn and Otis (1949). The circles show the sources of the data from the many publications on which the line is based, and the original article should be consulted for details of these. The gas exchange values are for a respiratory exchange ratio of 0.85. The locations of four of the highest towns in the world are shown. Note the very low P
The main message of this article is that all permanent residents of high altitude have some reduction of physiological function compared with lowlanders. In fact, this was asserted nearly 100 years ago by the physiologist, Barcroft (1925), who famously stated, “All dwellers at high altitude are persons of impaired physical and mental powers.” By impairment he meant reduced function compared with people who live at or near sea level. However many people refused to accept Barcroft's statement at the time, and there remains today a general belief among some people that permanent residents of high altitude are fully adapted to their environment. One aim of this article is to correct this misunderstanding.
One reason why it is important to appreciate that permanent residents of high altitude have incomplete adaptation to hypoxia is that recent technological advances raise the prospect of artificially reducing the physiological altitude. The result could be an improvement of both physical and mental performance of many permanent residents of high altitude. This technology is oxygen conditioning by which oxygen is added to the air of buildings just as air conditioning modifies its temperature.
Several studies have shown that indeed permanent residents of high altitude have a reduced physical performance because of the altitude, and there is also evidence of neuropsychological impairment.
Physical Ability
Elsner et al. (1964) studied people who lived in Cerro de Pasco and showed that they reduced their maximal oxygen consumption when the inspired gas was changed from sea level air to the P
Another study by Favier et al. (1995) showed that Bolivians living at an altitude of 3600 m corresponding to La Paz developed a significantly higher maximal oxygen consumption when they breathed sea level air. In addition, Cerretelli (1980) plotted VO2max against altitude for three groups of subjects exposed to hypoxia. These were unacclimatized lowlanders, acclimatized lowlanders, and permanent high altitude residents. He found that the values for all three groups lay close to the same line. All these studies support Barcroft's claim that the physical power of permanent residents of high altitude is reduced compared with sea level.
It is hardly surprising that residents of Cerro de Pasco increase their maximal oxygen consumption when they inspire sea level air. As Table 1 shows, the arterial P
Neuropsychological Function
When we turn from the physical to mental powers using Barcroft's terminology, the analysis becomes much more difficult. An index of physical power is relatively easy to obtain from the maximal oxygen consumption. By contrast mental power is much less well defined and certainly much more challenging to measure.
There is now a large literature on neuropsychological function in newcomers to high altitude following the ground-breaking studies of McFarland (1937), and the results are also probably relevant to sojourners, that is, people originally from low altitude who find themselves at high altitude to work. An example of this group for Barcroft was the engineers in the mine at Cerro. However the relevance of this work to permanent residents of high altitude is unclear.
Relatively few measurements of neuropsychological function have been made on permanent residents of high altitude. This is a challenging area of research because of the difficulty of making measurements in matched groups. For example, neuropsychological performance depends very much on the level of education, socioeconomic status, age, and other factors. An alternative strategy is to make repeated measurements on the same group of high altitude residents after moving them to different altitudes, but this procedure has obvious logistical difficulties. Another approach might be to do repeated comparisons in oxygen-enriched rooms and nonenriched rooms to simulate changes in altitude. It would be important to ensure that the subjects were blinded as to the oxygen level.
Nevertheless some measurements have been made. Yan et al. (2011a, 2011b, 2014) studied young adults who were third- or fourth-generation descendants of immigrants to high altitude. The two groups were well matched for ethnicity, age, gender, education, and socioeconomic status. One group was born and raised below 400 m altitude, and the other group was born and raised at altitudes of 2600 to 4200 m until early adulthood. The results showed that the high altitude residents had reduced performance accuracy in a verbal working memory task and longer reaction times in verbal and spatial working memory tasks. In addition, the investigators carried out functional magnetic resonance imaging (fMRI) measurements. These blood oxygen level dependent (BOLD) fMRI studies showed that the high altitude group had decreased activation of some brain regions compared with the low altitude controls. Some of the studies are very technical and the original publications should be consulted for details. To date there have been no studies that contradict these findings.
Another series of neuropsychological studies was carried out on 168 children and adolescents who permanently resided at three altitudes in Bolivia (Hogan et al., 2010). There were three groups of subjects, infants (6–12 months), children (6–10 years), and adolescents (13–16 years). The groups were studied at altitudes of about 500, 2500, and 3700 m. It was reported that there was a reduction in psychomotor speed with increasing altitude as determined by a finger tapping test that measured the number of taps that could be made by the dominant hand in a limited time.
A further study was carried out on 62 Bolivian children living either in La Paz, altitude 3700 m, or in El Alto, altitude 4100 m (Virues-Ortega et al., 2004). It was reported that at the higher altitude, the reduction in neuropsychomotor speed was the same as had previously been measured at 3700 m. However in addition it was shown that executive functions, including complex perceptual skills, reasoning, and verbal fluency, were also reduced by the additional altitude of 400 m. Another study by Rimoldi et al. (2016) showed that schoolchildren from near sea level who moved to La Paz for several years had impaired cognitive function compared with a control group.
Taken together, these measurements strongly suggest that neuropsychological function in permanent residents of high altitude may improve if they move to a lower altitude. Perhaps this is hardly surprising since the P
Reproduction at High Altitude
Successful reproduction is obviously important for a high altitude population. There is much anecdotal evidence that newcomers to high altitude are at a disadvantage. For example, when the women accompanying the Spanish conquerors had children at high altitude South America in the 17th century, it was found that most of the babies did not survive (Monge, 1948). The custom therefore arose for pregnant women to go to low altitude before birth. This is apparently still the case for Han Chinese women who become pregnant in Tibet.
At the present time it is still uncertain whether fertility is reduced in populations living permanently at high altitude (Goldstein et al., 1983). However one negative factor for high altitude populations is clear, that is, the increase of neonatal mortality with altitude (Moore et al., 2001). For example, the incidence of neonatal mortality in the highlands of Peru was reported as about 50 to 60 deaths per thousand live births, that is, about double the rate in the low lands (Mazess, 1965). It was also shown that the high altitude babies in Peru had a lower arterial oxygen saturation as measured by oximetry, a lower Apgar score at 1 minute, and a reduced neurological score 24 hours after birth (Gonzales and Salirrosas, 2005). In another study carried out in Ladakh, India, altitude 3000 m, it was found that neonatal mortality was responsible for 70% to 80% of the total infant mortality and that there was a relationship between the neonatal mortality and altitude (Wiley, 1994).
While the hypoxia of high altitude is an obvious factor in the neonatal mortality, other factors should also be considered. Mothers at high altitude tend to be of a low socioeconomic status, and many births occur in homes that are distant from hospitals where newborns can obtain additional treatment. Mothers are generally reluctant to give birth at high altitude, and they would prefer to descend to a lower altitude, but often this is impossible because of economic factors. An innovation that presumably would reduce this neonatal mortality is to increase the P
The Potential Value of Oxygen Conditioning at High Altitude
It is possible to reduce the physiological altitude by adding oxygen to the inspired air. This was first suggested over 20 years ago where the procedure was known as oxygen enrichment (West, 1995). At that time, the objective was to oxygenate single rooms, and this has become valuable in the number of settings, including dormitories, high altitude minds, high altitude telescopes, and some luxury hotels. A number of condominiums in high altitude ski resorts have had the bedrooms oxygen enriched because many people find that the hypoxia of high altitude is particularly unpleasant during sleep. The oxygen is obtained from atmospheric air by pumping this at high pressure into cylinders containing synthetic zeolite. This preferentially absorbs the nitrogen so that the exiting gas is oxygen enriched. The same technology is used on a small scale in oxygen generators that are now used by the hundreds in homes to deliver oxygen enriched air to patients with chronic lung disease by means of nasal cannulas.
Recently it has been appreciated that the same technology can now be used on a much larger scale to oxygenate whole buildings (West, 2016). As such it shows great potential for helping people at high altitude be they visitors, sojourners, or permanent residents. The procedure can be regarded as analogous to air conditioning, which of course is used on an enormous scale to improve the well-being and productivity of people who live in very hot climates. In the same way, oxygen conditioning has the promise of improving the living and working conditions of people at high altitude. It is not proposed that this technique would be of great value in individual homes at high altitude although this would be possible. However, there are a number of settings where oxygen conditioning would apparently be of considerable value.
Schools
As discussed earlier, studies of children of school age in Bolivia showed that neuropsychological function was reduced as altitude increased (Virues-Ortega et al., 2004; Hogan et al., 2010). Although the results cannot be immediately extrapolated to learning ability, the implication is that reducing the physiological altitude by oxygen conditioning would be beneficial. Another study reached similar conclusions. These children were not permanent residents of high altitude, but they were children from Europe who had moved to La Paz, altitude 3600 m, several years previously. There was clear evidence of some reduction in neuropsychological function compared with a control group of children in Switzerland at low altitude (Rimoldi et al., 2016).
Hospitals
On general principles, it seems reasonable that sick people would be improved if they were supplied with the inspired P
The striking increase in neonatal mortality with altitude was referred to earlier. In this setting, oxygen enrichment of the neonatal wards where newborn babies are being treated would be beneficial. Incidentally oxygen conditioning allows both the mother and baby to be together in an environment with a raised P
Corporate and Business Facilities
High altitude clearly impairs cognitive function of visitors and sojourners, and as discussed above, there is some evidence that this is also the case for permanent residents. Therefore it makes sense to use oxygen conditioning in any environment where important decisions are being made. This would include situations such as legal offices, law courts, banks, department stores, board rooms of corporations, and embassies. To cite one example, the US Embassy in La Paz, Bolivia, is at an altitude of about 3500 m, and several people from the embassy are known to have complained that the altitude made it difficult for them to work effectively and that they were frequently unusually fatigued. It is true that most of the embassy staff are sojourners at high altitude, but there are also permanent residents. By raising the oxygen concentration in the air from 21% to 27%, which is certainly possible by oxygen conditioning, the physiological altitude can be reduced to that of Denver where the altitude of 1600 m is generally easily tolerated.
The cost/benefit ratio of oxygen conditioning on a large scale at high altitude will gradually emerge with further work. However it should be pointed out that the technology of air conditioning and oxygen conditioning have many similar features. In air conditioning, refrigerant gas is compressed in the chiller on a large scale, and the power required is substantial. In oxygen conditioning, atmospheric air is compressed into tubes containing zeolite so that the nitrogen is adsorbed and oxygen-enriched gas is produced. On the face of it, both procedures have many comparable features.
Although the financial aspects of oxygen conditioning need further study, it should be emphasized that air conditioning is used on an enormous scale in the United States. For example, over 90% of new homes in the United States at the present time are now provided with air conditioning. This is because it is recognized that reducing the temperature of the air improves the well-being and productivity of people. The situation at high altitude is similar except that rather than the hot air reducing the well-being and work efficiency, the low P
Footnotes
Author Disclosure Statement
No competing financial interests exist.